

Abstract
Introduction:
Health warnings on tobacco packages are an effective strategy for informing the public about the harms associated with tobacco use. Most studies investigating the effectiveness of pictorial health warnings (PHWs) on cigarette packages are from high-income countries. This study evaluated the impact of PHWs on smokers’ perceptions and behavior in Mauritius, the first country in the World Health Organization African region to implement PHWs.
Methods:
Data were drawn from 3 waves of a nationally representative cohort of adult smokers from the International Tobacco Control (ITC) Mauritius Survey (n = 668). Wave 1 was conducted in 2009, 6 months prior to the implementation of PHWs. Waves 2 and 3 were conducted 10–12 months and 20–21 months, respectively, postimplementation. Six established indicators of warning effectiveness were used to evaluate the effect of PHWs on smokers’ perceptions and behavior.
Results:
All indicators of warning effectiveness (salience, cognitive, and behavioral reactions) and the Label Impact Index, a weighted combination of 4 indicators, increased significantly between Waves 1 and 2. However, between Waves 2 and 3, there was a significant decline in the proportion of smokers who reported “avoiding looking” at labels.
Conclusions:
This study found that implementation of PHWs in Mauritius significantly enhanced the effectiveness of warnings, illustrating their value for other countries, particularly in Africa, at an early stage in tobacco control. The study also demonstrates the importance of revising PHWs to counteract wearout. The introduction of PHWs in Mauritius clearly demonstrates the benefits of employing an evidence-based approach to strengthen tobacco control policies.
INTRODUCTION
Health warnings on tobacco packaging constitute an important intervention to inform the public about the harms associated with tobacco use (Hammond, 2011). With high reach at the population level and high frequency of exposure at the individual level, warnings also constitute an extremely cost-effective tobacco control strategy. In fact, the pack-a-day smoker is potentially exposed to warnings more than 7,000 times in one year (Hammond et al., 2007; Yong et al., 2013). Moreover, health warnings may be one of the few sources of health information on the dangers of smoking in many low- and middle-income countries (LMICs), where 80% of tobacco-related deaths occur (World Health Organization [WHO], 2008).
Article 11 of the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC) calls for the implementation of health warnings that cover at least 30% of the principal display areas (WHO, 2003). The Article 11 Guidelines provide more detailed recommendations such as calling for FCTC Parties to implement warnings that are periodically rotated; large, clear, visible, and legible; and are in the form of pictorials instead of text-only (WHO, 2008). To date, more than 60 countries have either implemented warnings that meet this standard or passed legislation calling for such warnings to be implemented (Canadian Cancer Society, 2012).
Studies have consistently shown that pictorial health warnings (PHWs) are more effective than text-only warnings in increasing key indicators of warning effectiveness, including their salience (noticing and reading warnings closely), cognitive measures (thinking about the health risks and motivation to quit smoking), and behavioral indicators (avoiding warnings and reports of forgoing a cigarette because of the warnings) (Borland et al., 2009a; Fong, Hammond, & Hitchman, 2009; Hammond, 2011; Hammond et al., 2007; WHO, 2008). In a study investigating PHWs in Canada, United States, United Kingdom, and Australia, Hammond et al. (2007) found that the effectiveness of PHWs in Canada was significantly greater than those in the other three countries, which at the time had not implemented PHWs. Additional studies (e.g., Hammond, Fong, McDonald, Cameron, & Brown, 2003; Hammond, Fong, McNeill, Borland, & Cummings, 2006) showed that PHWs on cigarette packs were associated with stronger beliefs that smoking is harmful and increased motivation to quit smoking. For example, PHWs with increased salience that evoke emotional responses (cognitive and/or behavioral) among smokers are associated with future cessation-related behavior (Borland et al., 2009b; Yong et al., 2013). Furthermore, evidence from population-based surveys found that smokers who avoided warnings were just as likely as others to attempt to quit smoking (Borland et al., 2009b).
