

Abstract
Childhood obesity is now a global problem throughout the world. The major factors affecting weight regulation and the development of obesity in children are the result of a large number of biological, behavioral, social, environmental, and economic factors and the complex interactions between them that promote a positive energy balance. The changes in the dietary habits with the adoption of sedentary life style increases manifold obesity-related diseases and their complications. An obese child later on grows up to become an obese adult. Therefore, the role of primary prevention along with methodical diet control, behavioral changes, and physical activity are the important strategies against the battle of childhood obesity.
Keywords: Childhood, obesity, prevention
INTRODUCTION
Childhood obesity in developed as well as developing countries has now reached epidemic levels. About 70% of obese adolescents grow up to become obese adults.[1,2,3] Over the last 20-30 years, however, increasingly high rates of overweight and obesity have been reported irrespective of the socioeconomic and income status.[4,5,6] There is also increasing evidence of plateauing in some age groups in developed countries in Europe, USA[7] and Australia.[8] The factors participating in weight regulation and the development of obesity in children include genetic, environmental factors, and developmental influences ("metabolic programming" or epigenetics). The relative importance of each of these mechanisms is the subject of ongoing research and probably varies considerably between individuals and populations. The rapidly changing dietary habits along with the adoption of sedentary lifestyle increases enormously the obesity-related non-communicable diseases like insulin resistance, type 2 diabetes mellitus, metabolic syndrome, etc., In developed countries, it is seen that greater social inequality is associated with increase chance of obesity contrary to developing countries.[9] Once obesity is established, it is very difficult to reverse through interventions.[10] In this context, the role of primary prevention is of paramount importance besides incorporating strategies of behavioral changes, diet control, and physical activity.
DEFINITION OF THE PROBLEM
The criteria for assessing childhood obesity have been the subject of debate and research. Although definition of obesity and overweight has changed over time,[11,12] it can be defined as an excess of Body Fat (BF). The current expert opinion recommends the use of body mass index (BMI) cutoff points to determine the weight status. Now, the measurement of BMI percentile for age and gender is the most practical tool for clinicians to identify and track overweight and obesity.[13,14,15] A rapid increase in weight-for-height or BMI is an important predictor of future obesity even in children who are currently within a healthy weight category.
BMI percentiles are grouped into the following categories:
Overweight: BMI 85th to 95th percentile
Obese: BMI ≥ 95th percentile
Severe obesity: BMI ≥ 99th percentile, or > 120 percent of the 95th percentile.
Other methods for measuring obesity or adiposity include dual energy x-ray absorptiometry (DEXA) and air displacement plethysmography. These techniques measure fat mass directly but are too cumbersome and expensive for clinical use. Use of waist circumference and skin-fold thickness measurements is limited by discrepancies in normative data, and they are not accurate indices of body fat in many patients.[16,17,18]
The commonly used BMI percentiles are Centers for Disease Control and Prevention (CDC) BMI percentiles[19] , International Obesity Task Force (IOTF) cutoffs[11] , World Health Organization (WHO) growth standards (1995)[12,20] , New WHO growth standards in preschool children (2006),[21] and WHO growth reference curves.[22]
Overweight and obesity in childhood are known to have significant impact on both physical and psychosocial health.[4]
Assessment of comorbidities of childhood obesity
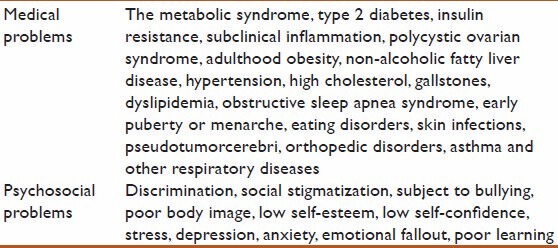
As a lot of comorbidities are associated with obesity [Table 1], a thorough physical examination is mandatory and it should include the review of linear growth (height velocity) and blood pressure.[23,24] Periodic measurement of a fasting lipid profile, hemoglobin A1c or fasting glucose level, and aminotransferase levels is suggested for children and adolescents with obesity (BMI ≥ 95th percentile). Additional assessment may be required in selected children with symptoms or signs of weight-related comorbidities.
