

Abstract
Much of the research in ingestive behavior has focused on the macronutrient composition of foods; however, these studies are incomplete, or could be misleading, if they do not consider the energy density (ED) of the diet under investigation. Lowering the ED (kcal/g) by increasing the volume of preloads without changing macronutrient content can enhance satiety and reduce subsequent energy intake at a meal. Ad libitum intake or satiation has also been shown to be influenced by ED when the proportions of macronutrients are constant. Since people tend to eat a consistent weight of food, when the ED of the available foods is reduced, energy intake is reduced. The effects of ED have been seen in adults of different weight status, sex, and behavioral characteristics, as well as in 3- to 5-year-old children. The mechanisms underlying the response to variations in ED are not yet well understood and data from controlled studies lasting more than several days are limited. However, both population-based studies and long-term clinical trials indicate that the effects of dietary ED can be persistent. Several clinical trials have shown that reducing the ED of the diet by the addition of water-rich foods such as fruits and vegetables was associated with substantial weight loss even when patients were not told to restrict calories. Since lowering dietary energy density could provide effective strategies for the prevention and treatment of obesity, there is a need for more studies of mechanisms underlying the effect and ways to apply these findings.
Keywords: calorie density, diets, energy density, energy intake, food intake, hunger, macronutrients, obesity, preloads, satiety, satiation, weight management
With the surge in the incidence of overweight and obesity, effective dietary strategies for weight management are needed. On the surface the issue is clear-cut: simply reduce energy intake below energy expenditure. There is, however, much debate and controversy over ways to achieve this goal. Variations in the proportions of macronutrients (carbohydrates, fat, and protein) in the diet have been proposed as a means to facilitate weight loss. Low-fat diets, low-carbohydrate diets, and high-protein diets have all been in vogue during the past 20 years. This focus on the macronutrients in the diet drives much of the basic and applied research in the study of ingestive behavior and has enhanced understanding of underlying mechanisms of hunger and satiety. However, studies of the effects of macronutrients are incomplete, or could be misleading, if they do not consider the energy density of the diet under investigation. The goal of this review is to summarize recent studies that have extended our understanding of the role of energy density in the control of food intake and to discuss some of the issues that require further investigation.
What is energy density?
Energy density is the amount of energy (calories or joules) in a particular weight of food. It is generally presented as the number of calories per gram of food (kcal/g). Energy density values, which are influenced by the macronutrient composition and moisture content of foods and beverages, range from 0 kcal/g to 9 kcal/g. Because of its high energy content, fat (9 kcal/g) influences energy density values more than carbohydrate or protein (4 kcal/g). Foods and beverages with a high fat content generally have a relatively high energy density; but a high moisture content lowers the energy density of foods, even those high in fat. Water lowers the energy density of foods because it contributes weight but not energy. Since beverages are primarily water, they tend to have a lower energy density than most foods.
If a person consumes a consistent weight of food, then even modest changes in energy density can have a significant impact on daily energy intake. For example, on a typical day an adult might consume 1200 g of food with an overall energy density of 1.8 kcal/g, giving an energy intake of 2160 kcal. If the average energy density of the diet was decreased by 0.1 kcal/g while the same weight of food was consumed, then the individual would ingest 2040 kcal. Thus, a relatively small change in the overall energy density of the diet would reduce energy intake by 120 kcal per day. Recent research has indicated that reductions in the energy density of foods can be used strategically to maintain satiety and to moderate energy intake.
Consumption of low-energy-dense preloads can enhance satiety
Satiety refers to the effects of food after eating has ended. To study satiety, a fixed amount of a defined food (a preload) is consumed; after an interval of time, the effect of the preload on subsequent test meal intake is measured. Satiety is also assessed by post-preload ratings of fullness using tools such as visual analog scales. The preloading paradigm has been used extensively to assess how foods and food components vary in their effects on satiety. Such studies have the potential to not only enhance understanding of biological and behavioral influences on satiety, but also could lead to the development of food products to help with weight management.
Studies employing preloads have indicated that there are numerous influences on satiety, encompassing not only the nutrient and energy content of foods, but also sensory and physical attributes, as well as the consumer’s previous experiences with the foods. Of particular interest to this review is whether satiety is affected by the energy density of foods. To test the independent effect of energy density, the energy and macronutrient content as well as the palatability of the preloads should be matched when the energy density is changed. This can be achieved by the addition of water to food which will increase the weight and volume, thus decreasing the energy density. In one study, decreasing the energy density of a milk-based preload by adding water and thus increasing the volume (300, 450, or 600 ml) led to a significant reduction in subsequent energy intake (1).
In another study, we determined whether drinking water as a beverage along with a meal had a similar effect on satiety as incorporating an equivalent amount of water into the food. On different test days, participants consumed no preload or one of three isoenergetic preloads varying in water content before an ad libitum test meal. The preloads were a chicken and rice casserole, the casserole served with a 10-ounce glass of water, or the casserole and the 10 ounces of water cooked together to make a soup. Participants consumed 26% less energy at lunch and rated themselves less hungry and fuller after consuming the soup than after either the casserole alone or the casserole served with water. This indicated that water can have a greater impact on satiety when incorporated into a food, thereby reducing its energy density, than when consumed as a beverage along with a food (2).
The mechanisms underlying the effects of reduced energy density and increased volume on satiety are likely complex and still not well understood. Cognitive and sensory factors related to the volume of food and beliefs about the satiating capacity of different foods are involved. We have shown, for example, that the declining hedonic response to a food as it is consumed (sensory-specific satiety) is affected more by the amount of food consumed than by its energy content (3). However, the energy density of food can also affect satiety when sensory cues are bypassed, as demonstrated in a study in which the volume and energy content of preloads infused intragastrically were varied independently. Increasing the volume of the infused preload, but not its energy content, enhanced satiety (4). Studies of gastric emptying in humans indicate that energy density has a greater effect than the macronutrient composition of foods (5, 6). Reducing the energy density of test foods slowed gastric emptying and this could be part of the explanation of the enhanced satiety. With the growing interest in the role of energy density in the control of energy intake, there is a need for systematic studies of basic physiologic responses to the energy density of foods; in particular, more studies are needed on the effects of the water content of foods and beverages on satiety mechanisms.
