

Abstract
Background
Ischaemic stroke interrupts the flow of blood to part of the brain. Haemodilution is thought to improve the flow of blood to the affected areas of the brain and thus reduce infarct size.
Objectives
To assess the effects of haemodilution in acute ischaemic stroke.
Search methods
We searched the Cochrane Stroke Group Trials Register (February 2014), the Cochrane Central Register of Controlled Trials (Issue 1, 2014), MEDLINE (January 2008 to October 2013) and EMBASE (January 2008 to October 2013). We also searched trials registers, scanned reference lists and contacted authors. For the previous version of the review, the authors contacted manufacturers and investigators in the field.
Selection criteria
Randomised trials of haemodilution treatment in people with acute ischaemic stroke. We included only trials in which treatment was started within 72 hours of stroke onset.
Data collection and analysis
Two review authors assessed trial quality and one review author extracted the data.
Main results
We included 21 trials involving 4174 participants. Nine trials used a combination of venesection and plasma volume expander. Twelve trials used plasma volume expander alone. The plasma volume expander was plasma alone in one trial, dextran 40 in 12 trials, hydroxyethyl starch (HES) in five trials and albumin in three trials. Two trials tested haemodilution in combination with another therapy. Evaluation was blinded in 14 trials. Five trials probably included some participants with intracerebral haemorrhage. Haemodilution did not significantly reduce deaths within the first four weeks (risk ratio (RR) 1.10; 95% confidence interval (CI) 0.90 to 1.34). Similarly, haemodilution did not influence deaths within three to six months (RR 1.05; 95% CI 0.93 to 1.20), or death and dependency or institutionalisation (RR 0.96; 95% CI 0.85 to 1.07). The results were similar in confounded and unconfounded trials, and in trials of isovolaemic and hypervolaemic haemodilution. No statistically significant benefits were documented for any particular type of haemodiluting agents, but the statistical power to detect effects of HES was weak. Six trials reported venous thromboembolic events. There was a tendency towards reduction in deep venous thrombosis or pulmonary embolism or both at three to six months' follow‐up (RR 0.68; 95% CI 0.37 to 1.24). There was no statistically significant increased risk of serious cardiac events among haemodiluted participants.
Authors' conclusions
The overall results of this review showed no clear evidence of benefit of haemodilution therapy for acute ischaemic stroke.
These results are compatible with no persuasive beneficial evidence of haemodilution therapy for acute ischaemic stroke. This therapy has not been proven to improve survival or functional outcome.
Keywords: Humans, Acute Disease, Brain Ischemia, Brain Ischemia/complications, Brain Ischemia/mortality, Brain Ischemia/therapy, Combined Modality Therapy, Combined Modality Therapy/methods, Hemodilution, Hemodilution/methods, Hemodilution/mortality, Phlebotomy, Phlebotomy/methods, Plasma Substitutes, Plasma Substitutes/therapeutic use, Randomized Controlled Trials as Topic, Stroke, Stroke/etiology, Stroke/mortality, Stroke/therapy
Plain language summary
Haemodilution for acute ischaemic stroke
Question
We wanted to compare the effectiveness of haemodilution (diluting the blood) treatment, started within 72 hours of stroke onset, versus control or no treatment in people with ischaemic stroke to assess the impact on death or dependence.
Background
Stroke is the second leading cause of death worldwide. Symptoms of stroke include face drooping, arm weakness and difficulty with speech. Most strokes are caused by a blood clot that interrupts blood flow to a part of the brain. If blood flow is not restored quickly, the brain cells will die. Haemodilution improves the flow properties of the blood so that, theoretically, oxygen and nutrient supply to the brain is improved and brain cells threatened to die could survive. This treatment reduces brain infarct (the area of dead cells) size in animals with experimental stroke. Haemodilution can be achieved by blood‐letting (removing blood), by giving fluids as an infusion or by a combination of both. The fluids used may be salt solutions but colloid solutions, which consist of large insoluble molecule meant to retain fluid intravascularly, are more effective as haemodilution agents. In many countries, haemodilution has been used in clinical treatment of people with acute stroke since the 1970s. Since then, a large number of clinical studies on haemodilution in acute stroke have been published. The goal of this review was to determine if blood dilution could prevent death in people with stroke due to blood clots.
Study characteristics
We identified 21 trials involving 4174 adult, male and female participants with presumed acute ischaemic stroke. The evidence is current to February 2014. Many trials followed participants for at least three to six months. Interventions included isovolaemic regimens (replacing a portion of blood volume with fluid) and hypervolaemic regimens (increasing the total volume of blood by adding fluid) using different types of solutions.
Key results
This review showed that, when all the studies are taken together, there is no clear evidence of benefit from haemodilution. There is also no clear evidence that any particular mode of haemodilution, with or without blood‐letting, using various types of haemodiluting agents, etc, is beneficial. There were no significant serious side effects of this treatment. It is concluded that there is no clear scientific support for the use of haemodilution in the routine treatment of people with acute ischaemic stroke.
Quality of the evidence
The overall quality of the evidence was moderate as individual trials were of varying quality. There was little variation among trials.
Summary of findings
Summary of findings for the main comparison. Haemodilution, all types, versus control for acute ischaemic stroke.
| Haemodilution, all types, versus control for acute ischaemic stroke | ||||||
| Patient or population: people with acute ischaemic stroke Settings: Intervention: haemodilution, all types, versus control | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Haemodilution, all types, versus control | |||||
| Mortality at early follow‐up (not later than 28 days) | Study population | RR 1.1 (0.9 to 1.34) | 3866 (16 studies) | ⊕⊕⊕⊝ moderate1 | ‐ | |
| 90 per 1000 | 99 per 1000 (81 to 120) | |||||
| Moderate | ||||||
| 54 per 1000 | 59 per 1000 (49 to 72) | |||||
| Mortality at late follow‐up (3‐6 months) | Study population | RR 1.05 (0.93 to 1.2) | 3957 (15 studies) | ⊕⊕⊕⊝ moderate2 | ‐ | |
| 185 per 1000 | 194 per 1000 (172 to 222) | |||||
| Moderate | ||||||
| 134 per 1000 | 141 per 1000 (125 to 161) | |||||
| Dead or dependent/institutionalised at 3‐6 months | Study population | RR 0.96 (0.85 to 1.07) | 2491 (8 studies) | ⊕⊕⊕⊝ moderate3 | ‐ | |
| 526 per 1000 | 505 per 1000 (447 to 563) | |||||
| Moderate | ||||||
| 539 per 1000 | 517 per 1000 (458 to 577) | |||||
| Venous thromboembolic events at early follow‐up (within 28 days) | Study population | RR 0.83 (0.2 to 3.44) | 621 (4 studies) | ⊕⊕⊕⊝ moderate4 | ‐ | |
| 27 per 1000 | 22 per 1000 (5 to 93) | |||||
| Moderate | ||||||
| 8 per 1000 | 7 per 1000 (2 to 28) | |||||
| Venous thromboembolic events at late follow‐up (3‐6 months) | Study population | RR 0.68 (0.37 to 1.24) | 865 (6 studies) | ⊕⊕⊕⊝ moderate5 | ‐ | |
| 72 per 1000 | 49 per 1000 (27 to 89) | |||||
| Moderate | ||||||
| 37 per 1000 | 25 per 1000 (14 to 46) | |||||
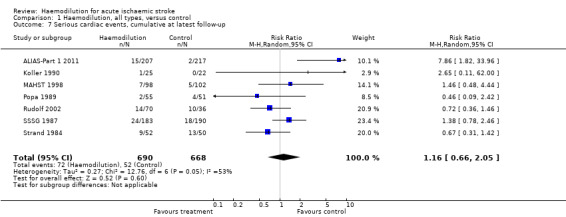
| Serious cardiac events, cumulative at latest follow‐up | Study population | RR 1.16 (0.66 to 2.05) | 1358 (7 studies) | ⊕⊕⊝⊝ low6,7 | ‐ | |
| 78 per 1000 | 90 per 1000 (51 to 160) | |||||
| Moderate | ||||||
| 78 per 1000 | 90 per 1000 (51 to 160) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Four studies lacked or were unclear on blinding of participants and evaluators. Five studies were unclear on randomisation and allocation concealment. However, these risks would be unlikely to increase the effect size. 2 Five studies lacked or were unclear on blinding of participants and evaluators. Five studies were unclear on randomisation and allocation concealment. However, these risks would be unlikely to increase the effect size. 3 Two studies lacked or were unclear on blinding of participants and evaluators. Two studies were unclear on randomisation and allocation concealment. However, these risks would be unlikely to increase the effect size. 4 15 total events. 5 51 total events. 6 One study was unclear on blinding of participants and evaluators. Two studies were unclear on randomisation and allocation concealment. However, these risks would be unlikely to increase the effect size. 7 124 total events.
Background
Description of the condition
Stroke is the second leading cause of mortality and third leading cause of disability worldwide (Lozano 2012). Globally, ischaemic stroke constitutes 68% of all strokes (Krishnamurthi 2013). The median age of stroke is 70 years with an age‐standardised incidence of 3.4 to 5.2 per 1000 (Feigin 2003). As the one‐month case‐fatality rate is 13% to 27% (Feigin 2003), and with limited treatment options, many treatments have been studied, including haemodilution.
Description of the intervention
Haemodilution is usually achieved by infusion of a plasma volume expander with or without concomitant venesection. It may be hyper‐, iso‐ or hypovolaemic, depending on the balance between plasma expansion and venesection. The most commonly used plasma expander in clinical stroke trials has been dextran 40, but hydroxyethyl starch (HES, also called pentastarch) and albumin have also been used.
How the intervention might work
There are several clinical observations suggesting that haemorheological factors have a role to play in acute ischaemic stroke.
People with polycythaemia vera, having very high haematocrit levels, are prone to various thromboembolic complications, including stroke (Pearson 1978).
High haematocrit, even within the 'normal' range, may predict ischaemic stroke (Kannel 1972; Kiyohara 1986), and haematocrit values are significantly higher in people with ischaemic stroke than in matched controls (Harrison 1981; Tohgi 1978). Although this may be a causal relationship, it must be remembered that high haematocrit is related to other cardiovascular risk markers such as hypertension, dyslipidaemia and diabetes (Kiyohara 1986; Lithner 1988).
People with stroke have a variety of haematological abnormalities that may increase whole‐blood viscosity. This includes decreased red cell deformability, increased red cell aggregation, signs of leukocyte activation, elevated fibrinogen and, as a result, high plasma viscosity (Di Perri 1986; Ott 1986; Wood 1985).
When local blood flow to a region of the brain is suddenly interrupted, collateral blood supply may maintain some delivery of oxygen and nutrients, although at a low level, and structural integrity of the neurons is preserved. Intentional haemodilution has been introduced to improve blood flow to hypoperfused but still viable brain areas supplied by collaterals (penumbra). Haemodilution reduces haematocrit and has dual effects: on the one hand, it improves blood flow, on the other hand, it reduces the oxygen‐carrying capacity. The net effect on tissue oxygen supply follows an inverse U‐shaped curve. As haematocrit is reduced, oxygen delivery increases to a peak. When haematocrit is reduced further, oxygen delivery starts to fall (Chien 1981). This has been shown in many peripheral tissues in various species, and there is some support for a similar relationship between haematocrit and oxygen delivery in the human brain (Todd 1994).
When an ischaemic stroke occurs, cerebral autoregulatory mechanisms are impaired (Paulson 1971). In people with brain infarction, intentional haemodilution has been associated with increased flow in the infarcted as well as in the contralateral hemisphere (Hartmann 1987; Vorstrup 1989; Wood 1983). This has also been amply shown in animal models of ischaemic stroke, in which beneficial results of haemodilution on infarct size have been demonstrated (Belayev 2001; Liu 2001). Oxygen‐carrying haemodilutants, such as per fluorocarbon emulsions or diaspirin cross‐linked haemoglobin, have also been used successfully to reduce brain infarct size in animal models (Aronowski 1996; Kline 1991). Other oxygen‐carrying agents of potential use in people with ischaemic stroke include polymerised bovine haemoglobin (Standl 2001).
The optimal haematocrit level for oxygen delivery to the ischaemic brain tissue remains to be determined. Several of the clinical trials reviewed here have been based on experimental data suggesting that haematocrit in the 30% to 33% range provides maximal oxygen delivery to normal peripheral tissues (Chien 1981). However, mathematical modelling based on published observations indicate that oxygen supply in the ischaemic brain penumbra decreases at haemoglobin concentrations below 10 g per 100 mL (Dexter 1997). At the other end of the spectrum, there are several indications that haematocrit levels as high as 40% to 45% provide maximal oxygen delivery to brain tissue (Chien 1981; Kusunoki 1981).
Why it is important to do this review
Systematic investigations of haemodilution in the clinical setting started in the 1960s. Initial clinical experiences of haemodilution without randomisation were encouraging, and suggested clinical benefits from various haemodilution regimens (Gottstein 1976; Gottstein 1981; Korosue 1988; Wood 1982). Haemodilution gained wide acceptance and, in many countries, it became the therapy of choice for people with acute ischaemic stroke. Despite the discouraging results of the randomised trials, as shown in the present review, haemodilution is still occasionally recommended to treat people with acute ischaemic stroke (Popov 2000).
Starting in the late 1960s, several randomised controlled trials (RCTs) of haemodilution treatment in people with acute stroke have been performed. The results have been conflicting. The present formal statistical overview includes the results from 21 independent RCTs of haemodilution in acute ischaemic stroke. Compared with the previous version in 2002, the present update includes three additional trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991). Additions include the 'Risk of bias' tool, reformatting of methods, sensitivity analysis and addition of sections throughout the text.
Objectives
To assess the effects of haemodilution in acute ischaemic stroke.
Methods
Criteria for considering studies for this review
Types of studies
We sought published and unpublished RCTs that compared haemodilution with control. Treatment in control groups varied between trials. Usually, no specific treatment was used, although a protocol involving infusions of crystalloids or dextrose was used in the control group in some trials. Blinding of participants or evaluators has not been a selection criterion (see also below).
We have included only those studies that reported clinical endpoints of direct relevance for participants (death, neurological outcome, functional outcome, need for institutional care, vascular or other events, adverse reactions). Thus, we have not included studies reporting on the effects of haemodilution on cerebral blood flow or other intermediary variables but not providing any other clinical data. We also did not include studies that only included neurological examination scale outcomes because these outcomes could not be combined given the variety of neurological scores (see Types of outcome measures). We have not included studies of haemodilution initiated in the late phase after stroke (i.e. later than one week after onset). We have also not included haemodilution to prevent stroke occurring after carotid surgery.
Types of participants
We only included acute trials with start of treatment within the first 72 hours of stroke onset. Although all trials involved only participants with a clinical diagnosis of presumed ischaemic stroke, some participants in five early trials conducted before computed tomography (CT) became available may actually have had a haemorrhagic stroke (Gilroy 1969; Kaste 1976; Matthews 1976; Popa 1989; Spudis 1973). One study performed CT after treatment and included haemorrhagic stroke (IASSG 1988). Some studies have reported results both on an intention‐to‐treat basis and a per‐protocol ('target group') basis (when participants not treated according to the study protocol have been excluded). If so, the data entered into this review are according to the intention‐to‐treat principle.
Types of interventions
We included trials of hyper‐ and isovolaemic haemodilution. Thus, some trials combined administration of plasma expanders with venesection, but other trials did not. Plasma expanders were plasma alone, low‐molecular‐weight dextran (dextran 40), HES and albumin. No study used a hypovolaemic protocol (i.e. blood‐letting alone). Two studies were confounded (i.e. haemodilution was used together with another treatment modality) (Frei 1987; Kaste 1976) (see Characteristics of included studies table). We did not include studies that compared two haemodilution modalities (e.g. dextran versus HES) as there was no control.
Types of outcome measures
Information on mortality at early (reported to occur within the first seven days in some studies up to 28 days in others) and at late (reported at three to six months) follow‐up was extracted from articles and unpublished reports when available. Since the proportion of participants who become severely dependent on help from other people after stroke may be affected by early death, we used a combined measure (dead or dependent/institutionalised) as a crude measure of functional outcome at three to six months after stroke. Many studies reported on changes in neurological and functional scores. A plethora of scores and measures of distribution were used. Therefore, it has not been possible to report on changes of score sums in a uniform manner. Thromboembolic events (deep venous thrombosis or pulmonary embolism or both) and adverse effects of the haemodilution treatment were reported in a systematic manner only in a few of the trials; these observations are, nevertheless, reported here.
Primary outcomes
Death or dependency/institutionalisation at three to six months.
Secondary outcomes
Mortality in the early (first 28 days) and late (three to six months) phase of stroke.
Venous thromboembolic events in the early (first 28 days) and late (three to six months) phase of stroke.
Serious anaphylactoid reactions.
Serious cardiac events.
Search methods for identification of studies
See the 'Specialized register' section in the Cochrane Stroke Group module. We searched for trials in all languages and arranged translation of relevant papers published in languages other than English.
Electronic searches
We searched the Cochrane Stroke Group Trials Register, which was last searched by the Managing Editor on 18 February 2014. In addition, we searched the following electronic bibliographic databases:
the Cochrane Central Register of Controlled Trials (CENTRAL) (Issue 1, 2014) (Appendix 1);
MEDLINE (Ovid) (January 2008 to October 2013) (Appendix 2);
EMBASE (Ovid) (January 2008 to October 2013) (Appendix 3).
We developed the search strategies for CENTRAL, MEDLINE and EMBASE with the help of the Cochrane Stroke Group Trials Search Co‐ordinator.