Table 1.
List of medical and psychosocial problems of childhood obesity
Determinants of childhood obesity
Key determinants of childhood obesity in developed countries are not very different from that of the developing countries. However, faulty dietary habits and reduced physical activity remain significant problems.
Lack of physical activity
Overindulgence in indoor leisure activities and entertainment (e.g. television viewing, internet, and computer games) alone or in combination with factors like unsafe neighborhoods for walking and other outdoor activities, lack of open spaces and playgrounds in schools and communities along with increasing pressure on children to perform in academics and reduced emphasis on sports contribute to childhood obesity.
In developed countries, sedentary activity is usually in the form of “screen time,” e.g. television, video games, internet and computer, and other media. According to national surveys in the United States, children between 8 and 18 years spend an average of 7.5 hours daily viewing media and those under age 6 spent nearly two hours daily.[25] Television viewing is perhaps the best established environmental influence on the development of obesity during childhood. The association between obesity and use of other media is somewhat weaker.
Combining a clinical assessment of baseline activity levels with the barriers to increased activity will provide the clinician with a basis with which to begin behavior changes. Reducing sedentary activities is a particularly important target for intervention and should be incorporated into any clinical approaches toward obesity treatment and prevention.
Excess caloric intake
Because of unrestricted access to energy-dense fast foods in school cafeteria, school vending machines, and school neighborhood combined with low knowledge about dietary components in school children, there is often increased caloric intake per body weight per day. The practice of overfeeding low-birth-weight babies for catch-up growth, if continued, also contributes to obesity later.
High-income group with high socio-economic status
Daily allowance (pocket money) to purchase lunch, easy availability of domestic help to take care of household chores, commuting to school by bus or car instead of walking or bicycling, and aggressive advertising by transnational fast-food and cola companies are some of the practices which predispose children to obesity.
Sociocultural factors and urbanization
Overprotection and forced feeding by parents, false traditional beliefs about health and nutrition, and low knowledge about nutrition in parents and caregivers also contribute to obesity. Again, limited availability of open spaces and parks due to population expansion and illegal settlements along with abundance of fast-food outlets and eating points increase the chance of the child becoming obese.
Age and female gender
More obesity in prepubertal phase compared with postpubertal phase is somewhat attributed to self-consciousness among postpubertal children about weight gain and physical appearance. Also, females who are mostly engaged in household chores and less involved in playground activities develop obesity during early childhood, including those in some developed nations with strong sociocultural beliefs against sports and outdoor physical activity being pursued by girls.
Methodical approach of managing weight
A staged approach to pediatric weight management is provided by the American Academy of Pediatrics.[26] Multiple factors influence treatment at the initial stages, including age, BMI percentile, and previous weight management history. The recommendations emphasize on counseling on obesity prevention irrespective of their BMI percentile or previous treatment history.
Additional intervention to address overweight or obesity is divided into stages (Stage 1: Prevention, Stage 2: Structured weight management, Stage 3: Comprehensive multidisciplinary evaluation, and the Stage 4: Tertiary care intervention) representing escalating degrees of supervision, counseling, and intervention. The first two stages should involve the primary care provider.
Taking about the sensitive issue of weight
In developed world, in most cultures, there is some bias against individuals with obesity, which presumes that obesity is a character flaw. Despite progress in understanding the complex origins of obesity, which include genetic, epigenetic, cultural, and environmental factors, this bias remains widespread. The bias is also present within the medical community,[27] where it often causes providers to take a blaming approach toward obese persons. Such an approach often jeopardizes the therapeutic alliance,[28] and there is development of barriers to behavioral change like low self-esteem, self-criticism, and hopelessness. Due to this bias, many families with obesity are extremely sensitive about discussing the issue. Therefore, the blaming approach should be condemned, and the focus should be on the modifiable environmental risk factors. This approach will firmly establish a therapeutic alliance.