Preload characteristics that can moderate the effect of energy density
In order to systematically investigate the mechanisms underlying the influence of energy density on satiety, we need a better understanding of how other properties of foods moderate the effect. The response to variations in preload volume by the addition of water has not been consistent. Several studies have failed to find that adding water to soup preloads influences satiety (7, 8). Although negative findings are more difficult to interpret than those that are positive, one explanation that has been offered is that volume is more influential when preloads are large. Another possibility is that there may be a threshold concentration for nutrients in the gastrointestinal tract before volume alone affects satiety and energy intake (8). It is also likely that the type of macronutrients in the preload will influence satiety (9).
In addition, as the energy density of a food varies, its physical properties such as viscosity and texture are likely to change and this could affect chewing, oro-gastric handling of foods, and absorption. Effects on satiety of changes in the form of a food independent of other food properties can be tested with a food such as soup where the form can be varied simply by keeping ingredients separate in chunks or by blending them together to make a puree. We tested the effects on meal intake of consuming preloads of four different soups with the same energy density and containing the same ingredients: broth and vegetables served separately, chunky vegetable soup, chunky-pureed vegetable soup, or pureed vegetable soup (10). Consuming a low-energy-dense soup as a preload led to a significant reduction in test meal intake compared to consuming no preload (Figure 1). However, the type of soup did not significantly influence test meal intake. Overall, following the soup preloads, subjects reduced total energy intake at lunch by 20%. This finding does not preclude the possibility that food properties such as viscosity and texture could affect satiety, but it is likely that such influences are relatively small compared to that of energy density.
Figure 1.
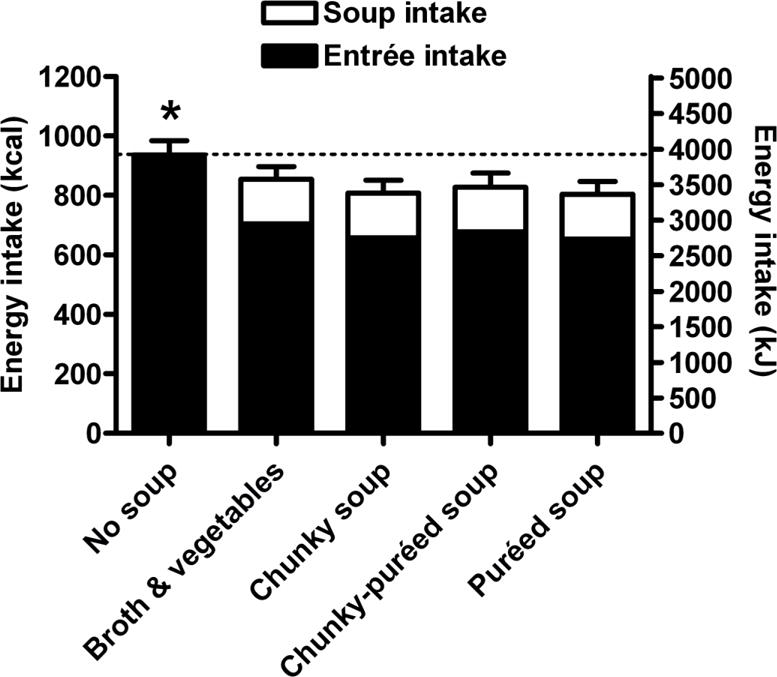
Mean (± SE) energy intake at lunch (soup + entrée intake) of 60 women and men in a study testing the effect of varying the form of soup on lunch intake. Subjects consumed significantly less total energy at lunch when soup was eaten as a first course, regardless of its form, compared to when no soup was eaten *(p < 0.0001) Reproduced with permission from Appetite (10).
Soup is a liquid that is perceived as a food and the perception of a preload as a food or as a beverage could have an effect on satiety. The question of whether energy in a liquid form affects satiety differently to that in a solid form is one of the most debated issues in ingestive behavior (11,12,13). Of interest to the current review is that, while soup is a low-energy-dense liquid food that increases satiety, other low-energy-dense liquids such as soda have been found in some studies to have little effect on satiety and to contribute additional energy to a meal (11, 14, 15). Such findings appear to contradict the suggestion that the water content of a preload is a critical determinant of satiety. It is possible that very dilute liquid calories or beverages composed of few nutrients, such as sugary drinks, fail to engage hunger mechanisms, and instead are recognized as beverages that influence thirst. However, not all data are consistent with this hypothesis. Some studies have found soda and more complex fluids such as milk to have similar effects on satiety (12,14). Indeed, several studies have indicated that solid foods do not always have a greater effect on satiety than liquids (12).
In studies comparing solids and liquids, variations in form have not been systematically disentangled from those related to energy density. Thus, we tested whether consumption of the same food in either a solid or liquid form had similar effects on satiety when the energy density was matched. On average, beverages are around ten-fold lower in energy density than foods because of their high water content, but it is possible to vary a food between solid and liquid states without changing the energy density. Fruit is well-suited to such an investigation since it is consumed in solid, pureed, and liquid forms that can be similar in energy density. We tested how consuming preloads of apples in different forms prior to a meal (whole apple, applesauce, and apple juice with and without added fiber) influences satiety and energy intake at a meal when matched for weight, energy content, energy density, and ingestion rate (16). We found that eating whole apple reduced lunch energy intake by 15% compared to no preload, and decreased energy intake compared to applesauce and both juices. Overall, whole apple increased satiety more than applesauce or apple juice (Figure 2). Adding naturally-occurring levels of fiber to juice did not enhance satiety. This study shows that when considering the impact of energy density on satiety, other properties of the preload such as its physical form must be considered since these could moderate the outcome.
Figure 2.