Using a comprehensive search strategy, the Cochrane Stroke Group Trials Search Co‐ordinator has already completed a retrospective search of MEDLINE and EMBASE for all stroke trials to December 2007 and added all relevant trials to the Stroke Group Trials Register. To avoid duplication of effort, we have limited the search of these two databases from January 2008 onwards.
Ongoing trials and research registers
We searched the following trials and research registers (February 2014):
ClinicalTrials.gov (www.clinicaltrials.gov/);
EU Clinical Trials Register (www.clinicaltrialsregister.eu);
Stroke Trials Registry (www.strokecenter.org/trials/);
Current Controlled Trials (www.controlled‐trials.com);
World Health Organization (WHO) International Clinical Trials Registry Platform (www.who.int/ictrp/en/).
Searching other resources
In an effort to identify further published, unpublished and ongoing trials, we carried out the following additional searches:
scanned the reference lists of relevant articles;
contacted authors and researchers in the field;
used Science Citation Index Cited Reference Search for forward tracking of important articles.
For the previous version of the review, the review authors:
searched MEDLINE (1966 to June 2002) (Appendix 4);
contacted investigators and manufacturers (Pharmacia and Fresenius) known to be active in trials of haemodilution in an effort to identify additional studies.
Data collection and analysis
Selection of studies
Two review authors (TC and MJ for this update) read the titles and abstracts of the records retrieved from the electronic searches and excluded obviously irrelevant papers. We obtained the full‐text articles of the remaining studies and the same two review authors independently selected studies for inclusion in the review based on the selection criteria described previously. We resolved any disagreements by discussion.
Data extraction and management
In the first version of this Cochrane review, data were independently extracted from published and unpublished articles by two sets of review authors using forms that included all types of outcome events reported. One review author abstracted information from the three trials added in the 2002 update (Bornstein 1981; MAHST 1998; Rudolf 2002). Two review authors abstracted information from the three additional included trials in this 2014 update (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991). We entered the data into Review Manager 5 (RevMan 2012).
Assessment of risk of bias in included studies
We assessed the quality of the included studies according to The Cochrane Collaboration's tool for assessing risk of bias (Higgins 2011). One review author (TC) entered the methodological description to the 'Risk of bias' section in the Characteristics of included studies table. When the description of methods was unclear, TC discussed this with MJ to reach a consensus. The overall risk of bias is summarised in Figure 1.
1.
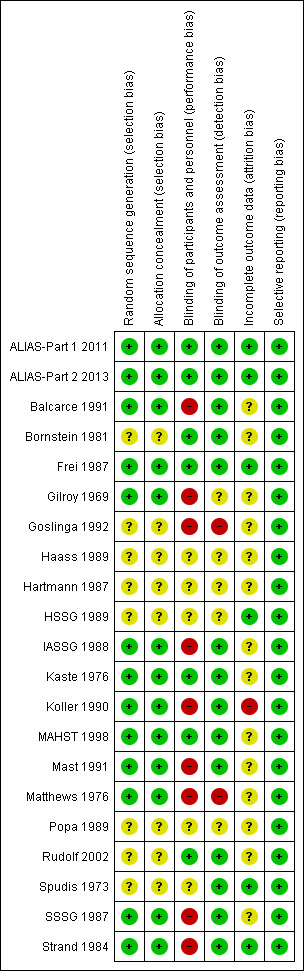
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Measures of treatment effect
We used risk ratios (RRs) and 95% confidence intervals (CI) as the effect measure for all dichotomous outcomes.
Unit of analysis issues
All studies randomised participants into a single arm without cross‐over. Repeated individual measures were managed by defining short‐ and long‐term follow‐up outcomes. Since time points of follow‐up varied greatly between trials, we extracted information for early and late follow‐up. We defined 'early' as day seven to 28 days after onset; if several follow‐ups during this period were reported, we used the one closest to day 21. We defined 'late' as three to six months after stroke; if several time points were reported, we used the one closest to three months.
Dealing with missing data
All studies included the number of events and the total number of individuals for all outcomes. We excluded studies with missing outcome information (e.g. time of death) (Balcarce 1991).
Assessment of heterogeneity
We used the Chi2 test and I2 statistic to test for heterogeneity between trials. The Chi2 test has less power and we considered it significant at a P value of 0.10. An I2 statistic of 50% represented moderate heterogeneity (Higgins 2011).
Assessment of reporting biases
We used funnel plots to investigate reporting biases when 10 or more studies were included in a meta‐analysis outcome. Other reasons, such as heterogeneity and poor methodology, can cause asymmetrical funnel plots.
Data synthesis
We calculated an RR for all outcomes using the Mantel‐Haenszel random‐effects model based on the DerSimonian and Laird's method to calculate the pooled effect size (DerSimonian 1986). We sought data on participants excluded from the analyses after entry into a trial in the published and unpublished reports to allow intention‐to‐treat analyses.
Subgroup analysis and investigation of heterogeneity
We performed subgroup analyses on hypervolaemic haemodilution versus control, isovolaemic haemodilution versus control, haemodilution using low‐molecular‐weight dextran versus control, haemodilution using HES versus control, albumin versus control, unconfounded haemodilution versus control and haemodilution combined with other treatment modalities versus control.
Sensitivity analysis
We performed sensitivity analyses for Analysis 1.1; Analysis 1.2; by removing the largest trial (IASSG 1988), removing the two trials using steroids or glycerol in addition to haemodilution (Frei 1987; Kaste 1976), and removing studies with high risk of performance or detection bias due to lack of blinding.
1.1. Analysis.
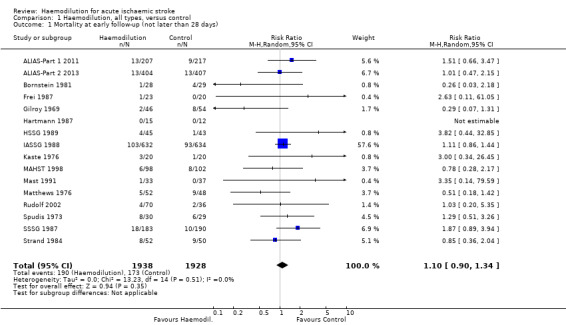
Comparison 1 Haemodilution, all types, versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
1.2. Analysis.
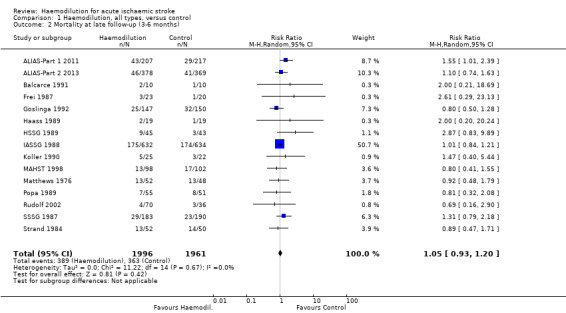
Comparison 1 Haemodilution, all types, versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
Results
Description of studies
See Characteristics of included studies table.
Results of the search
The search of the Cochrane Stroke Group Trials Register identified 266 citations, the searches of MEDLINE and EMBASE in October 2013 identified 2980 citations, and the search of CENTRAL identified 277 citations. After removing duplicate citations (525) and citations that were already referenced in the 2002 update (15), there were 2983 unique citations. We retrieved 14 full‐text articles. For this update, we included three new studies (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991), and excluded 11 studies (Chen 2006; Grauer 1999; Morgenthaler 2010; Shin 2007; Staedt 1987; Staedt 1989; Staedt 1991; Strand 2002; Tessitore 1990; Woessner 2003; Zhang 1990). There are 21 included studies in this review (see Characteristics of included studies table). We did not identify any ongoing trials.
See the PRISMA flow diagram for details of the study selection process for this current update (Figure 2).
2.
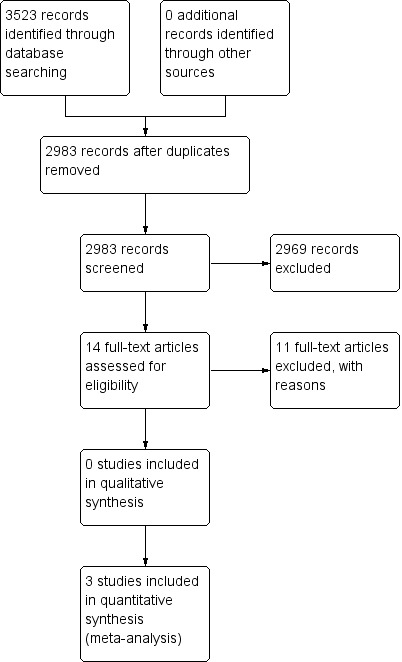
Study flow diagram, showing the results of the searches for this current update.
From the 2002 update, we identified 34 trials with any type of evaluation of haemodilution in people with stroke. Of these, we excluded 15 trials, which were mostly only available as abstracts (Chen 2006; Grauer 1999; Morgenthaler 2010; Schwarz 1998; Shin 2007; Staedt 1987; Staedt 1989; Staedt 1991; Strand 2002; Tessitore 1990; Wang 1990; Wise 1976; Woessner 2003; Zhang 1990; Zhang 1996).
Included studies
We identified 21 independent RCTs of which 18 were published in peer‐reviewed medical journals (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991; Frei 1987; Gilroy 1969; Goslinga 1992; HSSG 1989; IASSG 1988; Kaste 1976; Koller 1990; MAHST 1998; Mast 1991; Matthews 1976; Popa 1989; Rudolf 2002; Spudis 1973; SSSG 1987; Strand 1984). The results of one trial were only partly published but were available to us as a detailed lecture manuscript (Haass 1989), and are included in this review.
The trials used various haemodilution regimens. In the analyses, they were divided into hyper‐ and isovolaemic. In 12 of the trials, the administration of a plasma volume expander was not combined with venesection and was, therefore, defined as hypervolaemic (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Bornstein 1981; Frei 1987; Gilroy 1969; Haass 1989; Hartmann 1987; Kaste 1976; MAHST 1998; Matthews 1976; Rudolf 2002; Spudis 1973). In one study, venesection was performed only if there were signs of volume overload; this trial was also considered as hypervolaemic (HSSG 1989). In the remaining eight studies, the administration of a plasma volume expander was combined with venesection in most of the participants (Balcarce 1991; Goslinga 1992; IASSG 1988; Koller 1990; Mast 1991; Popa 1989; SSSG 1987; Strand 1984). This is operationally called 'isovolaemic haemodilution' in this overview, although in most instances the treatment protocols suggest that the haemodilution was, in fact, slightly or moderately hypervolaemic.
The trials were also subdivided depending on the type of plasma volume expander used. Plasma alone was used in one study (Balcarce 1991), dextran in 12 (Bornstein 1981; Frei 1987; Gilroy 1969; IASSG 1988; Kaste 1976; Koller 1990; Mast 1991; Matthews 1976; Popa 1989; Spudis 1973; SSSG 1987; Strand 1984), HES in five (Haass 1989; Hartmann 1987; HSSG 1989; MAHST 1998; Rudolf 2002), and albumin in three (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Goslinga 1992) (see Characteristics of included studies table).
In two of the trials, haemodilution was combined with other therapies in the intervention group (confounded trials) (Frei 1987; Kaste 1976). In one trial, dexamethasone was used (Kaste 1976), and in the other trial, glycerol was used together with haemodilution (Frei 1987). We performed separate analyses with these two trials since we excluded them to isolate the effects of unconfounded haemodilution.
IASSG 1988 included participants where treatment was started before a CT was performed; 164 of 1215 participants had a haemorrhagic stroke.
Excluded studies
The reasons for excluding studies are given in the Characteristics of excluded studies table.
The most frequent reasons were 1. no details on the intervention were provided (only general descriptions such as 'isovolemic haemodilution' or 'hypervolaemic haemodilution'), 2. neither mortality, functional (activities of daily living (ADL)) outcome nor institutionalisation at follow‐up were reported, 3. providing only neurological outcome and 4. comparing two haemodilution treatments.
We did not obtain access to data from one study in which HES and venesection were tested in approximately 55 participants. This trial was interrupted early for logistic reasons and no information has been available to us, despite written requests and personal contacts with the principle investigator and the manufacturer (Hartmann unpubl.). There are no published trials awaiting assessment.
Risk of bias in included studies
See the Characteristics of included studies table for full 'Risk of bias' assessment for each study.
Sequence generation (selection bias)
Three multicentre trials used centralised randomisation (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; IASSG 1988), eight used closed envelopes to randomise participants (Balcarce 1991; Frei 1987; Gilroy 1969; MAHST 1998; Mast 1991; Matthews 1976; SSSG 1987; Strand 1984), and two used identical looking vials (Kaste 1976; Koller 1990). We considered these 13 RCTs as low risk. Details of the randomisation procedure were missing for eight of the trials (Bornstein 1981; Goslinga 1992; Haass 1989; Hartmann 1987; HSSG 1989; Popa 1989; Rudolf 2002; Spudis 1973).
Allocation
Allocation concealment was low risk for the 13 studies describing their randomisation procedure (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991; Frei 1987; Gilroy 1969; IASSG 1988; Kaste 1976; Koller 1990; MAHST 1998; Mast 1991; Matthews 1976; SSSG 1987; Strand 1984).
Blinding
Seven studies were double‐blinded and low risk (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Bornstein 1981; Frei 1987; Kaste 1976; MAHST 1998; Rudolf 2002). Six additional studies described blinding of evaluators but not blinding of participants (Balcarce 1991; HSSG 1989; Koller 1990; Mast 1991; SSSG 1987; Strand 1984). We considered these studies at high risk of performance bias and low risk for detection bias. Two studies were high risk for bias as they did not blind participants or evaluators (Goslinga 1992; Matthews 1976). Blinding of participants was not possible in studies involving venesection. Information on blinding of participants, medical staff and evaluators was missing in four studies (Haass 1989; Hartmann 1987; HSSG 1989; Popa 1989). One study had high performance bias risk and unclear detection bias risk (Gilroy 1969), while another study had unclear performance bias risk and low detection bias risk (Spudis 1973).
In reports from 14 of the trials, it was clearly stated that blinded evaluators had been used (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991; Bornstein 1981; Frei 1987; IASSG 1988; Kaste 1976; Koller 1990; MAHST 1998; Mast 1991; Rudolf 2002; Spudis 1973; SSSG 1987; Strand 1984), whereas information on blinding was missing in the remaining seven (Gilroy 1969; Goslinga 1992; Haass 1989; Hartmann 1987; HSSG 1989; Matthews 1976; Popa 1989).
Only four trials were truly placebo‐controlled (Bornstein 1981; Frei 1987; Hartmann 1987; Kaste 1976). Participants and managing physicians were not blinded in the trials that involved venesection (Balcarce 1991; Goslinga 1992; HSSG 1989; IASSG 1988; Koller 1990; Mast 1991; Popa 1989; SSSG 1987; Strand 1984).
Incomplete outcome data
Six studies specifically described withdrawals after randomisation and were considered low risk (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Frei 1987; HSSG 1989; Spudis 1973; Strand 1984). The remaining trials did not provide data to address attrition bias.
Selective reporting
Based on the methods and reported results, all included studies were low risk of bias for selective reporting. Funnel plots from analyses with more than 10 studies were symmetrical. Although there was moderate heterogeneity in some analyses (Analysis 1.4; Analysis 1.7; Analysis 3.3), the funnel plots were symmetrical. The funnel plot of Analysis 1.1 is shown in Figure 3 and that of Analysis 3.3 is shown Figure 4. The funnel plots analysed are symmetric despite the fact that some studies are of poor methodology based on the risk of bias tool.
1.4. Analysis.

Comparison 1 Haemodilution, all types, versus control, Outcome 4 Venous thromboembolic events at early follow‐up (within 28 days).
1.7. Analysis.
Comparison 1 Haemodilution, all types, versus control, Outcome 7 Serious cardiac events, cumulative at latest follow‐up.
3.3. Analysis.

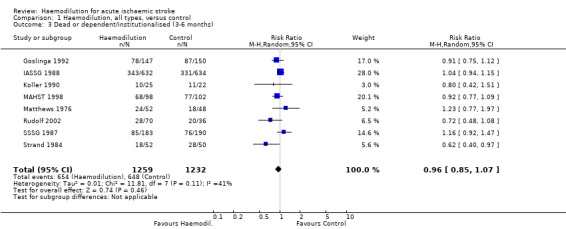
Comparison 3 Isovolaemic haemodilution (including venesection) versus control, Outcome 3 Dead or dependent/institutionalised (3‐6 months).
3.
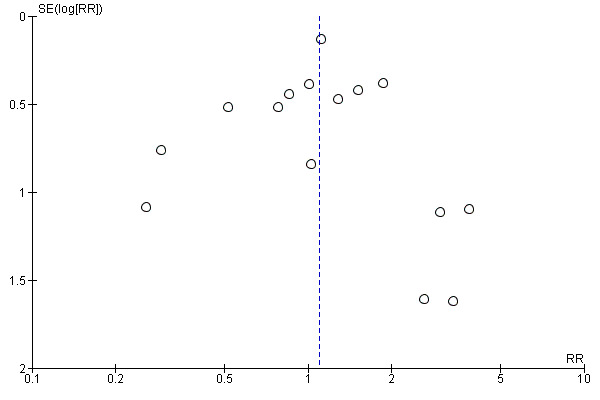
Funnel plot of comparison: 1 Haemodilution, all types, versus control, outcome: 1.1 Mortality at early follow‐up (not later than 28 days).
4.