Prevention
All health care personnel unanimously agree that prevention is the key strategy for controlling the current epidemic of obesity.[29] Prevention may include primary prevention of overweight or obesity itself, secondary prevention or avoidance of weight regains following weight loss, and prevention of further weight increases in obese individuals unable to lose weight. Till recently, most exclusively focused approaches were based on behavioral changes of individuals, dietary modifications, and exercise; it is seen that these strategies have had little impact on the growing increase of the obesity epidemic. Therefore, the prevention efforts are now best focused on key behaviors associated with the development of obesity, although other factors including genetics undoubtedly also contribute to the risk for obesity.[26]
There is modest evidence to suggest that modification of the following factors may help to prevent the development of obesity.
Maternal factors
Maternal weight prior to conception and weight gain during pregnancy should be recorded. Breastfeeding may have a weak protective effect on the development of obesity but it is probably not a major determinant of obesity risk.
Psychosocial factors
Establishing a healthy feeding relationship early in life (avoiding overly restrictive and overly permissive feeding patterns) is definitely helpful. Encouraging a family to eat meals together usually helps the parents to monitor the type of food intake in children.
Dietary goals
Some of the dietary goals include limiting consumption of sugar-sweetened beverages, including juice, encouraging a diet with ample servings of vegetables and fruits, limiting eating at restaurants (particularly fast-food restaurants), and limiting portion size (which, for young children, is often less than a “serving size” as listed on a food label).
Activity goals
Encouraging moderate to vigorous physical activity for one or more hours daily[26] and limiting television and other screen time-no screen time for children under two years of age; less than two hours daily after age two.[30]
Priority age group for starting prevention
Children are the priority population for intervention strategies as weight loss during adulthood is difficult, and there are more potential interventions for children than for adults. Schools are a natural setting for influencing the food and physical activity environments of children. Other settings, such as preschool institutions and after-school care services, will have similar opportunities for action. Prevention may be achieved through a variety of interventions targeting built environment, physical activity, and diet.
Built Environment
It is a challenge to identify obesogenic environments and modify them so that healthier choices are made available, more accessible, and widely promoted to a large proportion of the community. The neighborhood is a main setting that can be used for intervention. It encompasses the walking network (footpath, sand trails, etc.), the cycling network (roads and cycle paths), public open spaces (parks), and recreation facilities (recreation centers, etc.). While the amount of public open space is limited within an existing built environment, protecting the loss of such spaces requires strong support and motivation within the community. The home environment is also very important in relation to shaping children's eating behaviors and physical activity patterns. Astonishingly, very little is known about specific home influences and as a setting, it is difficult to influence because of the total numbers and heterogeneity of homes and the limited options for access.[31] Of all aspects of behavior at home, however, television viewing has drawn the utmost attention among the researchers .[32,33,34]
Physical activity
Stone et al.[35] , after reviewing the impact of 14 school-based interventions on physical activity knowledge and behavior, observed that most of the outcome variables showed significant improvements after the intervention. An intervention program in the United States used a curriculum-based approach to influence eating patterns, reduce sedentary behaviors (with a strong emphasis on television viewing), and promote higher activity levels among children in Grades 6–8. After two years, when evaluated, it showed a reduction in obesity prevalence in girls. The reduction in television viewing (by only 30 min/day) was highly significant for both boys and girls. Increases in sports participation and/or physical education time definitely needs policy-based changes at both school and education sector levels.[36] Also, increases in active modes of transport to and from school (walking, cycling, and public transport) would require policy changes as well as support from parents and the community. In some communities, a variety of such programs have been implemented, e.g. road crossings, “walking bus,” and designated safe walking and cycling routes.[37].