The vast majority of studies investigating the effectiveness of PHWs on cigarette packages have been based on well-educated Western populations from high-income countries (Yong et al., 2013). To date, only a very limited number of studies investigating the effectiveness of PHWs have been conducted in non-Western or LMICs. A study investigating responses to PHWs among Malaysian smokers revealed that, relative to text-only warnings, PHWs resulted in increased awareness of smoking-related health risks and an increased motivation to quit smoking (Fathelrahman et al., 2010). Similar results were found in a study conducted among Chinese smokers, who rated PHWs as more effective in motivating smoking cessation compared to text-only warnings (Fong et al., 2010). A recent study by Yong et al. (2013) also found a significant increase in reported awareness of cognitive and behavioral responses among smokers after the introduction of PHWs in Thailand. These results were compared to responses to text-only warnings in Malaysia over the same time period, where no significant changes in warning effectiveness were found. Finally, a study comparing the impact of Mexican text-only warnings with Canadian PHWs found that warnings in the form of prominent graphic imagery were more effective in improving smoking-related knowledge and in motivating cessation (Thrasher, Hammond, Fong, & Arillo-Santillán, 2007). These results were consistent with a later study conducted among smokers in Brazil, Uruguay, and Mexico, which found that compared to text-only warnings, PHWs depicting smoking-related bodily harm or human suffering were most effective (Thrasher et al., 2010).
Although the limited published evidence has indicated that the effects of PHWs are similar in LMICs, there have been no studies of PHWs in the African region, and it is unclear if previous evidence is generalizable due to region-specific differences (Blecher & Ross, 2013). For example, many African countries have weaker systems of tobacco control and law enforcement, as well as low awareness of the harms of using tobacco (Steptoe et al., 2002). The few studies that investigated tobacco use in Africa show that awareness of the harms of using tobacco in Sub-Saharan Africa is considerably lower than in LMICs in other regions of the world (Pampel, 2008; Steptoe et al., 2002). In fact, most male respondents from a qualitative study conducted in a rural community in Uganda believed that cigarettes were safe to use (van Gemert et al., 2013).
Due to these low levels of awareness, efforts to inform the public of the harms of tobacco use in the African region rank highly in the overall strategy of tobacco control. Unfortunately, existing literature shows that warnings have been underutilized among African nations. Tumwine (2011) showed that more than half (32 out of 54) of the African countries have only small text-only warnings (covering less than 30% of the front and back of package) or none at all. This is particularly problematic, as Africa is the region that presents the greatest threat in terms of future growth in smoking because current smoking rates are so low. With the growing number of smokers in Africa due to the economic and population growth seen over the past decade, it is important to determine which tobacco control policies hold greatest promise in reducing smoking rates. If the increase in smoking rates in Africa continue, it has been projected that by 2100, 26% of the world’s smokers (from the current 6%) representing 572 million smokers will live in Africa. Implementation of proven tobacco control policies, including PHWs and significant increases in price/tax of tobacco products, could reduce this number to almost half (Blecher & Ross, 2013).
In October 2009, Mauritius became the first country in WHO’s African region to implement PHWs, replacing a text-only warning that read, “GOVERNMENT WARNING: Smoking causes cancer, heart disease and bronchitis” with a set of eight rotating PHWs covering 60% of the front (in French) and 70% of the back (in English) of cigarette packages. Cigarette packages were also required to have a text warning covering 65% of the side of the pack in either French or English. Mauritius is a leading nation in regards to tobacco control initiatives within the African region, as smoking has been banned in indoor public places, public transport, as well as in health, sport, and educational facilities. Advertising, promotion, and sponsorship of tobacco products are also prohibited. To raise awareness on the smoke-free law and the dangers of secondhand smoke, the government organized media campaigns in 2009 and launched the “Sponge” campaign in 2011 (ITC Project, 2012a).
This article reports the results of a longitudinal evaluation study of the impact of the introduction of PHWs in Mauritius among a nationally representative cohort of adult smokers at three points in time: six months before the implementation (Wave 1), 10–12 months after the implementation (Wave 2), and 20–21 months after the implementation (Wave 3). The inclusion of two postimplementation timepoints allowed us to evaluate the impact of PHWs on Mauritian smokers’ perceptions and behavior by investigating: (a) whether the indicators of warning effectiveness increased after introduction of PHWs (between Wave 1 and Wave 2) and (b) whether there was evidence of wearout—leveling off or reductions in warning effectiveness—between Wave 2 and Wave 3. Studies have shown that the impact and effectiveness of health messages diminish the longer they remain in circulation (Elliott & Shanahan Research, 2009; Hammond et al., 2007; Hitchman et al., 2013). Accordingly, the analyses also tested for the presence of wearout between Wave 2 and Wave 3.