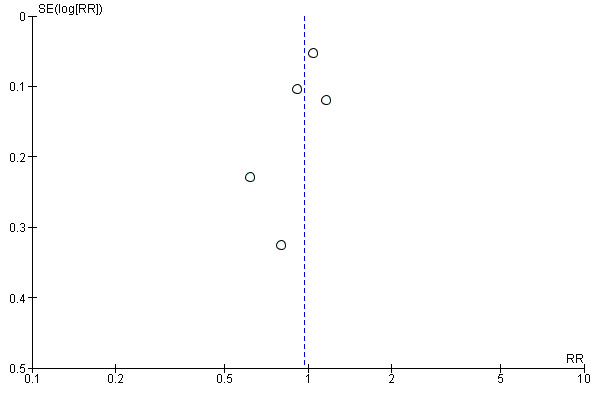
Funnel plot of comparison: 3 Isovolaemic haemodilution (including venesection) versus control, outcome: 3.3 Dead or dependent/institutionalised (3‐6 months).
Other potential sources of bias
The diagnosis of ischaemic stroke was based on CT examinations in 15 trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991; Frei 1987; Goslinga 1992; Haass 1989; Hartmann 1987; HSSG 1989; IASSG 1988; Koller 1990; MAHST 1998; Mast 1991; Rudolf 2002; SSSG 1987; Strand 1984), on bedside diagnosis and findings at autopsy in five trials (see remarks in Characteristics of included studies table), whereas information on diagnostic procedures was missing in one report. Thirteen per cent of IASSG 1988 participants had haemorrhagic stroke as the CT was performed before 48 hours and treatment was initiated within 12 hours.
MAHST 1998 was interrupted early when an interim analysis showed a very low likelihood of reaching statistically significant beneficial effects. ALIAS‐Part 1 2011 was interrupted during interim analysis because 90‐day death rates in participants older than 83 years were 2.3 times higher with albumin compared with saline. Due to this result, the following study excluded participants over 83 years old (ALIAS‐Part 2 2013).
Effects of interventions
See: Table 1
We included 21 studies with 3866 participants. Most studies were small with fewer than 110 participants in 15 of the studies (Balcarce 1991; Bornstein 1981; Frei 1987; Gilroy 1969; Haass 1989; Hartmann 1987; HSSG 1989; Kaste 1976; Koller 1990; Mast 1991; Matthews 1976; Popa 1989; Rudolf 2002; Spudis 1973; Strand 1984). The largest study, the Italian multicentre trial (IASSG 1988), accounted for 33% of all participants and the three largest studies (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; IASSG 1988), accounted for 65% of all participants.
As shown in Analysis 1.4 (P value = 0.09, I2 = 58%); Analysis 1.7 (P value = 0.02, I2 = 59%); and Analysis 3.3 (P value = 0.09, I2 = 50%) there was moderate heterogeneity. No other analyses showed significant heterogeneity.
The four studies published in the years 1969 to 1976 focused on dextran and its action in decreasing platelet and erythrocyte aggregation (Gilroy 1969; Kaste 1976; Matthews 1976; Spudis 1973). Therefore, changes in haemoglobin, haematocrit and whole‐blood viscosity were not reported. No venesection was used, so they constitute hypervolaemic haemodilution regimens. Many of the later trials used a combination of venesection and administration of a plasma volume expander (isovolaemic haemodilution) (Balcarce 1991; Goslinga 1992; IASSG 1988; Koller 1990; MAHST 1998; Popa 1989; SSSG 1987; Strand 1984).
The plasma expander used was plasma alone in one trial (Balcarce 1991), dextran 40 in 12 trials (Bornstein 1981; Frei 1987; Gilroy 1969; IASSG 1988; Kaste 1976; Koller 1990; Mast 1991; Matthews 1976; Popa 1989; Spudis 1973; SSSG 1987; Strand 1984), HES in five trials (Haass 1989; Hartmann 1987; HSSG 1989; MAHST 1998; Rudolf 2002), and albumin in three trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Goslinga 1992). In some of the studies, a standardised, moderately hypervolaemic regimen was used. Other protocols included more aggressive hypervolaemic treatment. Target haematocrit ranged from less than 38% to less than 33%. In three studies, haemodynamic monitoring was used to achieve individually tailored haemodilution and hypervolaemia without increasing the central venous pressure or the pulmonary wedge pressure to intolerable levels (Goslinga 1992; HSSG 1989; Rudolf 2002).
Despite large differences in treatment protocols and target haematocrit levels, the reduction in reported haematocrit was remarkably similar in all trials but for one that reported on haematocrit ranging from 2% to 7% in absolute terms and from 5% to 16% in relative terms (for details, see Asplund 1991 and MAHST 1998).
Haemodilution, all types, versus control
Mortality at early follow‐up (not later than 28 days)
Early mortality was reported in 16 of the 21 studies (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Bornstein 1981; Frei 1987; Gilroy 1969; Hartmann 1987; HSSG 1989; IASSG 1988; Kaste 1976; MAHST 1998; Mast 1991; Matthews 1976; Rudolf 2002; Spudis 1973; SSSG 1987; Strand 1984). In none of them was there any statistically significant effect of haemodilution on survival at early follow‐up.
When the 16 trials were taken together, the RR for death was 1.10 (i.e. somewhat more deaths in the treatment group), with a narrow 95% CI (0.90 to 1.34) (Analysis 1.1), indicating no beneficial effects of haemodilution on early survival. The large Italian multicentre study contributed over half all deaths (IASSG 1988). Therefore, we calculated the RR for survival excluding the Italian study. The RR remained essentially unchanged at 1.08. The mortality rate within each group was lower in the two large albumin trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013) compared with the Italian multicentre study (IASSG 1988). This may have been due to the large albumin trials reporting neurological death within seven days and the Italian study reporting death at discharge.
The two confounded trials involving steroids (Frei 1987) and glycerol (Kaste 1976) were small with 83 included participants (i.e. 2% of the total participant population in the haemodilution trials). Excluding these two trials from the analysis changed the outcome of the formal overview analyses only marginally (RR for early death went from 1.10 to 1.08). Steroids and glycerol are the subject of separate Cochrane reviews (Righetti 2004; Sandercock 2011). Excluding the trials with high risk of performance or detection bias (Gilroy 1969; IASSG 1988; Mast 1991; Matthews 1976; SSSG 1987; Strand 1984), the RR increased to 1.19 (95% CI 0.78 to 1.8).
Case fatality at late follow‐up (three to six months)
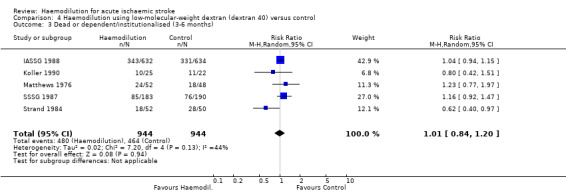
Case fatality was reported at three months in 13 trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Balcarce 1991; Frei 1987; Goslinga 1992; Haass 1989; HSSG 1989; Koller 1990; MAHST 1998; Popa 1989; Rudolf 2002; SSSG 1987; Strand 1984), and at six months in two trials (IASSG 1988; Matthews 1976), whereas no late follow‐up was done in the remaining six trials (Bornstein 1981; Gilroy 1969; Haass 1989; Kaste 1976; Mast 1991; Spudis 1973). In total, there were 752 deaths with equal distribution among haemodiluted and control participants (RR 1.05; 95% CI 0.93 to 1.20) (Analysis 1.2). In none of the individual trials was any statistically significant positive or negative effect on survival at late follow‐up noted.
Excluding the only confounded trial that reported mortality at late follow‐up had very little impact on the overall results, the RR still being 1.05 (Frei 1987). Excluding the Italian study (IASSG 1988), and trials with high risk of performance or detection bias (Balcarce 1991; Goslinga 1992; IASSG 1988; Koller 1990; Matthews 1976; SSSG 1987; Strand 1984), the RR increased to 1.10 (95% CI 0.92 to 1.34) and 1.20 (95% CI 0.94 to 1.53), respectively.
Dead or dependent/institutionalised (three to six months)
The definition of 'dependency' at follow‐up was not uniform between the trials. In this overview, dependency on other people for primary ADL or need for institutional care has been used to indicate poor functional outcome. We used the combined outcome measure of 'dead or dependent/institutionalised' to eliminate the possibility that with more participants dying, the proportion of severely affected people with stroke at follow‐up would be reduced (and vice versa).
The analyses were confined to unconfounded haemodilution trials, since none of the confounded trials reported dependency at late follow‐up.
Sufficient data from eight of the trials were available for estimating the outcome variable 'dead or dependent/institutionalised' (Goslinga 1992; IASSG 1988; Koller 1990; MAHST 1998; Matthews 1976; Rudolf 2002; SSSG 1987; Strand 1984). In one trial, there was a statistically significant effect in favour of haemodilution therapy (Strand 1984), whereas no significant effects were noted in the other trials. In the summary statistics, no beneficial effects of haemodilution emerged (RR 0.96; 95% CI 0.85 to 1.07) (Analysis 1.3). The same conclusion was reached if the analysis was restricted to all trials except IASSG 1988.
1.3. Analysis.
Comparison 1 Haemodilution, all types, versus control, Outcome 3 Dead or dependent/institutionalised (3‐6 months).
ADL performance was followed in detail in five studies (Haass 1989; HSSG 1989; MAHST 1998; Rudolf 2002; SSSG 1987), four of which reported a somewhat better outcome in haemodiluted participants (Haass 1989; HSSG 1989; MAHST 1998; Rudolf 2002), and the fifth (the largest of the trials) reported a better outcome in control participants (SSSG 1987); only in Haass 1989 did the difference in favour of haemodilution treatment reach statistical significance.
Venous thromboembolic events
Four of the studies reported explicitly comparisons of all events of venous thromboembolism in haemodiluted and control participants beyond the first few days (Kaste 1976; MAHST 1998; SSSG 1987; Strand 1984), whereas three studies only reported fatal events (Matthews 1976; Popa 1989; Koller 1990). In one carefully monitored safety study, venous thromboembolism was not mentioned among the adverse events, and it is assumed that no such events occurred during the trial (Rudolf 2002). None of the studies used systematic laboratory screening for thromboembolism in all participants, but the diagnosis was based on clinical presentation, substantiated by laboratory investigations in suspected cases and findings at autopsy. A statistically significant reduction of venous thrombosis, pulmonary embolism or both was reported in one of the studies, and there was a tendency towards reduction in the overview analysis (RR 0.68; 95% CI 0.37 to 1.24) (Analysis 1.5). Notably, this possible beneficial effect was not observed during the acute phase (follow‐up within one month) but only at three to six months' follow‐up.
1.5. Analysis.
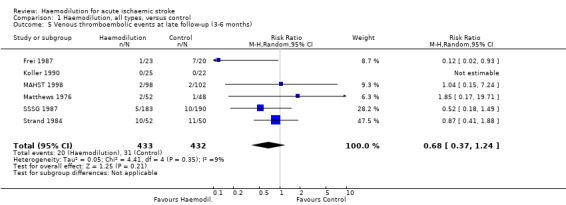
Comparison 1 Haemodilution, all types, versus control, Outcome 5 Venous thromboembolic events at late follow‐up (3‐6 months).
Adverse reactions
None of the studies published before 1984 reported adverse circulatory events. Anaphylactic/anaphylactoid reactions to dextran or HES were reported in six instances among 1136 participants receiving plasma volume expanders (RR versus controls 3.89; 95% CI 0.83 to 18.30) (Analysis 1.6). None of the events were fatal. Such reactions were reported only in trials of dextran (IASSG 1988; Spudis 1973; SSSG 1987; Strand 1984), in which they occurred in 0.6% of the treated participants.
1.6. Analysis.

Comparison 1 Haemodilution, all types, versus control, Outcome 6 Anaphylactic (or anaphylactic‐like) reactions.
Direct comparisons of the number of serious cardiac events, mainly myocardial infarction and acute congestive heart failure, were reported in seven studies (ALIAS‐Part 1 2011; Koller 1990; MAHST 1998; Popa 1989; Rudolf 2002; SSSG 1987; Strand 1984). The total number of reported events was 168 among 1358 participants (12.3%) with an RR of 1.16 (95% CI 0.66 to 2.05) (Analysis 1.7). The Scandinavian multicentre trial reported a significant increase in the number of cardiac events during the treatment period (first five days; odds ratio (OR) 2.64; 95% CI 1.03 to 6.80), but at follow‐up 90 days after stroke the difference in cardiac events between the two groups was no longer significant (OR 1.44; 95% CI 0.76 to 2.73). Myocardial infarction had an OR of 5.15 (95% CI 1.95 to 13.59) in ALIAS‐Part 1 2011. In ALIAS‐Part 2 2013, congestive heart failure was combined with pulmonary oedema and could not be added to this outcome. An excess risk of serious cardiac events was not observed in any of the other trials. The overview analysis of the cumulated number of cardiac events at latest follow‐up (usually three to six months after stroke) indicated no detrimental effects of haemodilution on the risk for serious cardiac events (OR 0.99; 95% CI 0.66 to 1.50).
Subgroups analyses: a word of caution
In the following, the results have been subdivided by mode of haemodilution, type of haemodiluting agent, delay to start of treatment and characteristics of participants treated. It must be emphasised that results of subgroup analyses should be interpreted with caution (even if the individual trials have been testing predetermined hypotheses), in particular when there is no overall effect of the intervention.
Hypervolaemic haemodilution (without venesection) versus control
In 12 trials, the administration of a plasma volume expander was not combined with venesection, or venesection was performed only when signs of volume overload occurred (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Bornstein 1981; Frei 1987; Gilroy 1969; Hartmann 1987; HSSG 1989; Kaste 1976; MAHST 1998; Matthews 1976; Rudolf 2002; Spudis 1973). In four of these trials of hypervolaemic regimens, the number of included participants exceeded 100. In total, 2055 participants were randomised. In the overall analyses, we observed no significant effects on early (RR 0.98; 95% CI 0.68 to 1.40) (Analysis 2.1), or late (RR 1.19; 95% CI 0.94 to 1.51) (Analysis 2.2) mortality or on functional outcome at late follow‐up (RR 0.92; 95% CI 0.74 to 1.14, only three trials (MAHST 1998; Matthews 1976; Rudolf 2002) reporting on this outcome measure) (Analysis 2.3).
2.1. Analysis.
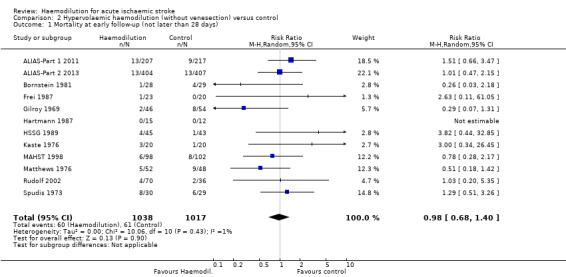
Comparison 2 Hypervolaemic haemodilution (without venesection) versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
2.2. Analysis.
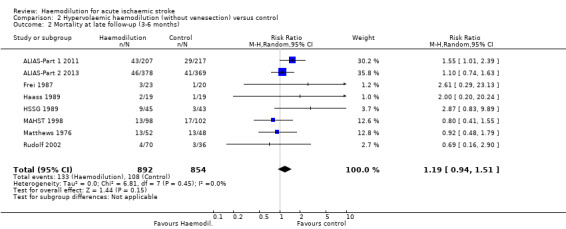
Comparison 2 Hypervolaemic haemodilution (without venesection) versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
2.3. Analysis.

Comparison 2 Hypervolaemic haemodilution (without venesection) versus control, Outcome 3 Dead or dependent/institutionalised (3‐6 months).
Isovolaemic haemodilution (including venesection) versus control
The haemodilution regimens in eight studies were operationally defined as 'isovolaemic', since the administration of a plasma volume expander was combined with venesection (Balcarce 1991; Goslinga 1992; IASSG 1988; Koller 1990; MAHST 1998; Popa 1989; SSSG 1987; Strand 1984). However, in most instances the treatment protocols suggest that the haemodilution was, in fact, slightly or moderately hypervolaemic. The largest trial used 'isovolaemic' haemodilution (IASSG 1988). There were no significant effects on mortality at early (RR 1.15; 95% CI 0.91 to 1.46) follow‐up (Analysis 3.1), late (RR 1.00; 95% CI 0.86 to 1.17) follow‐up (Analysis 3.2), and the proportion dead or dependent/institutionalised at late follow‐up was not affected (RR 0.97; 95% CI 0.83 to 1.13) (Analysis 3.3).
3.1. Analysis.

Comparison 3 Isovolaemic haemodilution (including venesection) versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
3.2. Analysis.

Comparison 3 Isovolaemic haemodilution (including venesection) versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
Different types of plasma expanders used in the haemodilution trials
Four different types of plasma volume expanders, namely plasma alone, low‐molecular‐weight dextran, HES and albumin, have been used in the haemodilution trials. Only one trial used plasma alone in combination with venesection.
Low‐molecular‐weight dextran versus control
Most of the haemodilution trials used dextran 40. In particular, it was used in two (IASSG 1988; SSSG 1987) of the four largest trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; IASSG 1988; SSSG 1987). We observed no significant effects on any of the outcome variables (RR 1.03; 95% CI 0.88 to 1.20 for three‐ to six‐month mortality; Analysis 4.2; RR 1.01; 95% CI 0.84 to 1.20 for death or being dependent/institutionalised at three to six months; Analysis 4.3).