Effects of dietary pattern and TV watching
Restricting television viewing appears to prevent obesity. Similarly, reduced eating in front of the television is also as important as increasing physical activity.[33] Fast foods are one of the most advertised products on television and children are often the targeted market. Reducing the huge volume of marketing of energy-dense foods and drinks and fast-food restaurants to young children, particularly through the powerful media of television, is a potential strategy that has been advocated. Television advertising to children less than 12 years of age has not been permitted in Sweden, although children's television programs from other countries through satellite television probably dilute the impact of the ban in Sweden. Norway, Denmark, Austria, Ireland, Australia, and Greece also have some restrictions on television advertising to young children.[37]
Nutrition sector
There is a marked influence of food prices on food-buying behavior and then on nutrient intake.[38] A tax, large enough to affect sales, levied on high-volume foods of low nutritional value, such as soft drinks, confectionery, and snack foods, may discourage their use. Such taxes are currently applied in some parts of the United States and Canada.[39] In addition, food labeling and nutrition “signposts” such as logos that indicate that a food meets specific nutrition standards might help consumers choose healthy foods. An example is the “Pick the Tick” symbol program run by the National Heart Foundations in Australia and New Zealand.[40] The “Pick the Tick” symbols made it easier for consumers to identify healthier food choices. Moreover, in addition to the nutrition criteria, the products serve as “defacto” standards of product formulation for the manufacturers.
Effectiveness of the prevention methods
It has been shown that focusing on reducing sedentary behavior and encouraging free play has been more effective than focusing on forced exercise or reducing food intake in preventing already obese children from gaining more weight.[41,42]
Recent efforts in preventing obesity include the initiative of using school report cards to make the parents aware of their children's weight problem. Health report cards are believed to aid prevention of obesity. In a study in the Boston area, parents who received health and fitness report cards were almost twice as likely to know or acknowledge that their child was actually overweight than those parents who did not receive a report card. They also were over twice as likely to plan weight control activities for their overweight children.
Specific recommendations
The following practices are recommended, which are based primarily on expert opinion and some are supported by clinical studies, usually with short-term outcomes.
Surveillance
Periodic monitoring of nutritional and obesity status of children and adults.
Regular measurement of BMI and plotting of results on a BMI chart to track changes over time
Assessment of all children for obesity-related risk factors to allow for early intervention. This includes recording the obesity status (BMI) of the biological parents and assessing key nutritional and physical activity habits
For children with obesity, weight-related comorbidities should be assessed through a focused review of systems, physical examination, and laboratory screening.
Maintain a nationwide database on secular trends in obesity and diabetes.
Education
or all children and their families, routine healthcare should include obesity-focused education
Nutrition and physical advice through audiovisual media and culturally conducive methods
Endorsement of healthy lifestyle by prominent people and local champions
For children who are overweight or obese, a series of clinical counseling interventions in the primary care setting is suggested
Educational materials are available from a variety of sources to facilitate the counseling. These materials have much in common and have not been directly compared; it is reasonable for providers to select materials with messaging that is best suited to their community
For patients who do not respond to a brief clinical intervention or for those with severe obesity, higher-intensity approaches are needed in tertiary care centers.
Community
Organization and participation in health walks and healthy food festivals
Information about nutrition to parents (particularly mothers)
Children-specific nutrition information and workshops for newly married women
Safe walk/bicycle routes to school
To establish a therapeutic relationship and enhance effectiveness, communication and interventions should be supportive rather than blaming, and family-centered rather than focused on the child alone
Long-term changes in behaviors that are related to obesity risk should be emphasized rather than diets and exercise prescriptions, which tend to set short-term goals.
Early infancy and perinatal period
Balanced nutrition to pregnant mothers
Encourage breastfeeding
Avoidance of catch-up obesity in children
Maintenance of correct growth velocity under guidance of physicians
Avoid excess nutrition to stunted children.
School-based interventions
High importance of physical activity
Healthy foods in cafeteria, ban on sweetened beverages and energy-dense junk food
Training of teachers regarding health education
Incorporation of more knowledge about nutrition and physical activity and nutrition-related diseases in school curriculum.