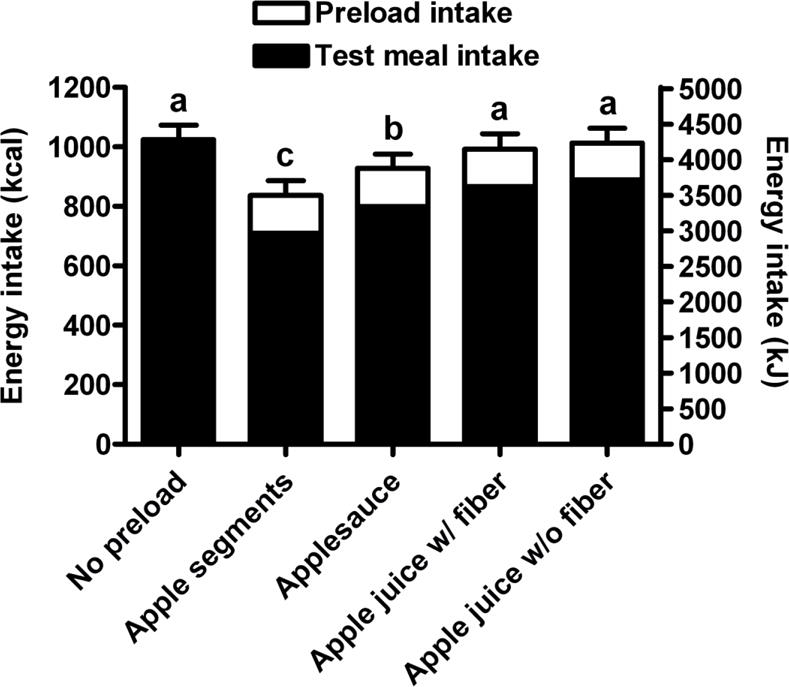
Mean (± SE) total energy intake at lunch (preload + test meal) for 58 subjects in a study testing the effects on satiety of apple preloads in different forms. Preloads were matched for weight, energy, energy density, and ingestion time; the apple segments, applesauce, and apple juice with fiber preloads were matched for fiber content. Means with different letters are significantly different (p<0.05) based on a mixed linear model with repeated measures. Reproduced with permission from Appetite (16).
The size of a preload can also influence the effect of energy density on satiety. For example, we found that the portion size and energy density of a preload of salad combined to influence meal intake. Subjects were required to consume a first course salad, which was varied in energy density and portion size on different days, followed by a main course of pasta (17). Compared to having no first course, a low-energy-dense salad as a first course led to a decrease in total energy intake at the meal. This reduction in energy intake was greater when subjects consumed the larger rather than the smaller low-energy-dense salad. Consuming either portion of the high-energy-dense salad increased energy intake at the meal. Thus, when assessing the effects of variations in the energy density of a preload it is important to understand that the outcome will be affected by the amount consumed as well as the total energy content.
In summary, the energy density of a preload can be used strategically to affect total energy intake in a meal. However, at present we have only a rudimentary understanding of the many variables that can influence the response to variations in preload energy density. These include properties of the preload and the test meal, timing of consumption, and hunger levels. In addition, little is known about whether effects of preload energy density are sustained beyond a single meal. Such basic studies should lead to a better understanding of the mechanisms underlying satiety and to the development of food-based strategies to enhance satiety.
Energy density and satiation: effects on ad libitum energy intake
Energy density can influence energy intake not only by enhancing satiety, but also through effects on ad libitum intake. Ad libitum intake is an indicator of satiation, or the processes leading to the termination of eating during a meal. The study of satiation is challenging because even slight differences in the palatability of the test foods could obscure effects on intake related to variations in meal components. Until recently, most studies of satiation focused on the influence of the macronutrient content of the diet. It was found, for example, that reducing the proportion of fat in the diet decreased energy intake even when palatability did not vary (18,19). In such studies dietary energy density also changed and it is therefore not clear whether satiation was affected by the proportions of macronutrients or by dietary energy density. It is possible, however, to separate these effects by adjusting the water content of foods. This can be achieved either by diluting foods or by adding low-energy, water-rich vegetables. Several studies have shown that when these techniques were used to hold energy density constant, even large variations in the proportion of energy from fat in the diet (20 to 60 %) had no significant influence on energy intake (20,21,22,23).
On the other hand, variations in the energy density of foods did influence ad libitum energy intake when the proportions of macronutrients were held constant (23,24). In a study in which energy density was manipulated, participants were served all of their meals for two days on three separate occasions (24). After consuming a standard breakfast, they freely consumed lunch and dinner entrees, which varied in energy density (low, medium, and high), along with compulsory side dishes. Variations in energy density were achieved by manipulating the proportion of vegetables and pasta in the meals; thus, low-energy-dense meals contained more water than those higher in energy density. The meals were rated as equally palatable and the macronutrient composition was similar across energy density manipulations. Even with a relatively large (30%) reduction in the energy density of the available foods, participants consumed a similar weight of food across conditions. Therefore, the cumulative energy intake over the two days was around 30% less in the lowest energy density condition compared to the highest. Despite differences in total energy intake between the diets, participants rated their hunger and fullness as similar, probably because they ate a consistent weight of food across conditions.
The available evidence from such controlled trials suggests that the effects of dietary energy density on energy intake are stronger than those related to variations in macronutrients. However, these lab-based studies have been criticized because of constraints imposed by the test situation; often participants could only adjust intake by eating more or less of the manipulated foods (25).While this probably does limit the potential for compensatory changes in intake, energy density has been shown to affect energy intake when only a portion of the diet is manipulated and participants can freely consume a variety of unmanipulated foods. In an experiment comparing obese and lean participants, energy intake was measured across a four-day period (23). Compulsory main course foods representing around 50% of each individual’s meal energy intake were manipulated in either energy density or fat content, and the palatability of the foods was matched. Overall, both lean and obese participants reduced energy intake of self-selected foods at meals by 16% when they consumed the low- compared to the high-energy-density main courses, whereas both groups failed to respond to differences in the fat content of the main courses. There was no tendency to compensate for the reduction in energy intake over the four-day period and ratings of hunger did not differ between the diets. Thus, the energy density of the diet affected satiation when only a portion of the diet was manipulated and the effect persisted over several days (23).
Do characteristics of the individual affect satiation?
Most of our understanding of the effects of dietary energy density comes from studies in young to middle-aged adults. In these studies, no systematic relationship has been demonstrated between subject characteristics such as weight status, dietary restraint, and disinhibition and the response to variations in energy density. It is of particular interest to determine whether the effect of energy density is robust across different age groups, since it is thought that the control of energy intake changes with age. It has been reported that young children are better at responding to the energy content of foods than adults (26), while elderly individuals are relatively insensitive to variations in energy (27). For example, when the energy density of foods available to hospitalized elderly patients was increased over 15 weeks there was a persistent increase in daily energy intake (28).
The suggestion that young children are responsive to variations in the energy content of foods is based primarily on studies showing that preschool children adjust their subsequent energy intake in response to the energy density of a preload. In some cases, children compensated for energy intake from the preload by reducing their intake of the main course, so that they consumed a consistent amount of total energy across meals (26,29,30). However, in other cases compensation has been incomplete with some children overcompensating for energy intake from the preload, and thus under-eating at the meal, and others under-compensating, and thus increasing meal energy intake (31,32,33). While these studies have shown that children can make some adjustments to their energy intake in response to the energy density of preloads, they do not indicate how children would respond to foods varying in energy density that are consumed ad libitum.