4.2. Analysis.
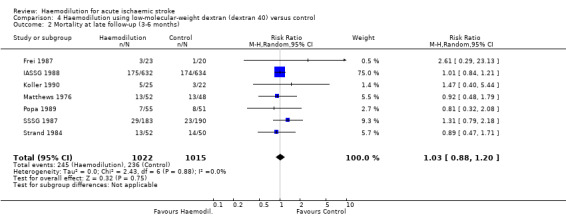
Comparison 4 Haemodilution using low‐molecular‐weight dextran (dextran 40) versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
4.3. Analysis.
Comparison 4 Haemodilution using low‐molecular‐weight dextran (dextran 40) versus control, Outcome 3 Dead or dependent/institutionalised (3‐6 months).
Hydroxyethyl starch versus control
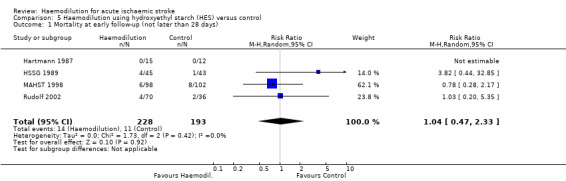
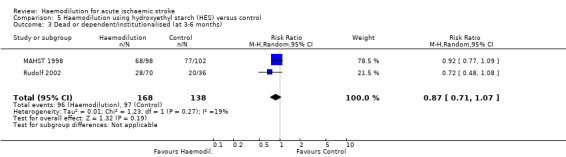
HES, also called pentastarch, was used as the haemodiluting agent in five trials (Haass 1989; Hartmann 1987; HSSG 1989; MAHST 1998; Rudolf 2002), the largest of which included 200 participants (MAHST 1998). Case fatality was not affected at early (RR 1.04; 95% CI 0.47 to 2.33) (Analysis 5.1) or late (RR 1.12; 95% CI 0.57 to 2.19) (Analysis 5.2) follow‐up. Only two studies reported functional outcome. There was a tendency towards better outcome in participants receiving HES than in control participants but the difference did not reach statistical significance (RR 0.87; 95% CI 0.71 to 1.07) (Analysis 5.3).
5.1. Analysis.
Comparison 5 Haemodilution using hydroxyethyl starch (HES) versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
5.2. Analysis.

Comparison 5 Haemodilution using hydroxyethyl starch (HES) versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
5.3. Analysis.
Comparison 5 Haemodilution using hydroxyethyl starch (HES) versus control, Outcome 3 Dead or dependent/institutionalised (at 3‐6 months).
Albumin versus control
Three studies used albumin as a part of the haemodilution regimen (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Goslinga 1992). There were no significant effects on mortality at early follow‐up (RR 1.21; 95% CI 0.69 to 2.12; Analysis 6.1) based on the two ALIAS studies (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013), or late follow‐up (RR 1.12; 95% CI 0.78 to 1.61; Analysis 6.2) based on all three studies (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Goslinga 1992).
6.1. Analysis.

Comparison 6 Haemodilution using albumin versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
6.2. Analysis.

Comparison 6 Haemodilution using albumin versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
Dextran versus hydroxyethyl starch as the haemodiluting agent
In direct comparisons, HES and dextran 40 seem to have similar effects on cerebral blood flow (Hartmann 1987) and plasma viscosity (Haass 1986; Staedt 1986). Two small randomised trials compared clinical outcome in participants with acute ischaemic stroke treated with dextran 40 (Krepp 1984) and HES (Schneider 1985). No overall effect on death or neurological outcome was noted (reviewed in Asplund 1991, data not shown here).
Effects of haemodilution in relation to delay from onset of symptoms to start of treatment
Some of the randomised trials entered participants up to 48 hours or even 72 hours after onset of symptoms. Four trials included only participants within the first six hours of onset of stroke symptoms (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; MAHST 1998; Rudolf 2002), and in five trials, subset analyses of participants included within six hours (IASSG 1988) or 12 hours (Haass 1989; HSSG 1989; Popa 1989; SSSG 1987) of onset of stroke were performed. Two studies showed non‐significant trends in favour of early versus late start of treatment (reviewed in Asplund 1991, data not shown here) (Haass 1989; HSSG 1989). The other three trials did not note such trends. In the large Italian multicentre study, which showed no benefit from haemodilution, all participants were treated within the first 12 hours (IASSG 1988). In this trial, haemodilution had no beneficial effects in participants treated within six hours. Similarly, no statistically significant effects were observed in the Austrian or German multicentre trials that both had a six‐hour upper time limit for inclusion of participants (Austrian trial: MAHST 1998; German trial: Rudolf 2002). However, these two small trials both showed a tendency towards improved functional outcome in HES‐treated participants (see subgroup analysis of HES).
Selection of people for haemodilution
In ischaemic stroke, the pathophysiological mechanisms may differ markedly from person to person. Is it then futile to try a standardised protocol to treat people with acute stroke unless a more precise mechanism is known in each individual person? Could the lack of beneficial effects of haemodilution be explained by detrimental effects in some people, counterbalancing beneficial effects in others?
An extensive subgroup analysis in SSSG 1987 showed similar clinical outcome when participants were subdivided into groups based on easily available clinical criteria, such as sex, age, a cardiac source of embolism, hypertension, heart failure, diabetes and severity of neurological deficits. A similar subgroup analysis was performed in ALIAS‐Part 2 2013, showing no difference based on thrombolysis treatment, demographic characteristics, baseline National Institutes of Health Stroke Scale, stroke onset or baseline imaging.
No beneficial effect of haemodilution was observed in the subgroup with highest haematocrit levels at entry in the Scandinavian (SSSG 1987), the Italian (IASSG 1988), the Romanian (Popa 1989), or the Dutch (Goslinga 1992), trials.
In the HSSG 1989 trial, a significantly better early neurological recovery was noted in participants who were able to increase their cardiac output during haemodilution when compared with participants who failed to do so, whereas outcomes at three months were similar. In SSSG 1987, the outcome was no different in participants with and without a history of cardiac failure (a marker for reduced capacity to increase the cardiac output as a response to haemodilution). Participants with a marked reduction in blood pressure following haemodilution had a similar outcome as participants who maintained their blood pressure.
Only one study addressed the question of the site of the brain lesion (SSSG 1987). Participants with infarcts in deep structures (internal capsule, basal ganglia, thalamus or brain stem) had a significantly higher mortality rate if they had received been haemodilution, whereas mortality rates were the same in treated and control participants if cortical structures were involved.
As described previously, ALIAS‐Part 1 2011 was stopped early due increased 90‐day death rates for albumin versus control in participants older than 83 years. It was hypothesised that the albumin predisposed participants to myocardial stress, which acted in combination with other factors to increase mortality five to 30 days after treatment. Due to this result, the protocol was revised and ALIAS‐Part 2 2013 excluded people older than 83 years old.
Discussion
Summary of main results
When we analysed all the trials together, there were no beneficial effects of haemodilution on mortality at early or late follow‐up or on functional outcome. The largest three studies accounted for two‐thirds of all participants (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; IASSG 1988), and the Italian study accounted for over half of all deaths (IASSG 1988). Sensitivity analysis when removing IASSG 1988 did not alter results. It is reasonable to conclude that haemodilution, as used in the trials conducted so far, has no major beneficial effects on survival or on functional outcome in acute ischaemic stroke.
There was a slight, statistically insignificant, tendency towards more early deaths among haemodiluted participants. The excess mortality observed in participants with deep brain infarctions in one study could be due to chance, but another tentative explanation is that deep brain structures are supplied by end‐arteries and that an adequate collateral blood supply is needed for haemodilution not to be harmful (or beneficial) (SSSG 1987). The significant increase in mortality for participants older than 83 years warranted the interim stopping of ALIAS‐Part 1 2011. However, it must be emphasised that results of subgroup analyses in individual trials should be interpreted with caution even if they are testing predetermined hypotheses, especially when there is no overall effect of the intervention.
These trials used many different modes of haemodilution. The overview analyses showed no positive effects whether the administration of plasma volume expanders was combined with venesection or not (i.e. was iso‐ or hypervolaemic). However, the statistical power to detect differences in the hypervolaemic group was relatively weak.
Low‐molecular‐weight dextran was used as the haemodiluting agent in many of the randomised trials. It has been reported that repeated dextran 40 infusions result in an accumulation of large dextran molecules and an increase in plasma viscosity (Kroemer 1987; Tsuda 1987). It has therefore been claimed that HES or albumin are better choices as plasma volume expanders. However, other studies have shown similar decreases in plasma viscosity with dextran and HES (Haass 1986; Staedt 1986). In people with ischaemic stroke, HES counteracts the increased intracranial pressure (Schwarz 1998). The half‐life of albumin in the circulation is much longer than that of dextran 40 or HES, and the risk for short‐term variations in whole‐blood viscosity is possibly lower.
The total number of participants in the HES trials was small (Haass 1989; Hartmann 1987; HSSG 1989; Mast 1991; Rudolf 2002). In the overview analyses, there was no trend towards improved survival among people treated with HES. However, there was a tendency towards better functional outcome in HES‐treated people, but this was not statistically significant. If this is a true beneficial effect, there may be an interaction with early onset of treatment, since the two HES trials (MAHST 1998; Rudolf 2002) reporting on functional outcome were two of the four haemodilution trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; MAHST 1998; Rudolf 2002) in which all participants were included within the first six hours after stroke onset.
In animal models of stroke, treatment with human albumin markedly increases cortical perfusion, reduces brain swelling and infarct volume, and improves neurological outcome (Belayev 2001; Liu 2001). Albumin was used as the haemodiluting agent in three clinical trials (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Goslinga 1992). There was no statistically significant harm or benefit to albumin although there was a tendency towards harm given the increase in cardiovascular‐related deaths and death in participants older than 83 years (ALIAS‐Part 1 2011).
Whereas no beneficial effects on mortality or functional dependency were documented in the formal overview analyses, there was a tendency towards significant reduction of the risk for venous thromboembolic events in participants who had received haemodilution. This is in line with the prophylactic effects of dextran against deep venous thrombosis and pulmonary embolism after major surgery. However, the results of the overview analysis must be interpreted with caution. The CIs were wide. The diagnosis of a deep vein thrombosis was based on clinical presentation and findings at autopsy. It seems that, in most instances, the clinicians making the diagnosis were not blinded as to which group the participant had been assigned. It is remarkable that the effect was most evident at late follow‐up (three to six months), making it unlikely that dextran, HES or albumin had any specific effect on the risk of venous thromboembolism. It may be speculated that low haematocrit in people who have undergone venesection reduces the risk of deep venous thrombosis and pulmonary embolism to some extent even after the acute phase of stroke.
There has been concern that many haemodilution regimens may involve a risk of volume overload in people with stroke with incipient or manifest heart failure. Cardiovascular events (ALIAS‐Part 1 2011) and cardiopulmonary events (ALIAS‐Part 2 2013) were more common in albumin‐treated participants in the ALIAS trials. Haemodynamic monitoring with a Swan‐Ganz catheter during the haemodilution procedure has been introduced to reduce the risk of left ventricular failure during hypervolaemic haemodilution (Goslinga 1992; HSSG 1989). The overview analysis of trials reporting cardiovascular events in a systematic manner, did not document any major increase in adverse circulatory events in participants who had received haemodilution (Goslinga 1992; HSSG 1989). The number of anaphylactic or anaphylactoid reactions was small and was reported in less than 1% of all participants receiving plasma volume expanders. Pretreatment with hapten‐dextran was used in three of the studies (IASSG 1988; Koller 1990; SSSG 1987), and this may have reduced the risk of anaphylaxis to dextran.
Overall completeness and applicability of evidence
Our objective was to evaluate the efficacy of haemodilution therapy in people with acute ischaemic stroke. We have identified relevant randomised trials investigating a variety of haemodilution strategies including plasma, dextran, HES and albumin with or without venesection for acute ischaemic stroke. The results are applicable to people meeting trial inclusion and exclusion criteria. As the inclusion criteria included people with presumed ischaemic stroke, 164 participants from IASSG 1988 had haemorrhagic stroke identified after treatment and five additional studies were performed before CT was available to rule out haemorrhagic stroke (Gilroy 1969; Kaste 1976; Matthews 1976; Popa 1989; Spudis 1973).
We have searched comprehensively the Cochrane Stroke Group Trials Register up to February 2014. This register contains all stroke trials from MEDLINE and EMBASE to December 2007. We searched MEDLINE and EMBASE from 2008 to October 2013, and CENTRAL up to Issue 1, 2014. It could have been possible to re‐search all of MEDLINE and EMBASE from 2002, but relevant stroke trials were included in the Cochrane Stroke Group Trials Register before December 2007 and the current search results had already returned 2983 citations.
The 21 studies included in this analysis are sufficient to address the objective. There are improvements that could be made.
There are likely to be more methods used for haemodilution, such as venesection plus plasma replacement, which were only studied in one randomised trial (Balcarce 1991). Additional subgroups based on treatments other than haemodilution, such as thrombolysis (ALIAS‐Part 2 2013), could have been included in more studies. ALIAS studies reported neurological death within seven days, which was included in the early mortality data (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013). Death from any cause was reported at 30 days, but was not included in the 28‐day cut‐off for early mortality. Additional outcomes, especially serious adverse events, could have been included in more studies.
We acknowledge there are excluded studies that meet eligibility criteria (based on types of studies, participants and interventions), but do not have relevant or appropriate outcomes. These outcomes included haematological values, laboratory values, imaging and neurological score. Haematological and laboratory values, considered as intermediary outcomes, may not correlate well with the clinical outcomes of interest. Only one excluded study reported imaging outcomes (Shin 2007). Clinical neurological scores were relevant outcomes but could not be combined in a meta‐analysis given the wide variety of scores used. Ideally, neurological score changes would be combined for analysis to measure more fine‐grained differences in outcomes. Unfortunately, this was not feasible given the variety of scoring methods and time points of evaluation. Although there may have been benefit or harm for neurological outcome after haemodilution therapy, this meta‐analysis does show that haemodilution therapy has no benefit for the clinical outcome of mortality.
Current practice of haemodilution in acute ischaemic stroke is likely to vary within and across countries. While older studies occasionally recommend haemodilution (Popov 2000), the American Heart Association does not recommend haemodilution based on the 2002 version of this review (Jauch 2013). Other guidelines, do not comment on haemodilution (ESO 2008; NICE 2008).
Quality of the evidence
There were 21 included studies consistently showing an inability to reject the null hypothesis of haemodilution treatment in acute ischaemic stroke having no harm or benefit. Using the GRADE system, the quality of evidence was moderate for outcomes including all haemodilution therapies, except for cardiac events, which was considered low (Table 1). There was little heterogeneity with only three analyses showing moderate heterogeneity (Analysis 1.4; Analysis 1.7; Analysis 3.3). All funnel plots were symmetrical.
Using the 'Risk of bias' tool, there were eight studies with more than three unclear categories as the information was not reported (Bornstein 1981; Goslinga 1992; Haass 1989; Hartmann 1987; HSSG 1989; Popa 1989; Rudolf 2002; Spudis 1973). Nine other studies had a high risk of performance or detection bias because the participants or evaluators or both were not blinded (Balcarce 1991; Gilroy 1969; Goslinga 1992; IASSG 1988; Koller 1990; Mast 1991; Matthews 1976; SSSG 1987; Strand 1984). These studies were unable to blind the interventions. Other study interventions were able to blind the intervention and control arm. Only six studies specifically reported on the number of participants who were withdrawn after randomisation making them at low risk of incomplete outcome bias (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013; Frei 1987; HSSG 1989; Spudis 1973; Strand 1984). Eight studies did not describe the randomisation procedure (Bornstein 1981; Goslinga 1992; Haass 1989; Hartmann 1987; HSSG 1989; Popa 1989; Rudolf 2002; Spudis 1973). All studies had low risk of reporting bias.
Potential biases in the review process
We attempted to reduce bias by performing a comprehensive literature search without language restrictions. The review authors of previous versions contacted authors for published and unpublished data. We did not contact the authors of the two studies included in this version as these studies were well documented (ALIAS‐Part 1 2011; ALIAS‐Part 2 2013). Other citations that we did and did not receive full text on could have had unpublished data relevant to this review. Unfortunately, we were unable to contact them all. The subgroup analysis should also be interpreted with caution, as this is a post‐hoc analysis.
Agreements and disagreements with other studies or reviews
This review and previous versions are the most recent systematic review of haemodilution in acute ischaemic stroke. In an early systematic review of haemodilution trials in acute stroke (Asplund 1991), it was shown that, despite large differences in treatment protocols and target haematocrit levels, the reduction in haematocrit was remarkably similar, ranging from 4% to 7% in absolute terms and from 9% to 16% in relative terms in all but one study (Koller 1990), in which the reduction in haematocrit was more pronounced. In the only trial reporting on the change of haematocrit, haemodilution by HES and without venesection reduced haematocrit by 2% in absolute and by 5% in relative terms (MAHST 1998).
Non‐systematic reviews of acute ischaemic stroke therapies including neuroprotection (Ginsberg 2008) and albumin (Prajapati 2011) have been published. Ginsberg 2008 discusses haemodilution trials referenced in this review. Both reviews discuss the promise of albumin therapy, but these reviews were completed while the ALIAS studies were underway.
Authors' conclusions
Implications for practice.
As shown in the International Stroke Trial, intentional haemodilution has until recently been widely used in some countries to treat people with acute ischaemic stroke (International Stroke Trial Collaborative Group, personal communication). The present systematic review shows that this clinical practice has no clear scientific support. No benefit of haemodilution on mortality or on functional outcome in survivors has been documented, and the overall results of this review showed no clear evidence of benefit of this therapy. This conclusion concerns both hyper‐ and isovolaemic haemodilution regimens and all types of haemodiluting agents used (dextran, hydroxyethyl starch and albumin). Haemodilution for acute ischaemic stroke should not be used outside of clinical trials with the possible exception of people with severe polycythaemia.