Home-based interventions
Key goals to address are the common diet-related problems encountered in children, set firm limits on television and other media early in the child's life, and establish habits of frequent physical activity.
TV/computer time to be restricted to maximum 2 hours/day
Mandatory 60 min of physical activity daily to be supervised by parents
Restriction on eating out and junk foods.
Health authority and legislation
Creation of national task force for obesity
Decrease in taxes and prices of fruits and vegetables
More playgrounds, parks and walking and bicycle tracks
Restriction on advertisement of commercial foods on television at prime time and during children's programs
Encourage trans-national food companies to manufacture healthy snacks
Ban on unfair nutrition claims for commercial products
Prohibition of promotional gifts with junk foods
Ban on monetary sponsorship of youth festivals by cola companies
Food labeling and quality monitoring
Food policy to include country-specific guidelines for healthy nutrition for adults and children.
CONCLUSION
Obesity is a chronic disorder with varied underlying etiology. Obesity in childhood has significant impact on both physical and psychological health, and over-consumption of calories and reduced physical activity are the two main factors involved in it. Therefore, the role of primary or secondary prevention is the mainstay plan for controlling this epidemic. Moreover, these strategies seem to be more effective in children than in adults. A good number of effective plans are thus implemented to target built environment, physical activity, and diet. These strategies can be initiated at home and in preschool institutions, schools, or after-school care services. However, further research needs to be conducted to examine the most effective strategies of intervention, prevention, and treatment of obesity. These strategies should be culture specific, ethnical, and consider the socio-economical aspects of the targeting population.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Nicklas TA, Baranowski T, Cullen KW, Berenson G. Eating patterns, dietary quality and obesity. J Am Coll Nutr. 2001;20:599–608. doi: 10.1080/07315724.2001.10719064. [DOI] [PubMed] [Google Scholar]
- 2.Parsons TJ, Power C, Logan S, Summerbell CD. Childhood predictors of adult obesity: A systematic review. Int J Obes. 1999;23:S1–107. [PubMed] [Google Scholar]
- 3.Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med. 1997;337:869–73. doi: 10.1056/NEJM199709253371301. [DOI] [PubMed] [Google Scholar]
- 4.Lobstein T, Bauer L, Uauy R. IASO International Obesity TaskForce. Obesity in children andyoung people: A crisis in public health. Obes Rev. 2004;5(Suppl 1):4–104. doi: 10.1111/j.1467-789X.2004.00133.x. [DOI] [PubMed] [Google Scholar]
- 5.Popkin BM, Gordon-Larsen P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int J Obes Relat Metab Disord. 2004;28(Suppl 3):S2–9. doi: 10.1038/sj.ijo.0802804. [DOI] [PubMed] [Google Scholar]
- 6.Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1:11–25. doi: 10.1080/17477160600586747. [DOI] [PubMed] [Google Scholar]
- 7.Rokholm B, Baker JL, Sorensen TI. The levelling off of the obesity epidemic since the year 1999- a review of evidence and perspectives. Obes Rev. 2010;11:835–46. doi: 10.1111/j.1467-789X.2010.00810.x. [DOI] [PubMed] [Google Scholar]