METHODS
Study Design
The International Tobacco Control (ITC) Mauritius Survey is a nationally representative longitudinal survey of adult smokers and nonsmokers in Mauritius. The ITC Mauritius Survey is part of the larger ITC Project (Fong et al., 2006), which has conducted parallel longitudinal cohort surveys in 22 countries to evaluate FCTC policies. Wave 1 of the ITC Mauritius Survey was conducted six months prior to the implementation of PHWs (April 20–May 24, 2009). Wave 2 and Wave 3 were conducted 10–12 months (August 30–October 2, 2010) and 20–21 months (June 20–July 11, 2011), respectively, postimplementation.
Participants and Survey Procedures
The participants in this study were smokers who completed the ITC Mauritius Survey at any of the three survey waves. Smokers were defined as those aged 18 years and older who had smoked more than 100 cigarettes in their lifetime and at least once in the past 30 days. A stratified multistage survey design was used to randomly select respondents from households within strata, defined by the nine geographic districts of Mauritius to ensure similar urban–rural representation (43% urban and 57% rural). Data were collected using face-to-face interviews in the Mauritian Creole language by interviewers hired and trained by the Mauritius Institute of Health, using extensive training materials provided by the ITC Project. The average time to complete the survey was 60min.
Over the three waves, 668 smokers were recruited, the majority in Wave 1 (n = 598). Survey response rates in Wave 1 were high: the household response rate was 89.8% and the individual response rate was 80.7% (ITC Project, 2012a). Respondents lost to attrition were replaced in subsequent waves, but retention rates were also very high: of those participating in Wave 1, 95% (n = 555) were surveyed again in Wave 2 while 89% (n = 534) participated in all waves. In Waves 2 and 3, 46 and 24 new smokers, respectively, were added to the cohort using the same sampling protocol employed in Wave 1.
Research ethics approval was obtained from the University of Waterloo Human Research Ethics Committee and from the National Ethics Committee of Mauritius.
Measures
Demographic Characteristics
Demographic measures included gender (male and female), age group (18–24, 25–39, 40–54, and 55+), income (low: MUR <15,000; moderate: MUR 15,000–24,999; high: MUR ≥25,000, not stated), and education (no education, primary school/Form 1–Form 4, school certificate/higher school certificate/vocational, university level, or higher).
Smoking Behavior
Smoking behaviors were measured using smoking status (daily vs. nondaily smoker) and number of cigarettes smoked per day (0–10, 11–20, 21–30, 31+).
Intentions to Quit Smoking
Intentions to quit smoking were measured with a question (planning to quit within the next six months, planning to quit, but not within the next six months, not planning to quit).
Health Warning Label Effectiveness
At each wave, warning label effectiveness was measured using three groups of indicators: salience, cognitive reactions, and behavioral reactions. Each of these indicators was analyzed as a dichotomous measure to estimate how frequently smokers noticed, read, and had specific cognitive and behavioral reactions to the PHW labels. These measures have been used to evaluate the effectiveness of health warnings in every ITC study across many countries (ITC Project, 2012b) and are listed in the section on evaluating health warnings in the 2008 Cancer Prevention Handbook of the International Agency of Research on Cancer on methods for evaluating the effectiveness of tobacco control policies (International Agency for Research on Cancer [IARC], 2008).
Salience was measured by two questions: (a) NOTICING: “In the last month, how often, if at all, have you noticed warnings on cigarette packages (dichotomized as: often/very often vs. never or once in a while)?” (b) READING: “In the last month, how often, if at all, have you read or looked closely at the warning labels on cigarette packages (dichotomized as: often vs. never or once in a while)?”
Cognitive reactions were measured by two questions: (a) THOUGHTS: “To what extent, if at all, do the warning labels make you think about the health risks of smoking (dichotomized as: a lot vs. not at all or a little)?” (b) QUITTING LIKELIHOOD: “To what extent, if at all, do the warning labels on cigarette packs make you more likely to quit smoking (dichotomized as: a lot vs. a little or not at all)?”
Behavioral reactions were measured by two questions: (a) FORGOING: “In the last month, have the warning labels stopped you from having a cigarette when you were about to smoke one? Would you say never, once in a while, many times?” Responses were dichotomized as: once in a while/many times versus never. (b) AVOIDING: “In the last month have you made any effort to avoid looking or thinking about the warning labels, such as covering them up, keeping them out of sight, using a cigarette case, avoiding certain warnings, or any other means (yes vs. no)?”