Implications for research.
In most participants included in the trials reviewed here, haemodilution treatment has been initiated later than six hours after onset of stroke symptoms and there has been a considerable additional delay before a significant reduction of haematocrit levels have been achieved. However, the available data from participants treated by isovolaemic and hypervolaemic haemodilution within six hours do not provide support for another large‐scale clinical trial of this treatment. There is growing support from animal experimental models of ischaemic stroke that haemodilution initiated within the first few hours may limit brain infarct size and improve neurological outcome. While there was promise for albumin therapy, the large ALIAS trials enrolled participants within five hours of stroke onset and did not show benefit, suggesting that future clinical trials using albumin would have less clinical equipoise. The development of new oxygen‐carrying haemodilutants and neuroprotectant agents is interesting. New clinical trials are warranted only if the balance between beneficial effects and adverse reactions of new modes of haemodilution have been solidly documented in experimental stroke models.
What's new
| Date | Event | Description |
|---|---|---|
| 29 April 2014 | New citation required but conclusions have not changed | New review author team completed this update |
| 9 March 2014 | New search has been performed | Compared with the previous version of the review, this update includes three additional randomised trials and uses random‐effects risk ratios instead of fixed‐effect odds ratios. The review now includes 21 trials involving 4174 participants. Other additions include the 'Risk of bias' tool, reformatting of methods, sensitivity analyses, and new sections throughout the text |
History
Protocol first published: Issue 2, 1995 Review first published: Issue 2, 1995
| Date | Event | Description |
|---|---|---|
| 25 August 2008 | Amended | Converted to new review format. |
| 14 August 2002 | New search has been performed | Compared to the previous version, this update includes two additional randomised trials (of which one is not yet published), a plain language summary has been added, more background information is provided and an additional end‐point (cardiac adverse effects) is presented. |
Acknowledgements
See Sources of support.
Appendices
Appendix 1. Cochrane Central Register of Controlled Trials (CENTRAL) search strategy
1. [mh ^"cerebrovascular disorders"] or [mh "basal ganglia cerebrovascular disease"] or [mh "brain ischemia"] or [mh "carotid artery diseases"] or [mh"intracranial arterial diseases"] or [mh "intracranial embolism and thrombosis"] or [mh "intracranial hemorrhages"] or [mh ^stroke] or [mh "brain infarction"]
2. (stroke* or apoplex* or cerebral vasc* or cerebrovasc* or cva):ti,ab
3. ((brain or cerebr* or cerebell* or vertebrobasil* or hemispher* or intracran* or intracerebral or infratentorial or supratentorial or middle next cerebr* or mca* or anterior next circulation) near/5 (ischemi* or ischaemic* or infarct* or thrombo* or emboli* or occlus* or hypoxi*)):ti,ab
4. ((brain* or cerebr* or cerebell* or intracerebral or intracran* or parenchymal or intraventricular or infratentorial or supratentorial or basal next gangli* or putaminal or putamen or posterior next fossa) near/5 (haemorrhage* or hemorrhage* or haematoma* or hematoma* or bleed*)):ti,ab
5. #1 or #2 or #3 or #4
6. [mh ^hemodilution]
7. [mh ^"plasma exchange"] or [mh "plasma substitutes"]
8. [mh ^"blood substitutes"]
9. [mh ^hetastarch] or [mh ^dextrans] or [mh ^polygeline] or [mh ^povidone] or [mh albumins] or [mh ^"sodium chloride"] or [mh ^"saline solution, hypertonic"] or [mh colloids]
10. [mh ^phlebotomy] or [mh ^bloodletting]
11. (hemodilut* or haemodilut*):ti,ab
12. (plasma near/3 (expand* or expansion or exchange* or substitut* or replace*)):ti,ab
13. (blood near/3 (expand* or expansion or exchange* or substitute* or replace* or remov* or dilut*)):ti,ab
14. (hetastarch or pentastarch or hydroxyethylstarch or "hydroxyethyl‐starch" or dextran* or polygeline or povidone or albumin or saline or colloid*):ti,ab
15. (phlebotomy or bloodletting or "blood‐letting" or venesection or venipuncture):ti,ab
16. {OR #6‐#15}
17. #5 and #16
Appendix 2. MEDLINE (Ovid) (January 2008 to October 2013) search strategy
1. cerebrovascular disorders/ or exp basal ganglia cerebrovascular disease/ or exp brain ischemia/ or exp carotid artery diseases/ or exp intracranial arterial diseases/ or exp "intracranial embolism and thrombosis"/ or exp intracranial hemorrhages/ or stroke/ or exp brain infarction/
2. (stroke$ or apoplex$ or cerebral vasc$ or cerebrovasc$ or cva).tw.
3. ((brain or cerebr$ or cerebell$ or vertebrobasil$ or hemispher$ or intracran$ or intracerebral or infratentorial or supratentorial or middle cerebr$ or mca$ or anterior circulation) adj5 (isch?emi$ or infarct$ or thrombo$ or emboli$ or occlus$ or hypoxi$)).tw.
4. ((brain$ or cerebr$ or cerebell$ or intracerebral or intracran$ or parenchymal or intraventricular or infratentorial or supratentorial or basal gangli$ or putaminal or putamen or posterior fossa) adj5 (haemorrhage$ or hemorrhage$ or haematoma$ or hematoma$ or bleed$)).tw.
5. 1 or 2 or 3 or 4
6. hemodilution/
7. plasma exchange/ or exp plasma substitutes/
8. blood substitutes/
9. hetastarch/ or dextrans/ or polygeline/ or povidone/ or exp albumins/ or sodium chloride/ or saline solution, hypertonic/ or exp colloids/
10. phlebotomy/ or bloodletting/
11. (hemodilut$ or haemodilut$).tw.
12. (plasma adj3 (expand$ or expansion or exchange$ or substitut$ or replace$)).tw.
13. (blood adj3 (expand$ or expansion or exchange$ or substitute$ or replace$ or remov$ or dilut$)).tw.
14. (hetastarch or pentastarch or hydroxyethylstarch or hydroxyethyl‐starch or dextran$ or polygeline or povidone or albumin or saline or colloid$).tw.
15. (phlebotomy or bloodletting or blood‐letting or venesection or venipuncture).tw.
16. or/6‐15
17. 5 and 16
18. Randomized Controlled Trials as Topic/
19. random allocation/
20. Controlled Clinical Trials as Topic/
21. control groups/
22. clinical trials as topic/ or clinical trials, phase i as topic/ or clinical trials, phase ii as topic/ or clinical trials, phase iii as topic/ or clinical trials, phase iv as topic/
23. double‐blind method/
24. single‐blind method/
25. Placebos/
26. placebo effect/
27. Therapies, Investigational/
28. Research Design/
29. randomized controlled trial.pt.
30. controlled clinical trial.pt.
31. (clinical trial or clinical trial phase i or clinical trial phase ii or clinical trial phase iii or clinical trial phase iv).pt.
32. random$.tw.
33. (controlled adj5 (trial$ or stud$)).tw.
34. (clinical$ adj5 trial$).tw.
35. ((control or treatment or experiment$ or intervention) adj5 (group$ or subject$ or patient$)).tw.
36. (quasi‐random$ or quasi random$ or pseudo‐random$ or pseudo random$).tw.
37. ((control or experiment$ or conservative) adj5 (treatment or therapy or procedure or manage$)).tw.
38. ((singl$ or doubl$ or tripl$ or trebl$) adj5 (blind$ or mask$)).tw.
39. (coin adj5 (flip or flipped or toss$)).tw.
40. placebo$.tw.
41. controls.tw.
42. or/18‐41
43. 17 and 42
44. stroke volume/ or stroke volume.tw.
45. 43 not 44
46. exp animals/ not humans.sh.
47. 45 not 46
Appendix 3. EMBASE (Ovid) (January 2008 to October 2013) search strategy
1. cerebrovascular disease/ or basal ganglion hemorrhage/ or exp brain hematoma/ or exp brain hemorrhage/ or exp brain infarction/ or exp brain ischemia/ or exp carotid artery disease/ or cerebral artery disease/ or cerebrovascular accident/ or occlusive cerebrovascular disease/ or stroke/
2. stroke patient/ or stroke unit/
3. (stroke$ or apoplex$ or cerebral vasc$ or cerebrovasc$ or cva).tw.
4. ((brain or cerebr$ or cerebell$ or vertebrobasil$ or hemispher$ or intracran$ or intracerebral or infratentorial or supratentorial or middle cerebr$ or mca$ or anterior circulation) adj5 (isch?emi$ or infarct$ or thrombo$ or emboli$ or occlus$ or hypoxi$)).tw.
5. ((brain$ or cerebr$ or cerebell$ or intracerebral or intracran$ or parenchymal or intraventricular or infratentorial or supratentorial or basal gangli$ or putaminal or putamen or posterior fossa) adj10 (haemorrhage$ or hemorrhage$ or haematoma$ or hematoma$ or bleed$)).tw.
6. or/1‐5
7. hemodilution/
8. exp plasma substitute/ or plasmapheresis/
9. blood substitute/ or dextran/ or dextran 40/ or dextran 60/ or dextran 70/ or hetastarch/ or polygeline/ or rheodextran/
10. albumin/ or serum albumin/ or sodium chloride/ or exp colloids/
11. phlebotomy/
12. (hemodilut$ or haemodilut$).tw.
13. (plasma adj3 (expand$ or expansion or exchange$ or substitut$ or replace$)).tw.
14. (blood adj3 (expand$ or expansion or exchange$ or substitut$ or replace$ or remov$ or dilut$)).tw.
15. (hetastarch or pentastarch or hydroxyethylstarch or hydroxyethyl‐starch or dextran$ or polygeline or povidone or albumin or saline or colloid$).tw.
16. (phlebotomy or bloodletting or blood‐letting or venesection or venipuncture).tw.
17. or/7‐16
18. 6 and 17
19. Randomized Controlled Trial/
20. Randomization/
21. Controlled Study/
22. control group/
23. clinical trial/ or phase 1 clinical trial/ or phase 2 clinical trial/ or phase 3 clinical trial/ or phase 4 clinical trial/ or controlled clinical trial/
24. Double Blind Procedure/
25. Single Blind Procedure/ or triple blind procedure/
26. latin square design/
27. Parallel Design/
28. placebo/
29. random$.tw.
30. (controlled adj5 (trial$ or stud$)).tw.
31. (clinical$ adj5 trial$).tw.
32. ((control or treatment or experiment$ or intervention) adj5 (group$ or subject$ or patient$)).tw.
33. (quasi‐random$ or quasi random$ or pseudo‐random$ or pseudo random$).tw.
34. ((control or experiment$ or conservative) adj5 (treatment or therapy or procedure or manage$)).tw.
35. ((singl$ or doubl$ or tripl$ or trebl$) adj5 (blind$ or mask$)).tw.
36. (coin adj5 (flip or flipped or toss$)).tw.
37. placebo$.tw.
38. controls.tw.
39. or/19‐38
40. 18 and 39
41. heart stroke volume/ or stroke volume.tw.
42. 40 not 41
43. limit 42 to human
Appendix 4. MEDLINE (Ovid) (1966 to June 2002) search strategy
1. (stroke or cerebrovascular disorders).mp 2. (haemodilution or hemodilution).mp 3. (plasma expanders or dextran or hydroxyethyl starch or albumin).mp 4. (bloodletting or venesection).mp 5. 2 or 3 or 4 6. 1 and 5
Data and analyses
Comparison 1. Haemodilution, all types, versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 16 | 3866 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.90, 1.34] |
| 2 Mortality at late follow‐up (3‐6 months) | 15 | 3957 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.93, 1.20] |
| 3 Dead or dependent/institutionalised (3‐6 months) | 8 | 2491 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.85, 1.07] |
| 4 Venous thromboembolic events at early follow‐up (within 28 days) | 4 | 621 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.20, 3.44] |
| 5 Venous thromboembolic events at late follow‐up (3‐6 months) | 6 | 865 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.37, 1.24] |
| 6 Anaphylactic (or anaphylactic‐like) reactions | 8 | 2253 | Risk Ratio (M‐H, Random, 95% CI) | 3.89 [0.83, 18.30] |
| 7 Serious cardiac events, cumulative at latest follow‐up | 7 | 1358 | Risk Ratio (M‐H, Random, 95% CI) | 1.16 [0.66, 2.05] |
Comparison 2. Hypervolaemic haemodilution (without venesection) versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 12 | 2055 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.68, 1.40] |
| 2 Mortality at late follow‐up (3‐6 months) | 8 | 1746 | Risk Ratio (M‐H, Random, 95% CI) | 1.19 [0.94, 1.51] |
| 3 Dead or dependent/institutionalised (3‐6 months) | 3 | 406 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.74, 1.14] |
Comparison 3. Isovolaemic haemodilution (including venesection) versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 4 | 1811 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.91, 1.46] |
| 2 Mortality at late follow‐up (3‐6 months) | 7 | 2211 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.86, 1.17] |
| 3 Dead or dependent/institutionalised (3‐6 months) | 5 | 2085 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.83, 1.13] |
Comparison 4. Haemodilution using low‐molecular‐weight dextran (dextran 40) versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 10 | 2210 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.76, 1.46] |
| 2 Mortality at late follow‐up (3‐6 months) | 7 | 2037 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.88, 1.20] |
| 3 Dead or dependent/institutionalised (3‐6 months) | 5 | 1888 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.84, 1.20] |
4.1. Analysis.
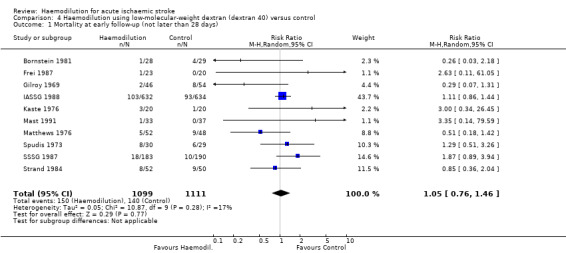
Comparison 4 Haemodilution using low‐molecular‐weight dextran (dextran 40) versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
Comparison 5. Haemodilution using hydroxyethyl starch (HES) versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 4 | 421 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.47, 2.33] |
| 2 Mortality at late follow‐up (3‐6 months) | 4 | 432 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.57, 2.19] |
| 3 Dead or dependent/institutionalised (at 3‐6 months) | 2 | 306 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.71, 1.07] |
Comparison 6. Haemodilution using albumin versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 2 | 1235 | Risk Ratio (M‐H, Random, 95% CI) | 1.21 [0.69, 2.12] |
| 2 Mortality at late follow‐up (3‐6 months) | 3 | 1468 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.78, 1.61] |
Comparison 7. Unconfounded haemodilution (with no other therapeutic modality) versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 14 | 3783 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.89, 1.33] |
| 2 Mortality at late follow‐up (3‐6 months) | 14 | 3914 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.93, 1.19] |
| 3 Dead or dependent/institutionalised (at 3‐6 months) | 8 | 2491 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.85, 1.07] |
7.1. Analysis.
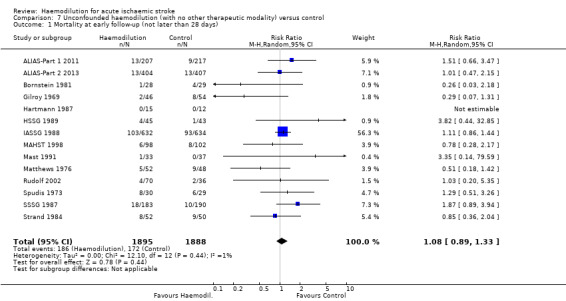
Comparison 7 Unconfounded haemodilution (with no other therapeutic modality) versus control, Outcome 1 Mortality at early follow‐up (not later than 28 days).
7.2. Analysis.
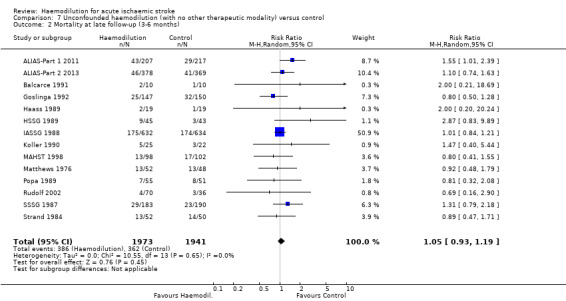
Comparison 7 Unconfounded haemodilution (with no other therapeutic modality) versus control, Outcome 2 Mortality at late follow‐up (3‐6 months).
7.3. Analysis.
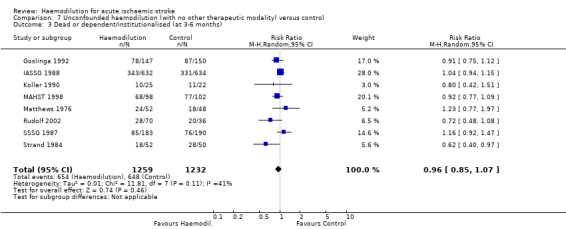
Comparison 7 Unconfounded haemodilution (with no other therapeutic modality) versus control, Outcome 3 Dead or dependent/institutionalised (at 3‐6 months).