- 8.Nichols MS, Silva-Sanigorski Ad, Cleary JE, Goldfeld SR, Colahan A, Swinburn BA. Decreasing trends in overweight and obesity among an Australian population of preschool children. Int J Obes (Lond) 2011;35:916–24. doi: 10.1038/ijo.2011.64. [DOI] [PubMed] [Google Scholar]
- 9.Monteiro CA, Conde WL, Lu B, Popkin BM. Obesity andinequities in health in the developing world. Int J Obes Relat Metab Disord. 2004;28:1181–6. doi: 10.1038/sj.ijo.0802716. [DOI] [PubMed] [Google Scholar]
- 10.Oude Luttikhuis H, Baur L, Jansen H, Shrewsbury VA, O'Malley C, Stolk RP, et al. Interventions for treating obesity in children. Cochrane Database Syst Rev. 2009;1:CD001872. doi: 10.1002/14651858.CD001872.pub2. [DOI] [PubMed] [Google Scholar]
- 11.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452. [PubMed] [Google Scholar]
- 13.Freedman DS, Wang J, Ogden CL, Thornton JC, Mei Z, Pierson RN, et al. The prediction of body fatness by BMI and skinfold thicknesses among children and adolescents. Ann Hum Biol. 2007;34:183–94. doi: 10.1080/03014460601116860. [DOI] [PubMed] [Google Scholar]
- 14.Freedman DS, Wang J, Thornton JC, Mei Z, Sopher AB, Pierson RN, Jr, et al. Classification of body fatness by body mass index-for-age categories among children. Arch Pediatr Adolesc Med. 2009;163:805–11. doi: 10.1001/archpediatrics.2009.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Reilly JJ. Descriptive epidemiology and health consequences of childhood obesity. Best Pract Res Clin Endocrinol Metab. 2005;19:327. doi: 10.1016/j.beem.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 16.Krebs NF, Himes JH, Jacobson D, Nicklas TA, Guilday P, Styne D. Assessment of child and adolescent overweight and obesity. Pediatrics. 2007;120(Suppl 4):S193–228. doi: 10.1542/peds.2007-2329D. [DOI] [PubMed] [Google Scholar]
- 17.Lohman TG. Anthropometric assessment of fat-free body mass. New York: Wile-Liss; 1991. [Google Scholar]
- 18.Sarría A, Moreno LA, García-Llop LA, Fleta J, Morellón MP, Bueno M. Body mass index, triceps skinfold and waist circumference in screening for adiposity in male children and adolescents. Acta Paediatr. 2001;90:387–92. doi: 10.1080/080352501750126195. [DOI] [PubMed] [Google Scholar]
- 19.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, et al. CDC growth charts: United States. Adv Data. 2000;314:1–27. [PubMed] [Google Scholar]
- 20.WHO Multicentre Growth Reference Study Group 2006 WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: WHO; [Google Scholar]
- 21.World Health Organization WHO child growth standard 2006. [Last accessed on 2014 Jan 21]. Available from: http://www.who.int/childgrowth .
- 22.Butte NF, Garza C, de Onis M. Evaluation of the feasibility of international growth standards for school-aged children and adolescents. J Nutr. 2007;137:153–7. doi: 10.1093/jn/137.1.153. [DOI] [PubMed] [Google Scholar]
- 23.Chadha DS, Gupta N, Goel K, Pandey RM, Kondal D, Ganjoo RK, et al. Impact of obesity on the left ventricular functions and morphology of healthy Asian Indians. Metab Syndr Relat Disord. 2009;7:151–8. doi: 10.1089/met.2008.0054. [DOI] [PubMed] [Google Scholar]
- 24.Goel K, Misra A, Vikram NK, Poddar P, Gupta N. Subcutaneous abdominal adipose tissue is associated with the metabolic syndrome in Asian Indians independent of intra-abdominal and total body fat. Heart. 2010;96:579–83. doi: 10.1136/hrt.2009.183236. [DOI] [PubMed] [Google Scholar]
- 25.Generation M2. Media in the lives of 8- to 18-year olds. The Kaiser Family Foundation. [Last accessed on 2014 Jan 22]. Available from: http://www.kff.org/entmedia/mh012010pkg.cfm .