Labels Impact Index
Adapted from previous research (Borland et al., 2009b), the Label Impact Index (LII) is a composite measure that combines four of the six outcomes indicators (NOTICING, THOUGHTS, QUITTING, and FORGOING). The index was created by standardizing the original measures and then weighting and summing the standardized scores as follows: LII = (NOTICING*1) + (THOUGHTS*2) + (QUITTING*2) + (FORGOING*3). Higher scores indicate greater impact.
Analyses
The proportion of smokers responding positively to each of the outcome measures was estimated in SAS (version 9.2) for each survey wave using statistical methods appropriate for the analysis of complex survey data. Estimates were weighted so that they were representative of the population of smokers in Mauritius. Generalized estimating equation (GEE) regression models were then used to test changes in warning label measures over time following the introduction of PHWs between Waves 1 and 2. GEE models account for within-subject correlation arising when outcomes are measured on the same respondent more than once (Liang & Zeger, 1986). It was expected that significant increases in each of the warning effectiveness measures would be observed between Waves 1 and 2. Additionally, wearout of these warnings was expected between Waves 2 and 3. Logistic regression models were estimated using GEE for binary outcomes, and linear GEE regression models were used to test the change in the LII over time. An exchangeable working correlation matrix was used to account for within-subject correlations across the survey waves. Regression models controlled for time-varying (cigarettes smoked per day, quit intentions) and time invariant (sex, age group, income, education) covariates to ensure that any changes in the effectiveness measures were not attributable to confounding effects from these covariates. Smokers who did not state their income were excluded from the GEE analysis because they were very few (n = 11). GEE models were estimated using SUDAAN version 10.0.1 to account for nonresponse and the complex survey design. Although the analysis was conducted using both unweighted and weighted data, only weighted results are presented because there were no differences between the two.
RESULTS
Sample Characteristics
Table 1 presents the unweighted sample characteristics for smokers at each of the three waves of the ITC Mauritius Survey. The majority of respondents were male (94.5%). The average age was 44.2 years (SD = 14.2). The majority of respondents were from the lowest education category (71.0%) and from the lowest income group (68.9%). Consistent with high-income countries and many other LMICs, the vast majority of smokers were daily smokers (91.2%).
Table 1.
Unweighted Sample Characteristics
| Characteristic | Frequency | % | |
|---|---|---|---|
| Sex | Male | 630 | 94.3 |
| Female | 38 | 5.7 | |
| Age (years) | 18–24 | 54 | 8.1 |
| 25–39 | 202 | 30.2 | |
| 40–54 | 253 | 37.9 | |
| 55+ | 159 | 23.8 | |
| M (SD) | 44.25 (14.23) | ||
| Income | < MUR 15,000 | 460 | 68.9 |
| MUR 15,000–24,999 | 132 | 19.8 | |
| ≥ MUR 25,000 | 65 | 9.7 | |
| Not stated | 11 | 1.6 | |
| Education | Up to Form 4 | 474 | 71.0 |
| SC/HSC completed | 157 | 23.5 | |
| Some/completed university | 37 | 5.5 | |
| Smoking status | Nondaily smoker | 59 | 8.8 |
| Daily smoker | 609 | 91.2 | |
| Smoking frequency | <10 cigarettes/day | 527 | 78.9 |
| 11–20 cigarettes/day | 115 | 17.2 | |
| 21–30 cigarettes/day | 18 | 2.7 | |
| 31+ cigarettes/day | 8 | 1.2 | |
| M (SD) | 9.16 (6.99) | ||
| Cohort: Wave entered | 1 | 598 | 89.5 |
| 2 | 46 | 6.9 | |
| 3 | 24 | 3.6 | |
| Retention: Cohort 1 | |||
| Wave 1 to Wave 2 | Lost | 43 | 7.2 |
| Retained | 555 | 92.8 | |
| Wave 2 to Wave 3 | Lost | 21 | 3.8 |
| Retained | 534 | 96.2 | |
| Retention: Cohort 2 | |||
| Wave 2 to Wave 3 | Lost | 2 | 4.3 |
| Retained | 44 | 95.7 | |
The retention rate was very high: 92.8% at Wave 2 and 96.2% at Wave 3. Therefore, possible biases due to attrition are minimal.