Comparison 8. Haemodilution combined with other treatment modalities.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality at early follow‐up (not later than 28 days) | 2 | 83 | Risk Ratio (M‐H, Random, 95% CI) | 2.87 [0.48, 17.21] |
| 2 Mortality at late follow‐up (3‐6 months) | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 2.61 [0.29, 23.13] |
8.1. Analysis.
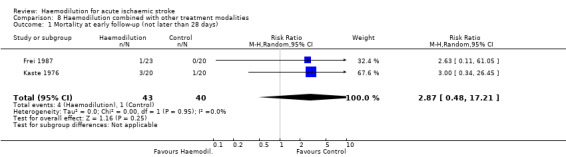
Comparison 8 Haemodilution combined with other treatment modalities, Outcome 1 Mortality at early follow‐up (not later than 28 days).
8.2. Analysis.

Comparison 8 Haemodilution combined with other treatment modalities, Outcome 2 Mortality at late follow‐up (3‐6 months).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
ALIAS‐Part 1 2011.
| Methods | RCT Centralised step‐forward, web‐based 1 : 1 randomisation process All study personnel and participants were blinded |
|
| Participants | People aged ≥ 18 years with acute ischaemic stroke within 5 hours of stroke onset and within 60 minutes of intravenous tPA Diagnosis of ischaemic stroke by CT or MRI scan |
|
| Interventions | 25% albumin therapy (2 g/kg intravenously administered over 120 minutes) versus isovolaemic 0.9% normal saline | |
| Outcomes | Death Neurological score Functional score | |
| Notes | Study suspended in 2007 after interim analysis of differences in overall death between groups Neurological death reported at 7 days Death from any cause reported at 30 and 90 days |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Centralized step‐forward, web‐based 1:1 randomisation process was used" |
| Allocation concealment (selection bias) | Low risk | Quote: "Centralized step‐forward, web‐based" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "All study personnel and patients were blinded" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "All study personnel and patients were blinded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Albumin: 8 participants did not receive allocated intervention, 9 participants lost to follow‐up Control: 2 participants did not receive allocated intervention, 2 participants lost to follow‐up ITT analysis |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
ALIAS‐Part 2 2013.
| Methods | RCT Centralised step‐forward, web‐based 1 : 1 randomisation All study personnel and participants were blinded |
|
| Participants | People aged 18‐83 years with acute ischaemic stroke within 5 hours of stroke onset and within 60 minutes of intravenous tPA Diagnosis of ischaemic stroke by CT or MRI scan |
|
| Interventions | 25% albumin therapy (2 g/kg intravenously administered over 120 minutes) versus isovolaemic 0.9% normal saline | |
| Outcomes | Death Neurological score Functional score | |
| Notes | Neurological death reported at 7 days Death from any cause reported at 30 and 90 days |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Centralized step‐forward, web‐based 1:1 randomisation process with a biased coin minimisation approach that accounted for the status of treatment group balance within and across sites" |
| Allocation concealment (selection bias) | Low risk | Quote: "Centralized step‐forward, web‐based 1:1 randomization process" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "All study personnel and patients were masked to the identity of the study drug. Each sealed kit contained two bottles (initially of 500 mL and 250 mL, then, for manufacturing reasons, both of 500 mL) of the same substance (either albumin or saline) encased in cardboard blinding boxes similar to those used in the Saline versus Albumin Fluid Evaluation (SAFE) Trial, in addition to filters and opaque sheathing to conceal the intravenous tubing. ... A bedside nurse or other personnel not associated with the trial administered the study drug (8 mL/kg estimated bodyweight) by constant intravenous infusion over 2 h (plus or minus 15 min)" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "All study personnel and patients were masked to the identity of the study drug" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Albumin: 3 participants withdrew, 11 participants lost to follow‐up Control: 3 participants withdrew, 13 participants lost to follow‐up, 10 other participants with 90‐day assessment missing ITT analysis |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Balcarce 1991.
| Methods | RCT, single‐blind Randomisation by envelopes |
|
| Participants | People with acute ischaemic stroke within 48 hours and haematocrit 39‐55%, no age limit Diagnosis of ischaemic stroke by CT scan |
|
| Interventions | Venesection with plasma replacement based on the following criteria:
Haemodilution was performed daily during the first 5 days or until haematocrit decreased to 38% |
|
| Outcomes | Death | |
| Notes | Published in Spanish | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Using enveloped containing the group of each patient" |
| Allocation concealment (selection bias) | Low risk | Quote: "Using enveloped containing the group of each patient" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Single‐blinded", "The evaluation was conducted by employees trained by neurologist who were blinded to which group each patient belonged to" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The evaluation was conducted by employees trained by neurologist who were blinded to which group each patient belonged to" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Details not given |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Bornstein 1981.
| Methods | RCT, double‐blind Details of randomisation procedure not given | |
| Participants | People with acute ischaemic stroke within 24 hours of onset | |
| Interventions | Hypervolaemic: dextran 40 versus placebo (not specified) | |
| Outcomes | Death Neurological score | |
| Notes | Published in Hebrew | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Details not given |
| Allocation concealment (selection bias) | Unclear risk | Details not given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Details not given |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Frei 1987.
| Methods | RCT Randomisation by using closed envelopes Evaluators and participants blinded | |
| Participants | People with acute ischaemic stroke within 30 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Hypervolaemic: dextran 40 plus glycerol versus placebo infusion | |
| Outcomes | Death Neurological score Venous thromboembolic events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by using closed envelopes |
| Allocation concealment (selection bias) | Low risk | Adequate |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 61 participants entered. 10 deaths, 2 participants discontinued in intervention |
| Selective reporting (reporting bias) | Low risk | All outcome reported |
Gilroy 1969.
| Methods | RCT Randomisation by using closed envelopes Information on blinding of evaluators or participants, or both, not given | |
| Participants | People with acute presumed ischaemic stroke within 72 hours of onset, haemorrhage excluded by CSF analysis | |
| Interventions | Hypervolaemic: dextran 40 for 72 hours versus a dextrose‐saline infusion | |
| Outcomes | Death Clinical improvement/deterioration (global assessment) Change in neurological score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "An envelope was taken in numerical series from 100 envelopes assorted in a random manner" |
| Allocation concealment (selection bias) | Low risk | Quote: "An envelope was taken in numerical series from 100 envelopes assorted in a random manner" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "The instruction 'treat' or 'control' which was contained in the envelope dictated the method of treatment" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Goslinga 1992.
| Methods | RCT Stratified randomisation, other details about the randomisation procedure not known Evaluators or participants, or both, not blinded | |
| Participants | People with acute ischaemic stroke within 48 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Isovolaemic: 20% albumin plus crystalloids plus venesection for 5 days versus crystalloids alone | |
| Outcomes | Death Functional outcome | |
| Notes | 300 participants randomised, data at follow‐up not reported in 1 participant receiving haemodilution and 2 participants receiving control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "One of the problems with the methodology of haemodilution trials is that a blind control group is not possible, either for the patient or for the medical staff" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "One of the problem with the methodology of haemodilution trials is that a blind control group is not possible, either for the patient or for the medical staff" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Exclusion information was provided. Post‐randomisation withdrawal was not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Haass 1989.
| Methods | RCT Details of randomisation procedure not known Possible blinding of evaluators or participants, or both, not known | |
| Participants | People with acute ischaemic stroke within 24 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Hypervolaemic: HES for 10 days versus crystalloid infusions | |
| Outcomes | Death Neurological score Functional score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Information not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Hartmann 1987.
| Methods | RCT Randomisation procedure not known Blinding of evaluators or participants, or both, not known | |
| Participants | People with acute ischaemic stroke in the carotid artery territory within 24 hours of onset Diagnosis of ischaemic stroke by CT scan in all participants | |
| Interventions | Hypervolaemic: HES 200 for 7 days versus no specific treatment | |
| Outcomes | Cerebral blood flow Death Complications | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Information not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
HSSG 1989.
| Methods | RCT Randomisation procedure not known Multicentre (13 centres) Evaluators blinded but not participants or managing physicians | |
| Participants | People with acute ischaemic stroke within 24 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Individualised hypervolaemic or isovolaemic: HES for 72‐96 hours plus venesection in selected participants during the first 24 hours versus no specific treatment | |
| Outcomes | Death Neurological score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Information not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Hypervolaemic: 15 participants did not complete the study: 9 died and 6 due to allergy, low haematocrit, lost to follow‐up, confined to distant nursing home, study terminated early Control: 6 participants did not complete the study: 3 died, other 3 due to malingering, lost to follow‐up, study terminated early |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
IASSG 1988.
| Methods | RCT Multicentre (31 centres) Telephone randomisation by lists kept at the co‐ordinating centre Evaluation of functional outcome by blinded telephone interview | |
| Participants | People with acute ischaemic and haemorrhagic stroke within 12 hours of onset Diagnosis of stroke subtype by CT scan in 97% of cases | |
| Interventions | Isovolaemic: dextran 40 plus venesection during the first 24 hours versus no specific therapy | |
| Outcomes | Death Functional independency/dependency at discharge and at 6‐month follow‐up | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by lists |
| Allocation concealment (selection bias) | Low risk | Telephone randomisation by lists kept at the co‐ordinating centre |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Since it was not possible to use a sham procedure the patient in the control group received only the most appropriate general treatment, the same as that provided for the patients in the haemodilution group" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Evaluation of functional outcome by blinded telephone interview |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Kaste 1976.
| Methods | RCT Randomisation by choosing from identical‐looking vials Evaluators and participants blinded | |
| Participants | People with acute presumed ischaemic stroke within 24 hours of onset Diagnosis of ischaemic stroke by CSF analysis and brain isotope scanning in all participants | |
| Interventions | Hypervolaemic: dextran 40 for 72 hours plus dexamethasone for 14 days versus placebo | |
| Outcomes | Death Neurological score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "We were unaware of the identity of the phials [sic] being used" |
| Allocation concealment (selection bias) | Low risk | Quote: "We were unaware of the identity of the phials [sic] being used" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The code being broken only after final evaluation of the patients' conditions" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The code being broken only after final evaluation of the patients' conditions" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Koller 1990.
| Methods | RCT Randomisation by using closed envelopes Evaluators but not participants blinded | |
| Participants | People with acute ischaemic stroke in the middle cerebral artery territory within 24 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Isovolaemic: dextran 40 plus venesection for 72 hours versus saline infusion | |
| Outcomes | Death Neurological score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by using closed envelopes |
| Allocation concealment (selection bias) | Low risk | Randomisation by using closed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Evaluators blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Haemodilution: 1 participant refused last follow‐up examination Control: 3 participants withdrawn due to misdiagnosis and doctor in charge changed treatment |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
MAHST 1998.
| Methods | RCT Randomisation by selecting from identical‐looking bottles Evaluators, participants and attending physicians blinded | |
| Participants | People with acute ischaemic stroke within 6 hours of onset Diagnosis of ischaemic stroke by CT | |
| Interventions | Hypervolaemic: HES plus crystalloid solution for 5 days versus crystalloids alone | |
| Outcomes | Death Neurological scores Functional score | |
| Notes | The trial was intended to include 400 participants. It was interrupted after an interim analysis performed when 200 participants had been included. There were 3 reasons: the originally planned sample size would have been too small to demonstrate any effects of haemodilution, recruitment to the study was slow and there were financial constraints | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization scheme was generated by permutation of random numbers (Sofware Randomsys, University of Linz) in 150 blocks with length of four patients each by an external biometrics consultant" |
| Allocation concealment (selection bias) | Low risk | Quote: "By an external biometrics consultant" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ITT and per‐protocol analysis performed. 42 participants were not considered for the per‐protocol analysis due to cerebral haematoma, brain stem and cerebellar infarcts, protocol violation, low haematocrit, elevated creatine and cardiac complication. Which group had these characteristics was not reported |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Mast 1991.
| Methods | RCT Randomisation by using closed envelopes Evaluators but not participants blinded | |
| Participants | People with acute ischaemic stroke within 24 hours of onset Diagnosis of ischaemic stroke by CT scan | |
| Interventions | Isovolaemic: dextran 40 plus venesection versus no specific treatment | |
| Outcomes | Death Neurological score at 2 weeks | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by using closed envelopes |
| Allocation concealment (selection bias) | Low risk | Randomisation by using closed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Evaluators blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Matthews 1976.
| Methods | RCT Randomisation by using closed envelopes Evaluators not blinded | |
| Participants | People with presumed ischaemic stroke within 48 hours of onset Haemorrhage excluded by CSF analysis | |
| Interventions | Hypervolaemic: dextran 40 for 72 hours versus dextrose infusion | |
| Outcomes | Death Neurological score Functional score Need for institutional care | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomly allocated to either dextran group or the control group by opening the next one of a series of envelopes" |
| Allocation concealment (selection bias) | Low risk | Quote: "Patients were randomly allocated to either dextran group or the control group by opening the next one of a series of envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Information on patient blinding not provided Quote: "After entry to the trial they remained under the care of the firm that had admitted them who did of course know whether dextran or 5 per cent dextrose solution was administered" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "After entry to the trial they remained under the care of the firm that had admitted them who did of course know whether dextran or 5 per cent dextrose solution was administered" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Popa 1989.
| Methods | RCT Randomisation procedure unknown No information on blinding of evaluators, participants, or both | |
| Participants | People with presumed ischaemic stroke, haemorrhage excluded by CSF analysis | |
| Interventions | Isovolaemic: dextran 40 for 5 days plus venesection for 2 days versus no specific treatment | |
| Outcomes | Death Neurological score Functional score | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Information not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Information not provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Rudolf 2002.
| Methods | Randomised placebo‐controlled trial Multicentre (16 centres) Randomisation procedure not described | |
| Participants | People with ischaemic stroke (CT scan) within 6 hours of onset | |
| Interventions | Hypervolaemic: HES 10% for 7 days versus saline infusions | |
| Outcomes | Death Neurological scores Functional scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Of the 107 patients randomised, 106 patients received at least one dose of study drug" No additional information provided on number of participants that completed the study |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Spudis 1973.
| Methods | RCT Randomisation procedure not known Evaluators but not participants blinded | |
| Participants | People with presumed ischaemic stroke within 24 hours of onset Haemorrhage excluded by CSF analysis in all participants | |
| Interventions | Hypervolaemic: dextran 40 for 72 hours versus no specific treatment | |
| Outcomes | Death Change in neurological signs | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Information not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "After one week the patient was independently graded by a second author, and after three weeks, by the author.... The second and third examiners never had an opportunity to see the patients while dextran was running and had little reason to try to guess which patients were controls" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dextran: 1 participant eliminated due to flushing and apnoea Controls: no participants withdrawn |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
SSSG 1987.
| Methods | RCT Multicentre (15 centres) Stratified randomisation by using closed envelopes Evaluators blinded, participants and attending physicians not blinded | |
| Participants | People with acute ischaemic stroke within 48 hours of onset Diagnosis of ischaemic stroke by CT scan in 63% and by CSF analysis in the remaining participants | |
| Interventions | Isovolaemic: dextran 40 for 48 hours plus venesection for the first 24‐48 hours versus no specific treatment | |
| Outcomes | Death
Neurological score
Functional score Need for institutional care Other clinical events |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratification by centre, age, prognostic neurological score by "preset multiple of 4 by drawing envelopes containing a slip assigning a particular patient to one of the two groups" |
| Allocation concealment (selection bias) | Low risk | Quote: "Drawing envelopes containing a slip assigning a particular patient to one of the two groups" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and attending physicians not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Evaluators blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information provided |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
Strand 1984.
