

Abstract
A fibrous or flabby ridge is a superficial area of mobile soft tissue affecting the maxillary or mandibular alveolar ridges. It can develop when hyperplastic soft tissue replaces the alveolar bone and is a common finding particularly in the upper anterior region of long term denture wearers. Masticatory forces can displace this mobile denture-bearing tissue, leading to altered denture positioning and loss of peripheral seal. Forces exerted during the act of impression making can result in distortion of the mobile tissue. Unless managed appropriately by special impression techniques, such ‘flabby ridges’ adversely affect the support, retention and stability of complete dentures. This paper presents three case reports for prosthodontic rehabilitation of patient with flabby ridges with three different impression techniques.
Keywords: Flabby tissue, impressions, irreversible hydrocolloid
INTRODUCTION
A fibrous or flabby ridge is a superficial area of mobile soft tissue affecting maxillary or mandibular alveolar ridges. It develops when hyperplastic soft tissue replaces the alveolar bone and is a common finding particularly in the upper anterior region of long term denture wearers. The reported prevalence has varied, but has been demonstrated in upto 24% of edentulous maxillae and 5% edentulous mandibles. Masticatory forces can displace this mobile denture-bearing tissue leading to loss of peripheral seal. Forces exerted during impression making can result in distortion of the mobile tissue.[1] Unless managed appropriately by special impression techniques, such ‘flabby ridges’ adversely affect support, retention and stability of complete dentures. Many impression techniques have been proposed to help overcome this difficulty.[2]
This article presents case reports for prosthodontic rehabilitation of patient with flabby ridges with three different impression techniques.
CASE REPORT
Case 1
A 60 year old female patient reported to the Department of Prosthodontics and Crown and Bridge with complaint of loose dentures. On examination, flabby tissue in the maxillary anterior region extending from canine to canine region was found. Tissue blanching was also noticed on pressure application [Figure 1].
Figure 1.

Flabby tissue in the maxillary anterior region
Fabrication of new complete dentures was planned for the patient with recording of flabby tissue in undisplaced condition using Hobkirk technique.[3] The maxillary preliminary impression was made using irreversible hydrocolloid (Tulip Alginate Impression Material, Cavex Holland BV, Holland) in perforated edentulous tray and the primary cast was poured [Figures 2a and b]. Special tray was fabricated using double spacer over the flabby tissue area and in the region of mid palatine raphe. After checking the proper tray extensions, border molding was done in conventional manner using green stick impression compound (DPI Pinnacle Tracing Sticks) [Figures 2c and d].
Figure 2.
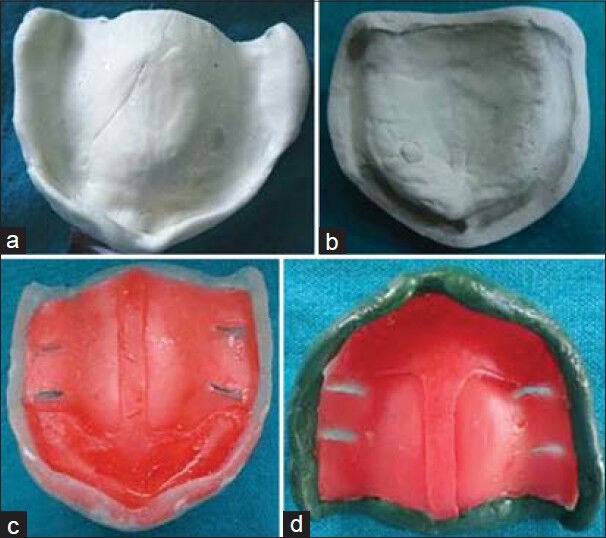
(a) Preliminary impression, (b) Primary cast, (c) Special tray, (d) Border molding
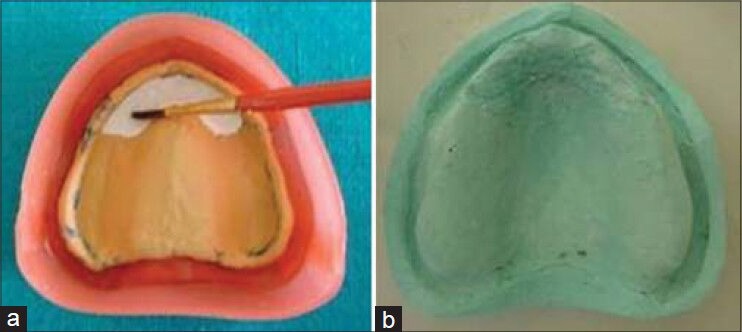
Spacer wax was removed and impression was made with medium body elastomeric impression material (Elite Glass medium body, Zhermack, Germany). The tray was then removed from the mouth and impression material was removed in the region of flabby tissue using a scalpel. Relief holes were made and tray was loaded in this region with light body elastomeric impression material (Elite HD+ light body, Zhermack, Germany) to record flabby tissue. Beading and boxing of the final impression was done using plaster pumice method and master cast was poured [Figures 3a–c]. The denture was fabricated and it had good retention and stability with proper recording of flabby tissue [Figures 3d, 4a and b].
Figure 3.
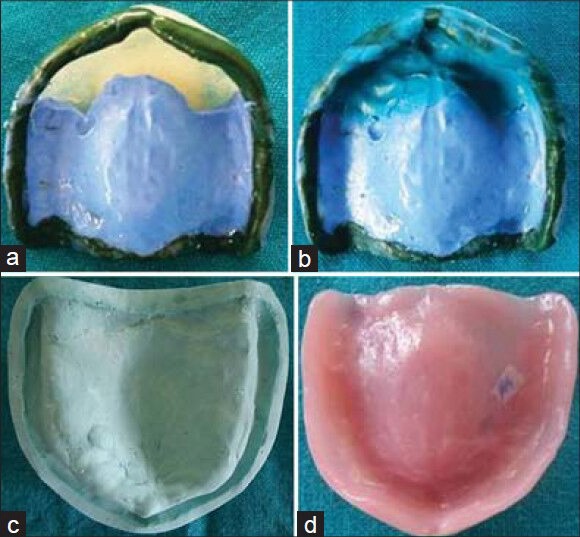
(a and b) Secondary impression,(c) Master cast,(d) Maxillary denture
Figure 4.