Impact of Pictorial Warnings—Wave 1 Versus Wave 2
The changes in the indicators of warning effectiveness across the waves are shown in Figure 1. The GEE analyses revealed that all indicators increased significantly between Waves 1 and 2. After the introduction of PHWs, Mauritian smokers had almost four times greater odds of reporting noticing warnings (p < .001, odds ratio [OR] = 3.60, 95% confidence interval [CI] = 2.38–5.44), increasing from 58.0% to 83.4%, and almost three times greater odds of reporting reading warnings closely (p < .001, OR = 2.64, 95% CI = 1.96–3.55), increasing from 29.8% to 51.8% after the introduction of PHWs.
Figure 1.
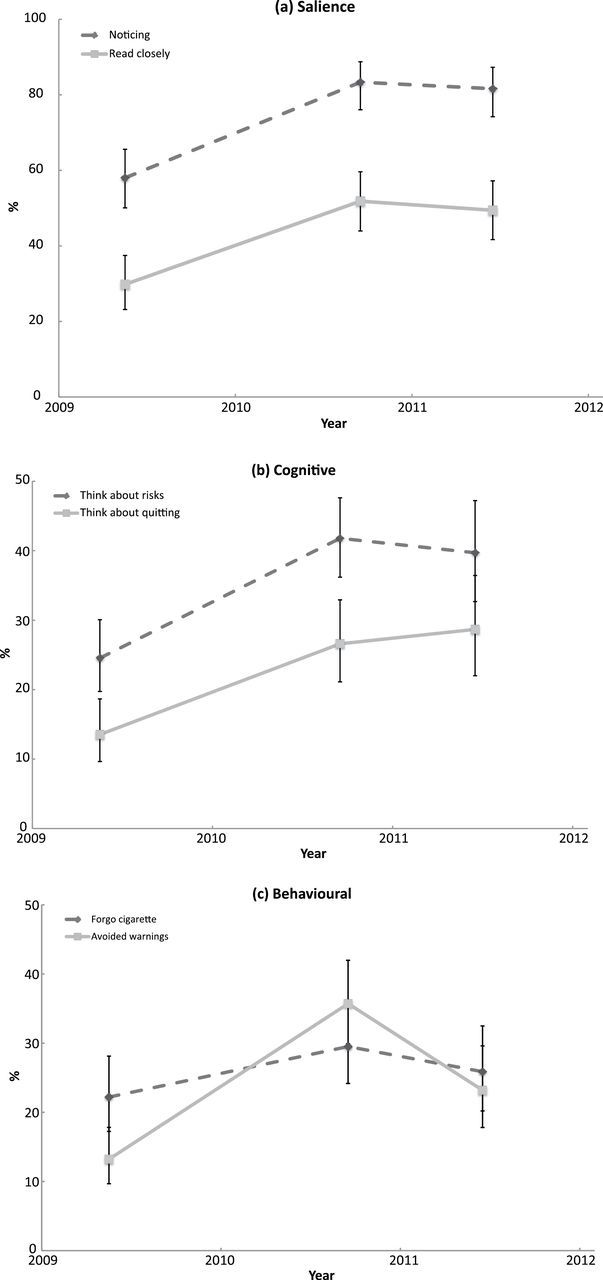
Generalized estimating equation analysis showing changes of health warning effectiveness measures over time.
Cognitive responses significantly increased from Wave 1 to Wave 2, with smokers having more than double the odds of reporting thinking about smoking-related health risks (p < .001, OR = 2.47, 95% CI = 1.87–3.26) and reporting considering quitting (p < .001, OR = 2.69, 95% CI = 1.75–4.15) because of the warning. From Wave 1 to Wave 2, smokers who reported thinking about smoking-related health risks increased from 24.5% to 41.8% and smokers who reported considering quitting increased from 13.5% to 26.6%.
Behavioral responses increased from Wave 1 to Wave 2, with smokers having significantly greater odds of reporting avoiding looking at the warnings (p < .001, OR = 3.85, 95% CI = 2.39–6.19). The percentage of smokers reporting avoiding labels increased from 13.2% in Wave 1 to 35.7% in Wave 2. Additionally, from Wave 1 to Wave 2, smokers had 66% greater odds of reporting forgoing a cigarette “at least once in a while” because of the warnings. Although marginally significant (p = .051, OR = 1.66, 95% CI = 1.10–2.52), the percentage of smokers reporting forgoing a cigarette “at least once in a while,” increased from 22.2% (Wave 1) to 29.5% (Wave 2).