We have addressed this in several recent studies by offering children foods varying in energy density and allowing them to eat as much or as little as they like. In these tests of satiation, young children behaved similarly to adults. In a study in 5- to 6-year-olds (34), the energy density of a main course of macaroni and cheese was lowered by reducing the fat content. Despite the difference in the energy density, children, like adults, consumed a consistent weight of the entrée and of the other unvaried foods served at the meal so that they consumed significantly less energy from the entrée and from the entire meal. Comparable findings have been reported in a younger sample of children (2–5 years old) using a similar protocol and entrée (35).
Children responded in a similar manner when the energy density of a pasta dish was reduced not only by lowering the fat content but also by adding extra vegetables (36). Preschool children again consumed a consistent weight of both versions of the pasta and the other items offered at the meal. Therefore, they ate significantly less energy from the pasta and the entire meal when the energy density of the pasta was reduced. The addition of extra vegetables did not affect preference ratings, but had the beneficial effect of increasing vegetable intake.
Thus, reductions in energy density lowered the energy intake of preschool children at a single meal. However, if children are sensitive to variations in energy content, they may compensate when the manipulation is extended over several days. This possibility was tested in children in a childcare facility that were provided with all of their meals (breakfast, lunch, afternoon snack, dinner, and evening snack) for two days in two experimental sessions (37). During one session, the foods and beverages served at breakfast, lunch, and afternoon snack on both days were reduced in energy density by 19% to 33%. Decreases in energy density were achieved using various strategies, such as reducing fat and sugar content and increasing fruit and vegetable content. Similar to findings from single-meal studies, the children ate a consistent weight of foods and beverages over two days in both sessions, and therefore, they consumed significantly less energy when served the lower-energy-dense versions (Figure 3).
Figure 3.
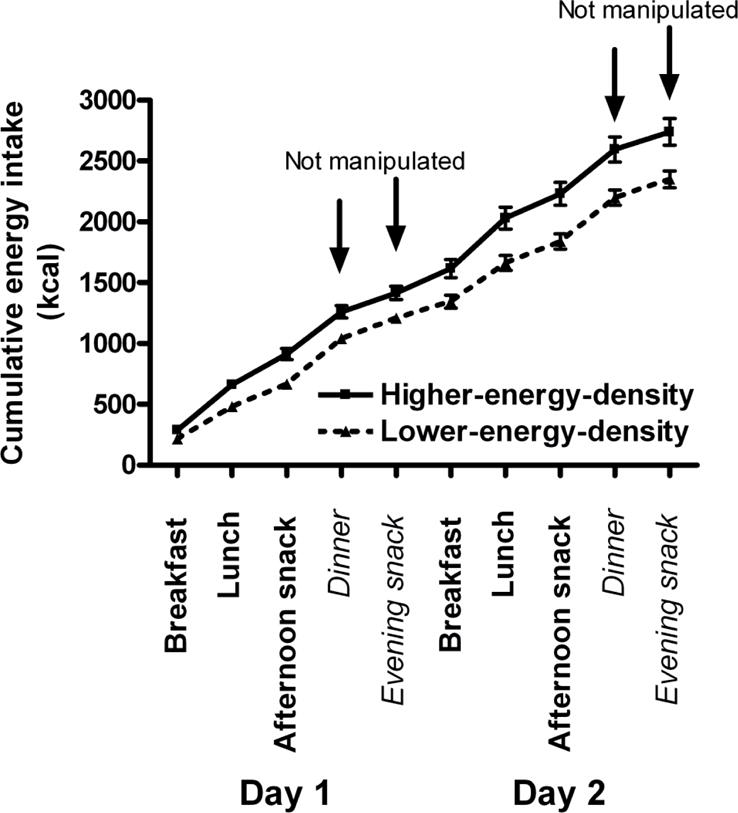
Mean (± SE) cumulative energy intake over two days in 26 preschool-age children who were served foods and beverages that were lower in energy density at breakfast, lunch, and afternoon snack. There was a significant effect of energy density on cumulative energy intake starting at breakfast on day 1 and accumulating over the course of the two days when assessed by a mixed linear model (p < 0.01) Reproduced with permission from the American Journal of Clinical Nutrition (37).
Since energy density has a persistent effect on children’s energy intake, reductions in energy density could possibly be used strategically to prevent excess energy intake in young children. However, studies are needed to determine whether over periods longer than several days children will sense an energy deficit, or learn that foods reduced in energy density are not satisfying and adjust their energy intake. Interestingly, while there have been no long-term interventions examining children’s responses to reductions in energy density, there have been studies showing that increasing the energy density of foods provided to malnourished children is associated with persistent increases in energy intake and weight gain (38).
Several longitudinal studies have determined whether there is an association between the energy density of children’s freely chosen diets and their body fatness. One study examined food records of 5- to 9-year-old children and found that an energy-dense, low-fiber, high-fat eating pattern was associated with higher fat mass and greater odds of excess adiposity 2 or 4 years later (39). Another study examined the relationship between reported dietary energy density and change in body fat as children (6 to 8 years of age) transitioned into adolescence (13 to 17 years of age). Energy density of the diet at baseline (calculated with all or most beverages excluded) was associated with change in fat mass index (body fat normalized for height). The inclusion of beverages in the calculation of energy density attenuated this relationship. No relationship was found between dietary energy density calculated by any method and change in the percentage of body fat, body mass index, or waist circumference. The authors conclude that the methods used to calculate both energy density and obesity risk affect the conclusions about associations between dietary energy density and fat gain during childhood (40).
How does energy density affect satiation?
The effects of energy density are robust, affecting energy intake in children, adults of a wide range of ages, and individuals with different weight status and with various levels of concern about what they eat. When presented with different versions of foods that are similar in palatability, but vary in energy density, the typical response is to consume a consistent amount of food. This suggests that intake during a meal depends upon cognitive factors related to previous experiences with foods and with beliefs about amounts appropriate to satisfy hunger. During a meal the physiologic cues associated with differences in energy density may not have time to be engaged, so intake will instead be determined by more immediate cues related to the amount consumed. The constancy of the amount consumed may also relate to sensory-specific satiety. This decline in pleasantness of a food as it is consumed limits consumption, and sensory-specific satiety has been shown to depend more upon the amount of food consumed than its energy content (3,41).