(a) Preoperative, (b) Postoperative
Case 2
A female patient aged 56 years reported to the Department of Prosthodontics and Crown and Bridge with complaint of ill fitting dentures. On examination, an area of flabby tissue in the maxillary anterior region was found [Figure 5].
Figure 5.

Flabby tissue in the maxillary anterior region
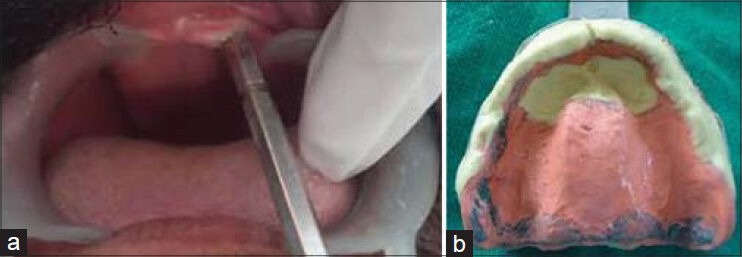
Zafarullah Khan technique[4] for impression making was planned for this patient. The maxillary preliminary impression was made using irreversible hydrocolloid (Tulip Alginate Impression Material, Cavex Holland BV, Holland) in perforated edentulous tray and primary cast was poured. Spacer was adapted over the primary cast except in the region of flabby tissue. Special tray was fabricated providing a window in the region of flabby tissue. Border molding was done using green stick compound [Figure 6a–d]. Spacer wax was removed and impression was made with zinc oxide eugenol impression material. With the zinc oxide eugenol impression (DPI Impression Paste) in the mouth, flabby tissue was painted with impression plaster. Impression plaster was allowed to set and tray was removed from the mouth [Figures 7a and b]. Master cast was poured after applying soap solution as separator over impression plaster [Figures 8a and b]. The denture was fabricated in which flabby tissue was properly recorded and given adequate relief [Figures 9a and b].
Figure 6.
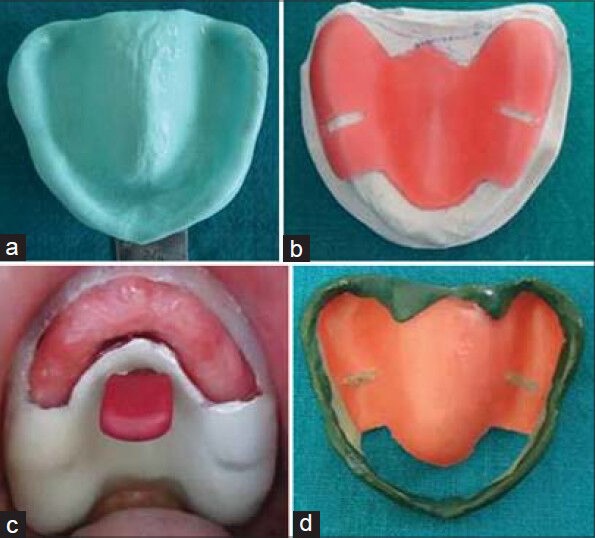
(a) Preliminary impression, (b and c) Special tray with window, (d) Border molding
Figure 7.
(a) Painted impression plaster (b) Secondary impression
Figure 8.
(a) Beading boxing (b) Master cast
Figure 9.