- 26.Spear BA, Barlow SE, Ervin C, Ludwig DS, Saelens BE, Schetzina KE, et al. Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics. 2007;120(Suppl 4):S254–88. doi: 10.1542/peds.2007-2329F. [DOI] [PubMed] [Google Scholar]
- 27.Majdan JF. Memoirs of an obese physician. Ann Intern Med. 2010;153:686–7. doi: 10.7326/0003-4819-153-10-201011160-00017. [DOI] [PubMed] [Google Scholar]
- 28.Puhl RM, Heuer CA. Obesity stigma: Important considerations for public health. Am J Public Health. 2010;100:1019–28. doi: 10.2105/AJPH.2009.159491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Muller MJ, Mast M, Asbeck I, Langnase K, Grund A. Prevention of obesity-is it possible? Obes Rev. 2001;2:15–28. doi: 10.1046/j.1467-789x.2001.00012.x. [DOI] [PubMed] [Google Scholar]
- 30.Davis MM, Gance-Cleveland B, Hassink S, Johnson R, Paradis G, Resnicow K. Recommendations for prevention of childhood obesity. Pediatrics. 2007;120(Suppl 4):S229–53. doi: 10.1542/peds.2007-2329E. [DOI] [PubMed] [Google Scholar]
- 31.Campbell K, Crawford D, Jackson M, Cashel K, Worsley A, Gibbons K, et al. Family food environments of 5-6-year-old-children: Does socioeconomic status make a difference? Asia Pac J Clin Nutr. 2002;11(Suppl 3):S553–61. doi: 10.1046/j.0964-7058.2002.00346.x. [DOI] [PubMed] [Google Scholar]
- 32.Gortmaker SL, Peterson K, Wiecha J, Sobol AM, Dixit S, Fox MK, et al. Reducing obesity via a school-based interdisciplinary intervention among youth: Planet Health. Arch Pediatr Adolesc Med. 1999;153:409–18. doi: 10.1001/archpedi.153.4.409. [DOI] [PubMed] [Google Scholar]
- 33.Robinson TN. Reducing children's television viewing to prevent obesity: A randomized controlled trial. JAMA. 1999;282:1561–7. doi: 10.1001/jama.282.16.1561. [DOI] [PubMed] [Google Scholar]
- 34.Dietz WH, Gortmaker SL. Preventing obesity in children and adolescents. Annu Rev Public Health. 2001;22:337–53. doi: 10.1146/annurev.publhealth.22.1.337. [DOI] [PubMed] [Google Scholar]
- 35.Stone EJ, McKenzie TL, Welk GJ, Booth ML. Effects of physical activity interventions in youth. Review and synthesis. Am J Prev Med. 1998;15:298–315. doi: 10.1016/s0749-3797(98)00082-8. [DOI] [PubMed] [Google Scholar]
- 36.Dwyer T, Coonan WE, Leitch DR, Hetzel BS, Baghurst RA. An investigation of the effects of daily physical activity on the health of primary school students in South Australia. Int J Epidemiol. 1983;12:308–13. doi: 10.1093/ije/12.3.308. [DOI] [PubMed] [Google Scholar]
- 37.Swinburn B. Egger G: Preventive strategies against weight gain and obesity. Obes Rev. 2002;3:289–301. doi: 10.1046/j.1467-789x.2002.00082.x. [DOI] [PubMed] [Google Scholar]
- 38.Guo X, Popkin BM, Mroz TA, Zhai F. Food price policy can favorably alter macronutrient intake in China. J Nutr. 1999;129:994–1001. doi: 10.1093/jn/129.5.994. [DOI] [PubMed] [Google Scholar]
- 39.Jacobson MF, Brownell KD. Small taxes on soft drinks and snack foods to promote health. Am J Public Health. 2000;90:854–7. doi: 10.2105/ajph.90.6.854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Young L, Swinburn B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Promot Int. 2002;17:13–9. doi: 10.1093/heapro/17.1.13. [DOI] [PubMed] [Google Scholar]
- 41.Caterson ID, Gill TP. Obesity: Epidemiology and possible prevention. Best Pract Res Clin Endocrinol Metab. 2002;16:595–610. doi: 10.1053/beem.2002.0228. [DOI] [PubMed] [Google Scholar]
- 42.Chomitz VR, Collins J, Kim J, Kramer E, McGowan R. Promotinghealthy weight among elementary school children via a health report card approach. Arch Pediatr Adolesc Med. 2003;157:765–72. doi: 10.1001/archpedi.157.8.765. [DOI] [PubMed] [Google Scholar]