While cognitive and sensory factors may override physiologic responses to variations in energy density during a meal, a critical question is whether compensation will occur over time. Westerterp-Plantenga (42,43) has argued that decreases in energy intake associated with reductions in energy density are short-term, especially if the reduction is achieved by the addition of water to the diet. The rationale is that while changes in the volume of food consumed can affect pre-absorptive mechanisms, which will affect satiety in the short term, they will not have a persistent influence on post-absorptive mechanisms which respond to variations in the energy content of food. Data to confirm or refute this hypothesis are needed. While there have been a number of controlled studies testing the effects of energy density on energy intake over a day or two, little is known about the effects over longer periods. Several studies in which the reduction in energy density was achieved by reducing the fat content of foods indicate that energy intake was reduced for periods of 5 days (44) to 11 weeks (19). Reductions in energy density through the use of the fat substitute olestra led to reduced energy consumption when the diet was manipulated over nine months (45). In two controlled feeding studies, the influence of energy density was assessed when the proportions of macronutrients were held constant. In one, we showed that the effects of changes in the energy density of a portion of the diet persisted over 4 days (23). In another study, 6 men showed persistent effects when all of the available foods were varied in energy density over 14 days (25). Clearly, more long-term controlled studies are needed to understand whether responses to energy density are sustained or whether physiologic or learned responses lead to compensatory behavior.
Energy density and body weight
Another way to examine the persistence of any influence that dietary energy density has on energy intake is to determine whether the energy density of the diet is associated with body weight status. Some population-based studies have shown that normal-weight adults report consuming diets with a lower energy density than obese individuals (46). Furthermore, dietary energy density was associated with the amount of weight gained over an eight-year period in a prospective study of over 50,000 middle-aged women (47). While these data suggest that dietary energy density could be a determinant of weight status, such epidemiologic studies cannot indicate causality. Furthermore, the significance of such associations depends upon whether or not different types of beverages are included in the calculation of energy density (48, 49). Because of their high water content, beverages can have a disproportionate impact on energy density. Agreement is needed upon the appropriate methods for exploring the influence of energy density on energy intake and body weight in free-living individuals (40,48,49). Decisions about whether or not to include caloric or non-caloric beverages in the calculation of energy density could be made more strategically if we better understood how different types of beverages influence hunger and thirst mechanisms.
Several year-long clinical trials also indicate that encouraging people to consume low-energy-dense foods affects weight loss. In one trial of 200 overweight men and women, we tested the efficacy of incorporating either a low- or high-energy dense food into a reduced-energy diet. We found that the reduction in dietary energy density was the main predictor of weight loss during the first two months of the study. Daily incorporation of a low-energy-dense food (soup) into a reduced-energy diet increased the magnitude of the weight loss and helped participants to maintain this loss (50).
In a second trial, we tested the effect of two strategies to reduce the energy density of the diet on weight loss in 97 obese women (51). One group was counseled to increase their intake of water-rich foods, such as fruits and vegetables, and to reduce dietary fat. A comparison group was counseled to restrict portions and to reduce dietary fat. Analysis of participants completing the study showed that both groups reduced the energy density of their diets, and both groups lost weight. However, after 12 months, the group counseled to eat more fruits and vegetables had a greater reduction in the energy density of their diet and lost more weight than the group told to reduce fat and restrict portions (17.4 vs. 14.1 lb). Over the course of the year, participants who ate the lower-energy-dense diet (higher in fruits and vegetables) reported consuming an average of 25% more food and reported less hunger than those in the comparison group.
While additional data from large scale clinical trials of dietary energy density are needed, a secondary analysis of the results from a multi-center intervention (PREMIER) indicates that changes in dietary energy density after six months were related to changes in body weight (52). Participants received one of three life-style interventions to reduce blood pressure that included information on physical activity, diet, and weight loss. Since each intervention group experienced a decline in energy density and body weight, analyses were conducted by classifying participants into tertiles based on the magnitude of change in energy density after six months. Participants with a relatively large reduction in energy density lost more weight (13 lb), than those with a modest reduction (9 lb) or those with a slight reduction or increase in energy density (5 lb). In addition to weight loss, reductions in energy density were associated with improved diet quality, indicating that this is a healthy strategy for weight management (53). Furthermore, participants with both large and modest decreases in energy density increased the amount of food they consumed (Figure 4). Increasing the amount of food consumed while decreasing energy intake could contribute to the long-term acceptability of a low-energy-dense eating pattern since it could help to control hunger.
Figure 4.
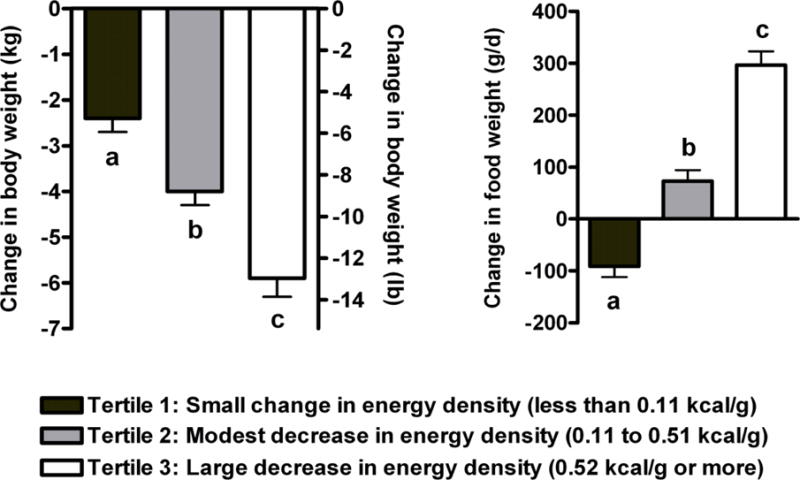
Mean (± SE) change in body weight and change in daily weight of food consumed after six months of intervention in 658 participants in the PREMIER trial. Participants were classified into tertiles based on the magnitude of change in dietary energy density. Those with a large reduction in energy density lost significantly more weight than those with a modest reduction or a slight reduction or increase in energy density. Participants with either a large or modest decrease in energy density significantly increased the amount of food they consumed. Values with different superscript letters are significantly different (p < 0.05) using ANOVA with a general linear model adjustment for baseline values followed by a Tukey-Kramer adjustment for multiple comparisons (52).
Another recent study examined the relationship between dietary energy density and weight change over a period of six years (54) in 186 young women. Of particular interest was that the reported energy density of the foods they consumed remained unchanged over the six years. However, body weight was not stable and those reporting a higher energy density gained two and a half times as much weight as those reporting a lower energy density (14 lb vs. 5.5 lb). Consistent with previous research, women eating the diets lower in energy density reported eating less energy but a greater weight of food and their diets were of higher quality than those of women eating a higher-energy-dense diet.