(a) Preoperative (b) Postoperative
Case 3
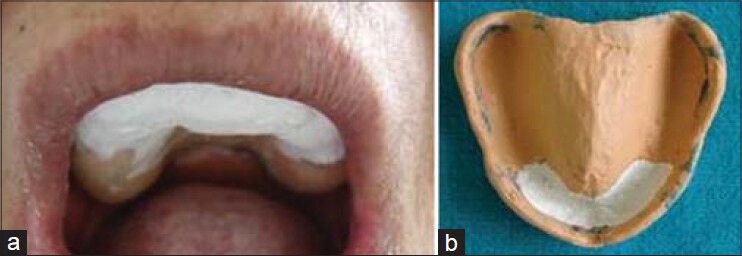
A 65 year old male patient reported to the Department of Prosthodontics and Crown and Bridge with history of wearing maxillary complete denture opposing mandibular removable partial denture for 2 years. He got his mandibular anteriors extracted 6 months back. There was flabby tissue in the maxillary anterior region. Window technique was used for this patient also. Instead of impression plaster, over impression of the flabby tissues was made with irreversible hydrocolloid (Tulip Alginate Impression Material, Cavex Holland BV, Holland) [Figures 10a and b].
Figure 10.
(a) Flabby tissue (b) Secondary impression
DISCUSSION
In 1972, Kelly and his colleagues first described ‘combination syndrome’ caused by the presence of opposing natural teeth to an edentulous area. His observations included alveolar bone resorption in the anterior maxilla, enlargement of the tuberosities and bone resorption underneath the mandibular denture bases.[5] Liddlelow[2] in 1964 described a technique whereby two separate impression materials were used in a custom tray (using ‘plaster of Paris’ over the flabby tissues and zinc oxide eugenol over the normal tissues). In 1964, Osborne[2] described a technique where two separate impression trays and materials were used to separately record the ‘flabby’ and ‘normal’ tissues and then related intra-orally. Watt and McGregor[2] in 1986 described a technique where impression compound was applied to a modified custom tray and a wash impression with zinc-oxide and eugenol is made.
Impression making plays critical role in complete denture fabrication. A particular problem is encountered if a flabby ridge is present within an otherwise ‘normal’ denture bearing area. An impression technique is required which will compress the non flabby tissues to obtain optimal support and at the same time, will not displace the flabby tissues.
CONCLUSION
Managing a patient with flabby maxillary ridge can be a challenging problem. Standard mucocompressive impression techniques are likely to result in an unretentive and unstable denture as the denture will be constructed on a model of the flabby tissue in a distorted state. Mucostatic techniques may not make the best use of the available tissue support and movement of the denture base relative to the support tissues may be a problem. The use of selective pressure or minimally displacive impression techniques should help to overcome some of these limitations. With modified impression techniques, these ridges can be managed effectively without any additional clinical visits as compared to patients with normal edentulous ridges.[6]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Crawford RW, Walmsley AD. A review of prosthodontic management of fibrous ridges. Br Dent J. 2005;199:715–9. doi: 10.1038/sj.bdj.4812968. [DOI] [PubMed] [Google Scholar]
- 2.Lynch CD, Allen PF. Management of the flabby ridge: Using contemporary materials to solve an old problem. Br Dent J. 2006;200:258–61. doi: 10.1038/sj.bdj.4813306. [DOI] [PubMed] [Google Scholar]
- 3.Hobkirk JA. Bristol: Wright; 1986. Complete Denturesda Dental Practitioner Hand book; pp. 44–5. [Google Scholar]
- 4.Khan Z, Jaggers JH, Shay JS. Impression of unsupported movable tissues. J Am Dent Assoc. 1981;103:590–2. doi: 10.14219/jada.archive.1981.0292. [DOI] [PubMed] [Google Scholar]
- 5.Kelly E. Changes caused by a mandibular removable partial denture opposing a maxillary complete denture. J Prosthet Dent. 1972;27:140–50. doi: 10.1016/0022-3913(72)90190-4. [DOI] [PubMed] [Google Scholar]
- 6.Allen F. Management of the flabby ridge in complete denture construction. Dent Update. 2005;32:524–8. doi: 10.12968/denu.2005.32.9.524. [DOI] [PubMed] [Google Scholar]