| Methods | RCT Randomisation by using closed envelopes Evaluators blinded, participants and attending physicians not blinded | |
| Participants | People with acute ischaemic stroke within 48 hours of onset Diagnosis of ischaemic stroke by CT scan and CSF analysis in all participants | |
| Interventions | Isovolaemic: dextran 40 for 7 days plus venesection during the first 24‐48 hours versus no specific treatment | |
| Outcomes | Death Neurological score Functional score Need for institutional care Other circulatory events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by using closed envelopes |
| Allocation concealment (selection bias) | Low risk | Closed envelope |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | People and attending physicians not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Evaluators blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4 participants with small intracerebral haemorrhage (2 in intervention and control), 4 participants not fulfilling inclusion criteria, and 1 deaf and blind participant were inadvertently randomised. ITT analysis on the remaining participants Haemodilution was interrupted in 2 participants with anaphylactoid reaction |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
CSF: cerebrospinal fluid; CT: computed tomography; HES: hydroxyethyl starch; ITT: intention‐to‐treat; MRI: magnetic resonance imaging; RCT: randomised controlled trial; tPA: tissue plasminogen activator.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Chen 2006 | Randomised trial comparing venesection and haemodilution plus herbal medicine of 1 form versus herbal medicine of another form. Death was reported |
| Ding 1992 | Quasi‐randomised trial of 2 different haemodilution regimens: normovolaemic (venesection plus dextran) versus hypervolaemic (dextran only) |
| Grauer 1999 | Randomised double‐blind study comparing low‐ and medium‐dose HES with haematological and neurological score outcome |
| Hamamoto 1992 | Randomised trial of unspecified 'hypervolaemic haemodilution', no information or detail of therapy. Cerebral blood flow and neurological score reported but not mortality, dependency or institutional care. Abstract only |
| Hartmann unpubl. | The trial was terminated early for logistical reasons. No data have been available to the review authors (despite personal contacts and reminders to the principal investigator and the manufacturer during the years 1993‐1995) |
| Hayes 2000 | Study on the effects of transcranial Doppler directed dextran 40 therapy to prevent postoperative stroke in people undergoing carotid endarterectomy. Historical controls |
| Koppi 1996 | Cerebrolysin (so‐called "neuron metabolism specific treatment") compared with haemodilution in a non‐randomised trial |
| Krack 1989 | Study on the haemodynamic effects of HES in people with stroke. Participants were their own controls (before versus after haemodilution) and no clinical outcome data were given (except the haemodynamic variables) |
| Luo 1991 | Non‐randomised trial (controls were matched with treated participants) with initial venesection plus low‐molecular‐weight dextran, then dextran daily for 15 days. Neurological score and laboratory variables were reported but not mortality or dependency or institutional care |
| Morgenthaler 2010 | RCT comparing 2 doses of HES with haemodynamics and rheology as outcomes. Adverse event questionnaire included pruritus |
| Porro 1985 | Randomised trial of isovolaemic haemodilution (7 participants; procedure not described) versus conventional treatment (8 participants) Emphasis on haemorheological outcome variables. Clinical effects described as "the neurological symptoms were not apparently influenced" without more detailed specifications |
| Schwarz 1998 | Study of the effects of HES and mannitol on intracranial pressure and cerebral perfusion pressure, not possible to abstract clinical endpoints |
| Shin 2007 | Randomised trial comparing albumin versus saline. Outcomes included neurological score and imaging |
| Staedt 1987 | Clinical trial comparing HES versus dextran with neurological outcome |
| Staedt 1989 | Prospective cross‐over study comparing HES, dextran and isotonic solution with haematological and eye oxygenation outcome |
| Staedt 1991 | Randomised trial comparing hypervolaemic haemodilution with haematocrit goal of 41‐43% versus 37‐39%. 1 death was reported but it is unknown in which group the death occurred. In addition, it does not report the number of people in each group. Abstract only |
| Stoll 1998 | Study of the acute effects of HES on haemodynamic variables and neurological score. No randomised control group |
| Strand 2002 | RCT comparing venesection plus dextran versus control with neurological score as outcome |
| Tessitore 1990 | Randomised trial comparing haemodilution and placebo with haematocrit and gross motor function outcomes |
| Torun 1995 | RCT of isovolaemic haemodilution (venesection plus HES; 95 participants) versus control (84 participants). No numbers given on survival or functional outcome |
| Walzl 1994 | Randomised trial of extracorporal fibrinogen and platelet precipitation, reporting only on intermediary (laboratory) outcome variables; no clinical information |
| Wang 1988 | Non‐randomised study of the combination of blood‐letting and either dextran 40 or hydroxyethyl amylum. Control group matched by age, sex and severity of stroke |
| Wang 1990 | Randomised trial of 2 different haemodilution regimens: plasma expander 706 (unknown content) plus crystalloid solution plus venesection versus low‐molecular‐weight dextran plus Chuan Xiong Qing (Chinese herb) |
| Wise 1976 | Randomised trial of 3 different interventions, of which 1 included a combination of a steroid (dexamethasone) and dextran. No figures on outcome given. Abstract only |
| Woessner 2003 | Randomised double‐blind trial comparing HES versus crystalloid solution. Outcomes only included haemodynamic parameters |
| Zhang 1990 | Randomised trial of intervention isovolaemic blood dilution with plasma substitute plus vitamin B and C versus control low‐molecular‐weight dextran and ligustrazine, a Chinese herbal medicine, plus vitamin B and C |
| Zhang 1996 | Controlled trial, but not clear if it was a randomised study. Mixture of people with acute stroke and in late phase after stroke (> 30 days). Wide variations between participants in the duration of follow‐up |
HES: hydroxyethyl starch; RCT: randomised controlled trial.
Differences between protocol and review
The 2002 version stated in the methods that "Only studies which reported clinical end‐points of direct relevance for the patients (death, neurological outcome, functional outcome, need for institutional care, vascular or other events, adverse reactions) have been included." and "Many studies reported on changes in neurological and functional scores. A plethora of scores and measures of distribution have been used. Therefore, it has not been possible to report on changes of score sums in a uniform manner." All studies containing neurological outcome also had other outcomes including mortality, need for institutional care, etc. Therefore, these studies could be included in the data and analyses.
We decided not to include studies that only had neurological score outcomes, which may have been implicit in the 2002 methods. These studies could not be added to the data and analyses given the varying scores. Therefore, we added the following in the current version's methods "...studies that only included neurological examination scale outcomes because these outcomes could not be combined given the variety of neurological scores (see Types of outcome measures)."
Contributions of authors
Kjell Asplund published the first review in 1995 with the aid of Karin Israelsson and Ingrid Schampi, who were both medical students. They contributed to the literature search and with independent abstracting of data from the articles. Kjell Asplund updated this review in 2002.
Matthew Jensen took charge of this review in 2011. He was involved in co‐ordinating the review, data collection, analysis of data, interpretation of data, writing the review and general advice on the review. Timothy Chang was involved in data collection, data management, analysis of data, interpretation of data and writing the review.
Sources of support
Internal sources
No sources of support supplied
External sources
Swedish Medical Research Council, Swedish Social Research Council, Chest and Heart Fund, Vardalstiftelsen, Sweden.
Clinical and Translational Science Award program, previously through the National Center for Research Resources grant 1UL1RR025011, and now by the National Center for Advancing Translational Sciences grant 9U54TR000021, USA.
National Heart Lung and Blood Institute Fellowship F30HL112491, USA.
National Institute of Health T32 GM008692, USA.
-
National Institute of Health, USA.
1K08NS079622‐01A1
Declarations of interest
None known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
ALIAS‐Part 1 2011 {published data only}
- Ginsberg MD, Martin RH, Hill MD, Palesch YY, Yeatts S, Moy CS, for the ALIAS Investigators. The Albumin in Acute Stroke (ALIAS) Trial: part 1 safety analysis. Stroke 2010;41(4):e228. [Google Scholar]
- Ginsberg MD, Palesch YY, Martin RH, Hill MD, Moy CS, Waldman BD, for the ALIAS Investigators. The Albumin in Acute Stroke (ALIAS) multicenter clinical trial: safety analysis of part 1 and rationale and design of part 2. Stroke 2011;42(1):119‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill MD, Martin RH, Palesch YY, Tamariz D, Waldman BD, Ryckborst KJ, for the ALIAS Investigators, Neurological Emergencies Treatment Trials Network. The Albumin in Acute Stroke Part 1 Trial: an exploratory efficacy analysis. Stroke 2011;42(6):1621‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill MD, Moy CS, Palesch YY, Martin R, Dillon CR, Waldman BD, for the ALIAS Investigators. The ALbumin In Acute Stroke trial (ALIAS); design and methodology. International Journal of Stroke 2007;2(3):214‐9. [DOI] [PubMed] [Google Scholar]
ALIAS‐Part 2 2013 {published data only}
- Ginsberg MD, Palesch YY, Hill MD, Martin RH, Moy CS, Barsan WG, ALIAS and Neurological Emergencies Treatment Trials (NETT) Investigators. High‐dose albumin treatment for acute ischaemic stroke (ALIAS) Part 2: a randomised, double‐blind, phase 3, placebo‐controlled trial. Lancet Neurology 2013;12(11):1049‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
Balcarce 1991 {published data only}
- Balcarce PE, Vila JF, Fustinoni O. Isovolaemic haemodilution with plasma in acute ischaemic stroke [Hemodilución isovolémica con plasma en el accidente cerebrovascular isquémico agudo]. Revista Neurologica Argentina 1991;16:154‐60. [Google Scholar]
Bornstein 1981 {published data only}
- Bornstein N, Regev I, Flechater S, Streifler M, Vardi J. Dextran‐40 in nonhemorrhagic cerebrovascular accidents. Harefuah 1981;100:455‐6. [PubMed] [Google Scholar]
Frei 1987 {published data only}
- Frei A, Cottier C, Wunderlich P, Ladin E. Glycerol and dextran combined in the therapy of acute stroke. A placebo‐controlled, double‐blind trial with a planned interim analysis. Stroke 1987;18:373‐9. [DOI] [PubMed] [Google Scholar]
Gilroy 1969 {published data only}
- Gilroy J, Barnhardt MI, Meyer JS. Treatment of acute stroke with Dextran 40. JAMA 1969;210:293‐8. [PubMed] [Google Scholar]
Goslinga 1992 {published data only}
- Goslinga H, Eijzenbach V, Heuvelmans JHA, Nes JCM, Kurk RM, Bezemer PD. Haemodilution in acute cerebral infarction; administration of albumin solution and crystalline infusion fluid guided by the haematocrit [Hemodilutie op maat bij het acute herseninfarct met behulp van een 20%‐albumine‐oplossing en fysiologische zoutoplossing]. Nederlands Tijdschrift voor Geneeskunde 1992;136:2422‐8. [PubMed] [Google Scholar]
- Goslinga H, Eijzenbach V, Heuvelmans JHA, Laan de Vries E, Melis VMJ, Schmid‐Schonbein H, et al. Custom‐tailored hemodilution with albumin and crystalloids in acute ischemic stroke. Stroke 1992;23:181‐8. [DOI] [PubMed] [Google Scholar]
- Goslinga H, Heuvelmans JH, Schmid‐Schönbein H. Hemodilution and rehydration in acute ischemic stroke. A preliminary report on the Amsterdam Stroke Study. Acta Medica Austriaca 1991;18 Suppl 1:41‐4. [PubMed] [Google Scholar]
Haass 1989 {published and unpublished data}
- Haass A, Decker I, Hamann G, Stoll M, Schimrigk K, Kasser U. Hemodilution therapy of acute stroke. Proceedings of the Satellite Symposium on Haemodilution at the First European Stroke Conference; 1990 10‐12 May; Dusseldorf, Germany.
- Krack P, Haass A. Hemodynamic effect of hemodilution with hydroxyethyl starch. Stroke 1989;20:137. [Google Scholar]
Hartmann 1987 {published data only}
- Hartmann A. Regional cerebral blood flow in acute cerebral infarction during hypervolemic hemodilution. In: Meyer JS, Lechner H, Reivich M, Ott EO editor(s). Cerebral Vascular Disease 5. Amsterdam: Excerpta Medica, 1985:206‐14. [Google Scholar]
- Hartmann A, Tsuda Y, Lagreze H, Dettmers C. Effect of hemodilution on regional cerebral blood flow in patients with acute cerebral infarction. In: Hartmann A, Kuschinsky W editor(s). Cerebral Ischemia and Hemorheology. Berlin: Springer‐Verlag, 1987:423‐8. [Google Scholar]
HSSG 1989 {published data only}
- The Hemodilution in Stroke Study Group. Hypervolemic hemodilution treatment of acute stroke. Results of a randomized multicenter trial using pentastarch. Stroke 1989;20:317‐23. [DOI] [PubMed] [Google Scholar]
IASSG 1988 {published data only}
- Italian Acute Stroke Study Group. Haemodilution in acute stroke: results from the Italian Haemodilution Trial. Lancet 1988;i:318‐20. [PubMed] [Google Scholar]
- Italian Acute Stroke Study Group. The Italian hemodilution trial in acute stroke. Italian Acute Stroke Study Group. Stroke 1987;18(3):670‐6. [DOI] [PubMed] [Google Scholar]
Kaste 1976 {published data only}
- Kaste M, Fogelholm R, Waltimo O. Combined dexamethasone and low‐molecular‐weight dextran in acute brain infarction: double‐blind study. British Medical Journal 1976;2:1409‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Koller 1990 {published data only}
- Koller M, Haenny P, Hess K, Weniger D, Zangger P. Adjusted hypervolemic hemodilution in acute ischemic stroke. Stroke 1990;21:1429‐34. [DOI] [PubMed] [Google Scholar]
MAHST 1998 {published data only}
- Aichner F, Brainin M, Fazekas F, Mamoli B, Polz W, Zeiler K. Hypervolemic hemodilution and rehydration in the early phase of ischemic stroke: results of the Multicenter Austrian Hemodilution Stroke Trial (MAHST). Journal of the Neurological Sciences 1997;150 Suppl:S76. [Google Scholar]
- Aichner FT, Fazekas F, Brainin M, Polz W, Mamoli B, Zeiler K. Hypervolemic hemodilution in acute ischemic stroke: the Multicenter Austrian Hemodilution Stroke Trial (MAHST). Stroke 1998;29:743‐9. [DOI] [PubMed] [Google Scholar]
Mast 1991 {published data only}
- Mast H, Marx P. Neurological deterioration under isovolemic hemodilution with hydroxyethyl starch in acute cerebral ischemia. Stroke 1991;22:680‐3. [DOI] [PubMed] [Google Scholar]
- Mast H, Vogel H‐P, Marx P. Hemodilution in ischemic stroke. Stroke 1991;22:955. [PubMed] [Google Scholar]
Matthews 1976 {published data only}
- Matthews WB, Oxbury JM, Grainger KMR, Greenhall RCD. A blind controlled trial of dextran 40 in the treatment of ischemic stroke. Brain 1976;99:193‐206. [DOI] [PubMed] [Google Scholar]
Popa 1989 {published data only}
- Popa G, Popa C, Stanescu A, Ionescu G, Lugoji G, Radula D, et al. Haemodilution therapy in acute ischaemic stroke. Revue Roumaine de Neurologie et de Psychiatrie 1989;27:79‐90. [PubMed] [Google Scholar]
Rudolf 2002 {published and unpublished data}
- Heiss W‐D for the HES Study Group. Hypervolemic hemodilution by hydroxyethyl starch in acute ischemic stroke. Stroke 1999;30:270. [Google Scholar]
- Rudolf J. Evaluation of safety of hydroxyethyl starch (HES) in hypervolemic hemodilution in patients with acute ischemic stroke ‐ an explanatory pilot study. Cerebrovascular Diseases 2001;11 Suppl 4:121. [DOI] [PubMed] [Google Scholar]
- Rudolf J, HES in Acute Stroke Study Group. Hydroxyethyl starch for hypervolemic hemodilution in patients with acute ischemic stroke: a randomized, placebo‐controlled phase II safety study. Cerebrovascular Diseases 2002;14:33‐41. [DOI] [PubMed] [Google Scholar]
Spudis 1973 {published data only}
- Spudis EV, Torre E, Pikula L. Management of completed stroke with dextran 40. A community hospital failure. Stroke 1973;4:895‐7. [DOI] [PubMed] [Google Scholar]
SSSG 1987 {published data only}
- Scandinavian Stroke Study Group. Hemodilution in acute ischemic stroke ‐ a randomized multicenter trial. Stroke 1986;17:143. [Google Scholar]
- Scandinavian Stroke Study Group. Multicenter trial of hemodilution in acute ischemic stroke: I. Results in the total patient population. Stroke 1987;18:691‐9. [DOI] [PubMed] [Google Scholar]
- Scandinavian Stroke Study Group. Multicenter trial of hemodilution in acute ischemic stroke: background and study protocol. Stroke 1985;16:885‐90. [DOI] [PubMed] [Google Scholar]
- Scandinavian Stroke Study Group. Multicenter trial of hemodilution in acute ischemic stroke: results of subgroup analyses. Stroke 1988;19:464‐71. [DOI] [PubMed] [Google Scholar]
Strand 1984 {published data only}
- Asplund K, Eriksson S, Hagg E, Lithner F, Strand T, Wester PO. Ischemic stroke treated by haemodilution: an interim report of a randomized trial. In: Meyer JS, Lechner H, Reivich M, Ott EO editor(s). Cerebral Vascular Disease 4. I.C.S. No. 616. Elsevier Science Publishing Co, 1982:148‐50. [Google Scholar]
- Strand T. Evaluation of long‐term outcome and safety after hemodilution therapy in acute ischemic stroke. Stroke 1992;23(5):657‐62. [DOI] [PubMed] [Google Scholar]
- Strand T, Asplund K, Eriksson S, Hagg E, Lithner F, Wester PO. A randomized controlled trial of hemodilution therapy in acute ischemic stroke. Stroke 1984;15:980‐9. [DOI] [PubMed] [Google Scholar]
- Strand T, Asplund K, Eriksson S, Hagg E, Lithner F, Wester PO. Hemodilution treatment of ischemic stroke. Stroke 1983;14:122. [Google Scholar]
References to studies excluded from this review
Chen 2006 {published data only}
- Chen Y, Xie GB. Evaluation of modified hemodilution combined therapy in the treatment of acute ischemic stroke in the elderly. Neural Regeneration Research 2006;1(2):184‐7. [Google Scholar]
Ding 1992 {published data only}
- Ding M, Wang NG, Pang SQ, Liu JX. A prospective trial of hemodilution therapy in acute cerebral infarction. Chung Hua Shen Ching Ching Shen Ko Tsa Chih 1992;25:146‐9. [PubMed] [Google Scholar]
Grauer 1999 {published data only}
- Grauer MT, Woessner R, Seltmann A, Windisch F, Schenk JF, Wenzel E, et al. Therapeutic safety of a high‐dose volume therapy with hydroxyethyl starch in patients with acute stroke under intensive care monitoring. Anasthesiologie Intensivmedizin Notfallmedizin Schmerztherapie 1999;34:S87‐8. [Google Scholar]
Hamamoto 1992 {published data only}
- Hamamoto M, Nagao T, Kanda A, Ichiseki H, Miyazaki T, Terashi A. Hypervolemic hemodilution for the elderly patients with atherothrombotic and hemodynamic ischemic stroke. Journal of Stroke and Cerebrovascular Diseases 1992;2 Suppl 1:S136. [Google Scholar]
Hartmann unpubl. {unpublished data only}
- Hartmann A. Unpublished data.