Relationships between dietary energy density and the maintenance of lost weight have not been extensively investigated. Greene and colleagues (55) examined energy density values two years after participation in a weight loss program that encouraged consumption of low-energy-dense foods. They found that individuals who maintained weight loss reported eating a lower-energy-dense diet than those who regained 5% or more of their body weight. In another study, men and women who had significant weight loss were given 10 to 14 sessions teaching the principles of low-energy-density eating. Results indicated that participants did well at reducing the energy density of their diets and maintaining their weight loss during the period when the treatment sessions were implemented. However, when treatment ended they had difficulty incorporating the strategies into their home environments. For example, they did not increase their intake of fruits and vegetables (56).
Additional long-term studies are required to understand the impact of diets reduced in energy density on both weight loss and weight maintenance. Such studies will need to pay particular attention to the challenges consumers face in order to make sustainable changes in the energy density of their diets. In the current food environment, many will find it difficult to make appropriate choices, since foods that are low in energy density but high in nutrient density are often expensive and not as readily available as those high in energy density (57,58). A better understanding of behaviors that will help consumers make long-term changes that reduce the energy density of their diets is urgently needed (59).
Conclusion
In recent years dietary energy density has emerged as an important influence on energy intake; however, our understanding of how energy density affects satiety and satiation is limited. Studies that have been conducted indicate that these effects are complex and include both psychological and physiological mechanisms. Despite this complexity, dietary energy density needs to be explored further since it not only has robust effects on intake, but also can moderate the influence of other dietary factors. Increased knowledge of how energy density influences energy intake could lead to effective strategies to enhance satiety and to moderate energy intake.
Acknowledgments
This research was supported by NIH grants R37DK039177 and R01DK059853, and by the Robert Wood Johnson Foundation.
References
- 1.Rolls BJ, Castellanos VH, Halford JC, Kilara A, Panyam D, Pelkman CL, Smith GP, Thorwart ML. Volume of food consumed affects satiety in men. Am J Clin Nutr. 1998;67:1170–1177. doi: 10.1093/ajcn/67.6.1170. [DOI] [PubMed] [Google Scholar]
- 2.Rolls BJ, Bell EA, Thorwart ML. Water incorporated into a food but not served with a food decreases energy intake in lean women. Am J Clin Nutr. 1999;70:448–455. doi: 10.1093/ajcn/70.4.448. [DOI] [PubMed] [Google Scholar]
- 3.Bell EA, Roe LS, Rolls BJ. Sensory-specific satiety is affected more by volume than by energy content of a liquid food. Physiol Behav. 2003;78:593–600. doi: 10.1016/s0031-9384(03)00055-6. [DOI] [PubMed] [Google Scholar]
- 4.Rolls BJ, Roe LS. Effect of the volume of liquid food infused intragastrically on satiety in women. Physiol Behav. 2002;76:623–631. doi: 10.1016/s0031-9384(02)00801-6. [DOI] [PubMed] [Google Scholar]
- 5.Hunt JN, Stubbs DF. The volume and energy content of meals as determinants of gastric emptying. J Physiol. 1975;245:209–225. doi: 10.1113/jphysiol.1975.sp010841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Calbet JA, MacLean DA. Role of caloric content on gastric emptying in humans. J Physiol. 1997;498:553–559. doi: 10.1113/jphysiol.1997.sp021881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gray R, French S, Robinson T, Yeomans M. Dissociation of the effects of preload volume and energy content on subjective appetite and food intake. Physiol Behav. 2002;76:57–64. doi: 10.1016/s0031-9384(02)00675-3. [DOI] [PubMed] [Google Scholar]
- 8.Gray RW, French SJ, Robinson TM, Yeomans MR. Increasing preload volume with water reduces rated appetite but not food intake in healthy men even with minimum delay between preload and test meal. Nutr Neurosci. 2003;6:29–37. doi: 10.1080/1028415021000056032. [DOI] [PubMed] [Google Scholar]
- 9.St-Onge MP, Rubiano F, DeNino WF, Jones A, Jr, Greenfield D, Ferguson PW, Akrabawi S, Heymsfield SB. Added thermogenic and satiety effects of a mixed nutrient vs a sugar-only beverage. Int J Obes Relat Metab Disord. 2004;28:248–253. doi: 10.1038/sj.ijo.0802560. [DOI] [PubMed] [Google Scholar]
- 10.Flood JE, Rolls BJ. Soup preloads in a variety of forms reduce meal energy intake. Appetite. 2007;49:626–634. doi: 10.1016/j.appet.2007.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Almiron-Roig E, Chen Y, Drewnowski A. Liquid calories and the failure of satiety: how good is the evidence? Obes Rev. 2003;4:201–212. doi: 10.1046/j.1467-789x.2003.00112.x. [DOI] [PubMed] [Google Scholar]
- 12.Mattes R. Fluid calories and energy balance: the good, the bad, and the uncertain. Physiol Behav. 2006;89:66–70. doi: 10.1016/j.physbeh.2006.01.023. [DOI] [PubMed] [Google Scholar]
- 13.Drewnowski A, Bellisle F. Liquid calories, sugar, and body weight. Am J Clin Nutr. 2007;85:651–661. doi: 10.1093/ajcn/85.3.651. [DOI] [PubMed] [Google Scholar]