Evidence of Wearout—Wave 2 Versus Wave 3
GEE analyses showed that there was a significant decline in the proportion of smokers reporting “avoiding looking” at the labels between Waves 2 and 3 (p = .004, OR = 0.52, 95% CI = 0.36–0.76) from 36% to 23% (Figure 1). Although not statistically significant, the remaining warning label effectiveness indicators (except the “considering quitting” indicator) also declined slightly between Wave 2 and Wave 3.
Labels Impact Index
Figure 2 presents the changes in the LII over the three waves. The LII increased significantly from Wave 1 to Wave 2 (p < .001, β = 3.43, 95% CI = 2.48–4.38) and between Wave 1 and Wave 3 (p < .001, β = 2.86, 95% CI = 1.82–3.91). There was no significant difference in the LII between Wave 2 and Wave 3 (p = .215, β = −0.57, 95% CI = −1.19–0.05).
Figure 2.

Generalized estimating equation analysis showing changes in the Label Impact Index over time.
DISCUSSION
The findings from this study demonstrate that the introduction of PHWs in Mauritius led to a pronounced increase in the indicators of effectiveness of the warnings (IARC, 2008). All indicators of warning salience, and of cognitive and behavioral responses to the warnings significantly increased at the first postimplementation (Wave 2) period compared to the preimplementation (Wave 1) period. These results are similar to those found in ITC studies investigating the effectiveness of warnings in high-income countries, such as Australia (Borland et al., 2009a) and Canada (Hammond et al., 2003), as well as in the few middle-income countries where PHWs have been evaluated, including Thailand (Yong et al., 2013), Malaysia (Fathelrahman et al., 2010), and Mexico (Thrasher et al., 2007, 2010). The common finding that PHWs are more effective than text-only warnings demonstrates the generalizability of the power of graphically depicting the health consequences of tobacco use on warnings. Additionally, these findings support current initiatives to introduce PHWs in other African countries such as South Africa, Kenya, Niger, Burkina Faso, and Chad (Centre for Tobacco Control in Africa, 2014).
Results of this study also showed a decline in PHW effectiveness from Wave 2 to Wave 3 (a period in which PHWs remained unchanged), indicating wearout and emphasizing the importance for the revision of any system of warnings. The warning effectiveness indicators either remained unchanged or, in the case of avoiding warnings, significantly decreased at Wave 3. These findings suggest that PHWs lost effectiveness because smokers were overexposed to the same images and were therefore becoming habituated to them. The fact that avoiding labels was the only indicator that significantly changed (declined) from Wave 2 to Wave 3 further supports the notion of wearout.
Evidence of wearout has been reported in previous literature regarding the impact of health warnings. A study conducted by Hammond et al. (2007) showed declines in salience and impact measures during a 2.5-year period after new text-only warnings were introduced in the United Kingdom. Hitchman et al. (2013) found significant wearout in the effectiveness of PHWs in Canada over a nine-year period (2002–2011); they also found significant wearout, albeit to a lesser degree, in the effectiveness of the text-only warnings in the United States over the same period of time, even though the same warnings had been on cigarette packages in the United States since 1984.
Existing literature has also suggested that PHWs on cigarette packages may be less susceptible to wearout compared to text-only warnings. For example, a study comparing the impact of Mexican text-only warnings to Canadian PHWs found Canadian warnings had significantly higher salience despite having been in circulation for three years longer than the text-only warnings in Mexico (Thrasher et al., 2007). These findings further support the superiority of PHWs over text-only warnings.
Our findings call attention to the rapidity with which wearout occurs. After just a year, the impact of the PHWs in Mauritius leveled off or declined significantly. These results provide evidence supporting the recommendation of the Article 11 Guidelines that governments should build in mechanisms for revising their warnings every 12–36 months (WHO, 2008).