Hayes 2000 {published data only}
- Hayes PD, Lloyd AJ, Lennard N, Wolstenholme JL, London NJ, Bell PR, et al. Transcranial Doppler‐directed dextran‐40 therapy is a cost‐effective method of preventing carotid thrombosis after carotid endarterectomy. European Journal of Vascular and Endovascular Surgery 2000;19:56‐61. [DOI] [PubMed] [Google Scholar]
Koppi 1996 {published data only}
- Koppi S, Barolin GS. Hemodilution therapy with neuron metabolism specific therapy in ischemic stroke ‐ encouraging results of a comparative study. Wiener Medizinische Wochenschrift 1996;146:41‐8. [PubMed] [Google Scholar]
- Koppi S, Barolin GS. Use of cerebrolysin in the treatment of ischemic stroke. Zhurnal Nevrologii i Psikhiatrii Imeni S.S. Korsakova 1998;98:30‐3. [PubMed] [Google Scholar]
Krack 1989 {published data only}
- Krack P, Haass A. Hemodynamic effect of hemodilution with hydroxyethyl starch. Stroke 1989;20:137. [Google Scholar]
Luo 1991 {published data only}
- Luo Y, Du Q. Hemodilution in the treatment of acute cerebral ischemia. Chung Hua Shen Ching Ching Shen Ko Tsa Chih 1991;24:244‐6. [PubMed] [Google Scholar]
Morgenthaler 2010 {published data only}
- Morgenthaler M, Woessner R, Treib J. Is there new safety information to be gained out of the use of thrombelastography in stroke patients receiving hydroxyethyl starches for treatment?. Cerebrovascular Diseases 2010;29 Suppl 2:235. [Google Scholar]
Porro 1985 {published data only}
- Porro F, Pastori P, Lanzoni M, Curti L, Fanelli M. Hemorheology in acute ischemic stroke: influence of isovolemic hemodilution. Clinical Hemorheology 1985;5:669. [Google Scholar]
Schwarz 1998 {published data only}
- Schwarz S, Schwab S, Bertram M, Aschoff A, Hacke W. Effects of hypertonic saline hydroxyethyl starch solution and mannitol in patients with increased intracranial pressure after stroke. Stroke 1998;29:1550‐5. [DOI] [PubMed] [Google Scholar]
Shin 2007 {published data only}
- Shin DH, Moon GJ, Bang OY. Albumin therapy in acute stroke patients. Journal of Neurology 2007;254:870‐8. [DOI] [PubMed] [Google Scholar]
Staedt 1987 {published data only}
- Staedt V, Huett M, Seufzer U, Oster P, Schlierf G, Morl H. The treatment of acute cerebral infarcts. Comparative study of hemodilution therapy with 10% HES 200/0.5 and 10% dex 40. Therapiewoche 1987;37:2944‐9. [Google Scholar]
Staedt 1989 {published data only}
- Staedt U, Stein T, Herrmann T. Effect of HAES 200/0,5‐, dextran 40 and isotonic solution on haemorheology and microcirculation in patients with brain infarction. Zeitschrift fur Kardiologie 1989;78 Suppl 1:113. [Google Scholar]
Staedt 1991 {published data only}
- Staedt U, Stein T, Arling G, Herrmann M, Keller H. Is there a relation between the improvement of blood fluidity and neurological symptoms in brain infarction? [Besteht ein Zusammenhang zwitschen der verbesserung von blutfluiditat und neurologischen symptomatik bei hirninfarkt?]. VASA. Supplementum 1991;20 Suppl 33:163‐4. [PubMed] [Google Scholar]
Stoll 1998 {published data only}
- Stoll M, Treib J, Seltmann A, Anton H, Klaus S. Hemodynamics of stroke patients under therapy with low molecular weight hydroxyethyl starch. Neurological Research 1998;20:231‐4. [DOI] [PubMed] [Google Scholar]
Strand 2002 {published data only}
- Strand T, Hjerppe C. Update hemodilution therapy: dextran improves the clinical course in patients with cerebral infarction and leukocytosis. Cerebrovascular Diseases 2002;13 Suppl 3:8. [Google Scholar]
Tessitore 1990 {published data only}
- Tessitore A, Diaco S, Battaglia A. Hydroxyethyl starch in the treatment of ischemic stroke. Quaderni di Medicina e Chirurgia 1990;6(3):350‐2. [Google Scholar]
Torun 1995 {published data only}
- Torun S, Özöner Z, Gucuyner D, Uzuner N, Özdemir G. The effects of isovolemic hemodilution in acute ischemic stroke: a randomized controlled clinical trial. European Journal of Neurology 1995;2:78. [Google Scholar]
Walzl 1994 {published data only}
- Walzl B, Walzl M, Lechner H. Extracorporeal fibrinogen and platelet precipitation as a new haemorheological treatment for acute stroke. Journal of the Neurological Sciences 1994;126:25‐9. [DOI] [PubMed] [Google Scholar]
Wang 1988 {published data only}
- Wang B‐P, Sun F‐C. Treatment of ischemic cerebral stroke by isovolemic hemodilution. Clinical Hemorheology 1988;8:269‐72. [Google Scholar]
Wang 1990 {published data only}
- Wang B‐P, Cao J, Liu Y‐C, Xin H‐H, Sun F‐C, Zhao J‐Q, et al. Treatment of ischemic cerebral apoplexy by equivalent volume hemodilution. Chung Hua Shen Ching Ching Shen Ko Tsa Chih 1990;23:81‐3. [Google Scholar]
Wise 1976 {published data only}
- Wise G. Comparison of papaverine and decadron to decadron and dextran to decadrone therapy alone in acute ischemic infarction. Stroke 1976;7:6. [Google Scholar]
Woessner 2003 {published data only}
- Woessner R, Grauer MT, Dieterich HJ, Bepperling F, Baus D, Kahles T, et al. Influence of a long‐term, high‐dose volume therapy with 6% hydroxyethyl starch 130/0.4 or crystalloid solution on hemodynamics, rheology and hemostasis in patients with acute ischemic stroke. Results of a randomized, placebo‐controlled, double‐blind study. Pathophysiology of Haemostasis and Thrombosis 2003;33(3):121‐6. [DOI] [PubMed] [Google Scholar]
Zhang 1990 {published data only}
- Zhang C, Han Z. Dynamic state of haematocrit and blood dilution treatment of ischemic cerebrovascular diseases. Journal of Apoplexy and Nervous Diseases 1990;7:49‐50. [Google Scholar]
Zhang 1996 {published data only}
- Zhang Y, Wang C, Li K. A comparative study of the efficacy of normovolemic hemodilution and traditional therapy in treating ischemic stroke. Zhurnal Nevropatologii i Psikhiatrii Imeni S.S. Korsakova 1996;96:98. [PubMed] [Google Scholar]
Additional references
Aronowski 1996
- Aronowski J, Strong R, Grotta JC. Combined neuroprotection and reperfusion therapy for stroke. Effect of lubeluzole and diaspirin cross‐linked hemoglobin in experimental focal ischemia. Stroke 1996;27:1571‐6. [DOI] [PubMed] [Google Scholar]
Asplund 1991
- Asplund K. Hemodilution in acute stroke. Cerebrovascular Diseases 1991;1 Suppl 1:129‐38. [Google Scholar]
Belayev 2001
- Belayev L, Liu Y, Zhao W, Busto R, Ginsberg MD. Human albumin therapy of acute ischemic stroke: marked neuroprotective efficacy at moderate doses and with a broad therapeutic window. Stroke 2001;32:553‐60. [DOI] [PubMed] [Google Scholar]
Chien 1981
- Chien S. Haemorheology in disease: pathophysiological significance and therapeutic implications. Clinical Hemorheology 1981;1:419‐42. [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. [DOI] [PubMed] [Google Scholar]
Dexter 1997
- Dexter F, Hindman BJ. Effect of hemoglobin concentration on brain oxygenation in focal stroke: a mathematical modelling study. British Journal of Anaesthesia 1997;79:346‐51. [DOI] [PubMed] [Google Scholar]
Di Perri 1986
- Perri T, Guerrini M, Laghi Pasini F. Haemorheological changes associated with acute and chronic cerebrovascular disease. Royal Society of Medicine International Congress and Symposium Series 1986;100:33‐46. [Google Scholar]
ESO 2008
- European Stroke Organisation (ESO) Executive Committee, ESO Writing Committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovascular Diseases 2008;25(5):457‐507. [DOI] [PubMed] [Google Scholar]
Feigin 2003
- Feigin VL, Lawes CMM, Bennett DA, Anderson CS. Stroke epidemiology: a review of population‐based studies of incidence, prevalence, and case‐fatality in the late 20th century. Lancet Neurology 2003;2(1):43‐53. [DOI] [PubMed] [Google Scholar]
Ginsberg 2008
- Ginsberg MD. Neuroprotection for ischemic stroke: past, present and future. Neuropharmacology 2008;55(3):363‐89. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gottstein 1976
- Gottstein U, Seidlmeyer I, Heuss A. Treatment of acute cerebral ischemia with low‐molecular dextran. Results of a retrospective study. Deutsche Medizinische Wochenschrift 1976;101:223‐7. [DOI] [PubMed] [Google Scholar]
Gottstein 1981
- Gottstein U. Normovolemic and hypervolemic hemodilution in cerebrovascular ischemia. Bibliotheca Haematologica 1981;47:127‐38. [DOI] [PubMed] [Google Scholar]
Haass 1986
- Haass A, Kroemer H, Jäger H, Müller K, Decker I, Wagner EM, et al. Dextran 40 or HES 200/0.5? Hemorheology of the long‐term treatment of ischemic cerebral attacks. Deutsche Medizinische Wochenschrift 1986;111(44):1681‐6. [DOI] [PubMed] [Google Scholar]
Harrison 1981
- Harrison MJG, Pollock S, Kendall BE, Marshall J. Effect of hematocrit on carotid stenosis and cerebral infarction. Lancet 1981;ii:114‐5. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jauch 2013
- Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Peripheral Vascular Disease, Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44(3):870‐947. [DOI] [PubMed] [Google Scholar]
Kannel 1972
- Kannel WB, Gordon T, Wolf PA, McNamara P. Hemoglobin and the risk of cerebral infarction. The Framingham Study. Stroke 1972;3:409‐20. [DOI] [PubMed] [Google Scholar]
Kiyohara 1986
- Kiyohara Y, Ueda K, Hasuo Y, Fijii I, Yanai T, Wada J, et al. Hematocrit as a risk factor of cerebral infarction: long‐term prospective population survey in a Japanese rural community. Stroke 1986;17:687‐92. [DOI] [PubMed] [Google Scholar]
Kline 1991
- Kline RA, Negendank W, McCoy L, Berguer R. Beneficial effects of isovolemic hemodilution using a perfluorocarbon emulsion in a stroke model. American Journal of Surgery 1991;162:103‐6. [DOI] [PubMed] [Google Scholar]
Korosue 1988
- Korosue K, Ishida K, Matsuoka H, Nagao T, Tamaki N, Matsumoto S. Clinical, hemodynamic, and hemorheological effects of isovolemic hemodilution in acute cerebral infarction. Neurosurgery 1988;23:148‐53. [DOI] [PubMed] [Google Scholar]
Krepp 1984
- Krepp H‐P, Beez M, Bock P. Behandlung des akuten Hirninfarktes durch hypervolamische hamodilutionstherapie. Klinikarzt 1984;13:597‐607. [Google Scholar]
Krishnamurthi 2013
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor C, Bennett DA, on behalf of the Global Burden of Diseases, Injuries, Risk Factors Study 2010 (GBD 2010) and the GBD Stroke Experts Group. Global and regional burden of first‐ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. The Lancet Global Health 2013;1(5):e259‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kroemer 1987
- Kroemer H, Haass A, Muller K, Jager H, Wagner EM, Heimburg P, et al. Haemodilution therapy in ischemic stroke: plasma concentrations and plasma viscosity during long‐term infusion of dextran 40 or hydroxyethyl starch 200/0.5. European Journal of Clinical Pharmacology 1987;31:705‐10. [DOI] [PubMed] [Google Scholar]
Kusunoki 1981
- Kusunoki M, Kimura K, Nakamura M, Isaka Y, Yoneda S, Abe H. Effects of hematocrit variations on cerebral blood flow and oxygen transport in ischemic cerebrovascular disease. Journal of Cerebral Blood Flow and Metabolism 1981;1:413‐7. [DOI] [PubMed] [Google Scholar]
Lithner 1988
- Lithner F, Asplund K, Eriksson S, Hagg E, Strand T, Wester P‐O. Clinical characteristics in diabetic stroke patients. Diabetes and Metabolism 1988;14:15‐9. [PubMed] [Google Scholar]
Liu 2001
- Liu Y, Belayev L, Zhao W, Busto R, Belayev A, Ginsberg MD. Neuroprotective effect of treatment with human albumin in permanent focal cerebral ischemia: histopathology and cortical perfusion studies. European Journal of Pharmacology 2001;428:193‐201. [DOI] [PubMed] [Google Scholar]
Lozano 2012
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2095‐128. [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2008
- National Collaborating Centre for Chronic Conditions (UK). Stroke: National Clinical Guideline for Diagnosis and Initial Management of Acute Stroke and Transient Ischaemic Attack (TIA). National Institute for Health and Clinical Excellence: Guidance. London: Royal College of Physicians (UK), 2008. [PubMed] [Google Scholar]
Ott 1986
- Ott E. The clinical importance of haemorheological alteration in cerebrovascular disease. Royal Society of Medicine International Congress and Symposium Series 1986;100:25‐32. [Google Scholar]
Paulson 1971
- Paulson OB. Cerebral apoplexy (stroke). Pathogenesis, pathophysiology and therapy as illustrated by regional blood flow measurements. Stroke 1971;2:327‐60. [DOI] [PubMed] [Google Scholar]
Pearson 1978
- Pearson TC, Wetherley‐Mein G. Vascular occlusive episodes and venous haematocrit in primary proliferative polycythaemia. Lancet 1978;2:1219‐22. [DOI] [PubMed] [Google Scholar]
Popov 2000
- Popov VV, Molchanov IV, Karpunichev OB, Poliakov AU, Kuznetsova IV, Goldina OA, et al. Basic intensive care of ischemic cerebral stroke. Method of therapeutic hemodilution. Anesteziologiia i Reanimatologiia 2000;Jul‐Aug:44‐9. [PubMed] [Google Scholar]
Prajapati 2011
- Prajapati KD, Sharma SS, Roy N. Current perspectives on potential role of albumin in neuroprotection. Reviews of Neurosciences 2011;22(3):355‐63. [DOI] [PubMed] [Google Scholar]
RevMan 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Righetti 2004
- Righetti E, Celani MG, Cantisani TA, Sterzi R, Boysen G, Ricci S. Glycerol for acute stroke. Cochrane Database of Systematic Reviews 2004, Issue 2. [DOI: 10.1002/14651858.CD000096.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sandercock 2011
- Sandercock PAG, Soane T. Corticosteroids for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2011, Issue 9. [DOI: 10.1002/14651858.CD000064.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schneider 1985
- Schneider R, Hacke W, Kiesewetter H, Jung F. Haemodilution in acute ischemic insults. Comparative study on the clinical and haemorheological effectiveness of 10% HES 200/0,5 and Dextran 40 [Hamodilution bei akuten ischamischen Insulten. Vergleichende Studie zur klinischen und hamorheologischen Wirksamkeit von 10% HES 200/0,5 and Dextran 40]. Fortschritte der Medizin 1985;103:1031‐4. [PubMed] [Google Scholar]
Staedt 1986
- Staedt U, Genth KR, Gaa J, Ritz R. Hemodilution in patients with cerebrovascular ischemia, using low‐molecular dextran (Dex 40) and middle‐molecular weight hydroxyethyl starch (HES 200). Therapiewoche 1986;36(23):2485‐95. [Google Scholar]
Standl 2001
- Standl T. Haemoglobin‐based erythrocyte transfusion substitutes. Expert Opinion on Biological Therapy 2001;1:831‐43. [DOI] [PubMed] [Google Scholar]
Todd 1994
- Todd MM, Wu B, Maktabi M, Hindman BJ, Warner DS. Cerebral blood flow oxygen delivery during hypoxemia and hemodilution: role of arterial oxygen content. American Journal of Physiology 1994;267:H2026‐31. [DOI] [PubMed] [Google Scholar]
Tohgi 1978
- Tohgi H, Yamanouchi H, Murakami M, Kameyama M. Importance of the hematocrit as a risk factor in cerebral infarction. Stroke 1978;9:369‐74. [DOI] [PubMed] [Google Scholar]
Tsuda 1987
- Tsuda Y, Hartmann A, Weiland J, Solymosi L. Effect of hydroxyethyl starch and low molecular weight dextran on cerebral blood flow and hemorheology in normal baboons. In: Hartmann A, Kuschinsky W editor(s). Cerebral Ischemia and Hemorheology. Berlin: Springer‐Verlag, 1987:398‐407. [DOI] [PubMed] [Google Scholar]
Vorstrup 1989
- Vorstrup S, Andersen A, Juhler M, Brun B, Boysen G. Hemodilution increases cerebral blood flow in acute ischemic stroke. Stroke 1989;20:84‐9. [DOI] [PubMed] [Google Scholar]
Wood 1982
- Wood JH, Fleischer AS. Observations during hypervolemic hemodilution of patients with acute focal cerebral ischemia. JAMA 1982;248:2999‐3004. [PubMed] [Google Scholar]
Wood 1983
- Wood JH, Polyzoidis KS, Epstein CM, Gibby GL, Tindall GT. Improvement in cerebral blood flow and power spectral EEG after isovolemic hemodilution in stroke patients. Journal of Cerebral Blood Flow and Metabolism 1983;3:588‐9. [Google Scholar]
Wood 1985
- Wood JH, Kee DB Jr. Hemorheology of the cerebral circulation in stroke. Stroke 1985;16:765‐72. [DOI] [PubMed] [Google Scholar]