- 14.DellaValle DM, Roe LS, Rolls BJ. Does the consumption of caloric and non-caloric beverages with a meal affect energy intake? Appetite. 2005;44:187–193. doi: 10.1016/j.appet.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 15.Flood JE, Rolls BJ, Roe LS. The effect of increased beverage portion size on energy intake at a meal. J Am Diet Assoc. 2006;106:1984–1990. doi: 10.1016/j.jada.2006.09.005. [DOI] [PubMed] [Google Scholar]
- 16.Flood-Obbagy JE, Rolls BJ. The effect of fruit in different forms on energy intake and satiety at a meal. Appetite. 2009 doi: 10.1016/j.appet.2008.12.001. NIHMSID# 97426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rolls BJ, Roe LS, Meengs JS. Salad and satiety: energy density and portion size of a first course salad affect energy intake at lunch. J Am Diet Assoc. 2004;104:1570–1576. doi: 10.1016/j.jada.2004.07.001. [DOI] [PubMed] [Google Scholar]
- 18.Lissner L, Levitsky DA, Strupp BJ, Kalkwarf HJ, Roe DA. Dietary fat and the regulation of energy intake in human subjects. Am J Clin Nutr. 1987;46:886–892. doi: 10.1093/ajcn/46.6.886. [DOI] [PubMed] [Google Scholar]
- 19.Kendall A, Levitsky DA, Strupp BJ, Lissner L. Weight loss on a low-fat diet: consequence of the imprecision of the control of food intake in humans. Am J Clin Nut. 1991;53:1124–1129. doi: 10.1093/ajcn/53.5.1124. [DOI] [PubMed] [Google Scholar]
- 20.van Stratum P, Lussenburg RN, van Wezel LA, Vergroesen AJ, Cremer HD. The effect of dietary carbohydrate:fat ratio on energy intake by adult women. Am J Clin Nutr. 1978;31:206–212. doi: 10.1093/ajcn/31.2.206. [DOI] [PubMed] [Google Scholar]
- 21.Stubbs RJ, Ritz P, Coward WA, Prentice AM. Covert manipulation of the ratio of dietary fat to carbohydrate and energy density: effect on food intake and energy balance in free-living men eating ad libitum. Am J Clin Nutr. 1995;62:330–337. doi: 10.1093/ajcn/62.2.330. [DOI] [PubMed] [Google Scholar]
- 22.Saltzman E, Dallal GE, Roberts SB. Effect of high-fat and low-fat diets on voluntary energy intake and substrate oxidation: studies in identical twins consuming diets matched for energy density, fiber and palatability. Am J Clin Nutr. 1997;66:1332–1339. doi: 10.1093/ajcn/66.6.1332. [DOI] [PubMed] [Google Scholar]
- 23.Rolls BJ, Bell EA, Castellanos VH, Chow M, Pelkman CL, Thorwart ML. Energy density but not fat content of foods affected energy intake in lean and obese women. Am J Clin Nutr. 1999;69:863–871. doi: 10.1093/ajcn/69.5.863. [DOI] [PubMed] [Google Scholar]
- 24.Bell EA, Castellanos VH, Pelkman CL, Thorwart ML, Rolls BJ. Energy density of foods affects energy intake in normal-weight women. Am J Clin Nutr. 1998;67:412–420. doi: 10.1093/ajcn/67.3.412. [DOI] [PubMed] [Google Scholar]
- 25.Stubbs RJ, Johnstone AM, O’Reilly LM, Barton K, Reid C. The effect of covertly manipulating the energy density of mixed diets on ad libitum food intake in ‘pseudo free-living’ humans. Int J Obes. 1998;22:980–987. doi: 10.1038/sj.ijo.0800715. [DOI] [PubMed] [Google Scholar]
- 26.Birch LL, Deysher M. Caloric compensation and sensory specific satiety: evidence for self-regulation of food intake by young children. Appetite. 1986;7:323–331. doi: 10.1016/s0195-6663(86)80001-0. [DOI] [PubMed] [Google Scholar]
- 27.Rolls BJ, Drewnowski A. Diet and nutrition. In: Birren JE, editor. Encyclopedia of Gerontology: Age, Aging, and the Aged. 2. Oxford, UK: Elsevier Inc.; 2007. pp. 417–427. [Google Scholar]
- 28.Odlund Olin A, Armyr I, Soop M, Jerstrom S, Classon I, Cederholm T, Ljunggren G, Ljungqvist O. Energy-dense meals improve energy intake in elderly residents in a nursing home. Clin Nutr. 2003;22:125–131. doi: 10.1054/clnu.2002.0610. [DOI] [PubMed] [Google Scholar]
- 29.Birch LL, Deysher M. Conditioned and unconditioned caloric compensation: evidence for self-regulation of food intake in young children. Learn Motiv. 1985;16:341–355. [Google Scholar]
- 30.Hetherington M, Wood C, Lyburn SC. Response to energy dilution in the short term: evidence of nutritional wisdom in young children? Nutr Neurosci. 2000;3:321–329. doi: 10.1080/1028415X.2000.11747329. [DOI] [PubMed] [Google Scholar]
- 31.Birch LL, McPhee LS, Bryant JL, Johnson SL. Children’s lunch intake: effects of midmorning snacks varying in energy density and fat content. Appetite. 1993;20:83–94. doi: 10.1006/appe.1993.1011. [DOI] [PubMed] [Google Scholar]
- 32.Johnson SL, Birch LL. Parents’ and children’s adiposity and eating style. Pediatrics. 1994;94:653–661. [PubMed] [Google Scholar]
- 33.Cecil JE, Palmer CN, Wrieden W, Murrie I, Bolton-Smith C, Watt P, Wallis DJ, Hetherington MM. Energy intakes of children after preloads: adjustment, not compensation. Am J Clin Nutr. 2005;82:302–308. doi: 10.1093/ajcn.82.2.302. [DOI] [PubMed] [Google Scholar]
- 34.Fisher JO, Liu Y, Birch LL, Rolls BJ. Effects of portion size and energy density on young children’s intake at a meal. Am J Clin Nutr. 2007;86:174–179. doi: 10.1093/ajcn/86.1.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Leahy KE, Birch LL, Rolls BJ. Reducing the energy density of an entrée decreases children’s energy intake at lunch. J Am Diet Assoc. 2008;108:41–48. doi: 10.1016/j.jada.2007.10.015. [DOI] [PubMed] [Google Scholar]
- 36.Leahy KE, Birch LL, Fisher JO, Rolls BJ. Reductions in entrée energy density increase children’s vegetable intake and reduce energy intake. Obesity. 2008;16:1559–1565. doi: 10.1038/oby.2008.257. [DOI] [PubMed] [Google Scholar]
- 37.Leahy KE, Birch LL, Rolls BJ. Reducing the energy density of multiple meals decreases the energy intake of preschool-age children. Am J Clin Nutr. 2008;88:1459–1468. doi: 10.3945/ajcn.2008.26522. [DOI] [PubMed] [Google Scholar]
- 38.Traore T, Vieu MC, Alfred TS, Serge T. Effects of the duration of the habituation period on energy intakes from low and high energy density gruels by Burkinabe infants living in free conditions. Appetite. 2005;45:279–286. doi: 10.1016/j.appet.2005.07.001. [DOI] [PubMed] [Google Scholar]
- 39.Johnson L, Mander AP, Jones LR, Emmett PM, Jebb SA. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am J Clin Nutr. 2008;87:846–854. doi: 10.1093/ajcn/87.4.846. [DOI] [PubMed] [Google Scholar]
- 40.McCaffrey TA, Rennie KL, Kerr MA, Wallace JM, Hannon-Fletcher MP, Coward WA, Jebb SA, Livingstone MB. Energy density of the diet and change in body fatness from childhood to adolescence; is there a relation? Am J Clin Nutr. 2008;87:1230–1237. doi: 10.1093/ajcn/87.5.1230. [DOI] [PubMed] [Google Scholar]
- 41.Miller DL, Bell EA, Pelkman CL, Peters JC, Rolls BJ. Effects of dietary fat, nutrition labels, and repeated consumption on sensory-specific satiety. Physiol Behav. 2000;71:153–158. doi: 10.1016/s0031-9384(00)00319-x. [DOI] [PubMed] [Google Scholar]
- 42.Westerterp-Plantenga MS. Effects of energy density of daily food intake on long-term energy intake. Physiol Behav. 2004;81:765–771. doi: 10.1016/j.physbeh.2004.04.030. [DOI] [PubMed] [Google Scholar]
- 43.Westerterp-Plantenga MS. Modulatory factors in the effect of energy density on energy intake. Br J Nutr. 2004;92(Suppl 1):S35–S39. doi: 10.1079/bjn20041140. [DOI] [PubMed] [Google Scholar]
- 44.Duncan KH, Bacon JA, Weinsier RL. The effects of high and low energy density diets on satiety, energy intake, and eating time of obese and nonobese subjects. Am J Clin Nutr. 1983;37:763–767. doi: 10.1093/ajcn/37.5.763. [DOI] [PubMed] [Google Scholar]
- 45.Bray GA, Lovejoy JC, Most-Windhauser M, Smith SR, Volaufova J, Denkins Y, de Jonge L, Rood J, Lefevre M, Eldridge AL, Peters JC. A 9-mo randomized clinical trial comparing fat-substituted and fat-reduced diets in healthy obese men: the Ole Study. Am J Clin Nutr. 2002;76:928–934. doi: 10.1093/ajcn/76.5.928. [DOI] [PubMed] [Google Scholar]
- 46.Ledikwe JH, Blanck HM, Kettel-Khan L, Serdula M, Seymour JD, Tohill BC, Rolls BJ. Dietary energy density is associated with energy intake and weight status in US adults. Am J Clin Nutr. 2006;83:1362–1368. doi: 10.1093/ajcn/83.6.1362. [DOI] [PubMed] [Google Scholar]
- 47.Bes-Rastrollo M, van Dam RM, Martinez-Gonzalez MA, Li TY, Sampson LL, Hu FB. Prospective study of dietary energy density and weight gain in women. Am J Clin Nutr. 2008;88:769–777. doi: 10.1093/ajcn/88.3.769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Cox DN, Mela DJ. Determination of energy density of freely selected diets: methodological issues and implications. Int J Obes Relat Metab Disord. 2000;24:49–54. doi: 10.1038/sj.ijo.0801084. [DOI] [PubMed] [Google Scholar]
- 49.Ledikwe JH, Blanck HM, Kettel-Khan L, Serdula MK, Seymour J, Tohill BC, Rolls BJ. Dietary energy density determined by eight calculation methods in a nationally representative United States population. J Nutr. 2005;135:273–278. doi: 10.1093/jn/135.2.273. [DOI] [PubMed] [Google Scholar]
- 50.Rolls BJ, Roe LS, Beach AM, Kris-Etherton PM. Provision of foods differing in energy density affects long-term weight loss. Obes Res. 2005;13:1052–1060. doi: 10.1038/oby.2005.123. [DOI] [PubMed] [Google Scholar]
- 51.Ello Martin JA, Roe LS, Ledikwe JH, Beach AM, Rolls BJ. Dietary energy density in the treatment of obesity: a year-long trial comparing 2 weight-loss diets. Am J Clin Nutr. 2007;85:1465–1477. doi: 10.1093/ajcn/85.6.1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ledikwe JH, Rolls BJ, Smiciklas-Wright H, Mitchell DC, Ard JD, Champagne C, Karanja N, Lin PH, Stevens VJ, Appel LJ. Reductions in dietary energy density are associated with weight loss in overweight and obese participants in the PREMIER trial. Am J Clin Nutr. 2007;85:1212–1221. doi: 10.1093/ajcn/85.5.1212. [DOI] [PubMed] [Google Scholar]
- 53.Ledikwe JH, Blanck HM, Khan LK, Serdula MK, Seymour JD, Tohill BC, Rolls BJ. Low-energy-density diets are associated with high diet quality in adults in the United States. J Am Diet Assoc. 2006;106:1172–1180. doi: 10.1016/j.jada.2006.05.013. [DOI] [PubMed] [Google Scholar]
- 54.Savage JS, Marini M, Birch LL. Dietary energy density predicts women’s weight change over 6 y. Am J Clin Nutr. 2008;88:677–684. doi: 10.1093/ajcn/88.3.677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Greene LF, Malpede CZ, Henson CS, Hubbert KA, Heimburger DC, Ard JD. Weight maintenance 2 years after participation in a weight loss program promoting low-energy density foods. Obesity. 2006;14:1795–1801. doi: 10.1038/oby.2006.207. [DOI] [PubMed] [Google Scholar]
- 56.Lowe MR, Tappe KA, Annunziato RA, Riddell LJ, Coletta MC, Crerand CE, Didie ER, Ochner CN, McKinney S. The effect of training in reduced energy density eating and food self-monitoring accuracy on weight loss maintenance. Obesity. 2008;16:2016–2023. doi: 10.1038/oby.2008.270. [DOI] [PubMed] [Google Scholar]
- 57.Rolls BJ, Drewnowski A, Ledikwe JH. Changing the energy density of the diet as a strategy for weight management. J Am Diet Assn. 2005;105:S98–S103. doi: 10.1016/j.jada.2005.02.033. [DOI] [PubMed] [Google Scholar]
- 58.Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87:1107–1117. doi: 10.1093/ajcn/87.5.1107. [DOI] [PubMed] [Google Scholar]
- 59.Ledikwe JH, Rolls BJ. Properties of foods and beverages that influence energy intake and body weight. In: Coulston A, Boushey C, editors. Nutrition in the Prevention and Treatment of Disease. 2. Burlington, MA: Elsevier Inc.; 2008. pp. 469–481. [Google Scholar]