The Mauritius Government gave a plenary presentation of their tobacco control program at the Fifth Conference of the Parties of the FCTC in November 2012 and cited evidence from this study documenting wearout of the warnings as the reason for the Government’s plan to accelerate the revision of their pictorial warnings. Currently, the Mauritian Ministry of Health is in the process of developing eight new PHWs to be released in 2014.
With respect to limitations of this study, it is important to note that some of the usual sources of bias in the typical survey-based study were likely fairly minimal in the ITC Mauritius Survey. For example, attrition is a potential source of bias in a cohort survey, with those who fail to return in some systematic ways from those who remain in the survey. However, the retention rates for this study were extremely high (93% and 96% at the two follow-up waves), and so this is likely to be a minor problem at most, particularly when compared to the very strong effects observed between Wave 1 and Wave 2. As with any cross-country survey, there should be some caution in interpreting the results due to the possible differences in interpretation of the questions. However, the Mauritius team took great care in conducting the translation into Mauritian Creole using fully bilingual project members, following best practices in translation (IARC, 2008). Moreover, given that the pattern of the results showing a strong increase in warning effectiveness after the introduction of PHWs in Mauritius is consistent with evaluation studies of PHWs in several other ITC countries (e.g., Australia, Thailand, Malaysia), these possible differences in interpretation did not affect the findings and the conclusions in any appreciable way.
CONCLUSIONS
In conclusion, this study, which is the first to evaluate PHWs in WHO’s African region, demonstrated that the implementation of PHWs in Mauritius significantly enhanced the effectiveness of their warnings. Additionally, PHWs represent a high-priority tobacco control strategy for enhancing label impact and increasing awareness of the harms of tobacco products among LMICs (including many countries within the African region) given their low cost and high reach.
Overall, the findings of this study affirm the benefits of implementing PHWs as the graphics increased salience, cognitive, and behavioral reactions among smokers. Pictorial warnings, therefore, represent an important tool in increasing awareness of the many negative health consequences of the most harmful consumer product ever created.
FUNDING
This research was funded by the International Development Research Centre (Waves 1 and 2), and partial funding from the Bloomberg Global Initiative-International Union Against Tuberculosis and Lung Disease (Wave 3), and the World Lung Foundation (Wave 3). Support was also provided by the Canadian Institutes of Health Research (79551 and 115016) and the US National Cancer Institute (P01 CA138389 and P50 CA111236). ACG was supported by the CIHR Training Grant in Population Intervention for Chronic Disease Prevention: A Pan-Canadian Program (53893). GTF was supported by a Senior Investigator Award from the Ontario Institute for Cancer Research and a Prevention Scientist Award from the Canadian Cancer Society Research Institute.
DECLARATION OF INTERESTS
None declared.
ACKNOWLEDGMENTS
The authors would like to acknowledge the members of the ITC Mauritius team—Dr. Marie Chan Sun, Ms. Leelmanee Moussa, Mr. D. Mohee, Mrs. V. LeClezio, and Ms. V. Pitchamootoo—for their contributions in planning and implementing the ITC Mauritius Survey, and the fieldwork team who conducted the interviews. We also thank Sylviane Ratte of the International Union Against Tuberculosis and Lung Disease and Sandra Mullin of the World Lung Foundation for their support.
REFERENCES
- Blecher E., Ross H. (2013). Tobacco use in Africa: Tobacco control through prevention Retrieved from http://global.cancer.org/acs/groups/content/@internationalaffairs/documents/document/acspc-041294.pdf
- Borland R., Wilson N., Fong G. T., Hammond D., Cummings M., Yong H, … McNeill A. (2009a). Impact of graphic and text warnings on cigarette packs: Findings from four countries over five years. Tobacco Control, 18, 358–364. 10.1136/tc.2008.028043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borland R., Yong H. H., Wilson N., Fong G. T., Hammond D., Cummings M, … McNeill A. (2009b). How reactions to cigarette packet health warnings influence quitting: Findings from the ITC four-country survey. Addiction, 104, 669–675. 10.1111/j.1360-0443.2009.02508.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canadian Cancer Society. (2012). Cigarette package health warnings international status report (3rd ed). Retr ieved from http://global.tobaccofreekids.org/files/pdfs/en/WL_status_report_en.pdf [Google Scholar]
- Centre for Tobacco Control in Africa. (2014). Pictorial health warnings highest achievements 2012–2013. Retrieved from http://ctc-africa.org/index.php/pictorial- health-warnings-highest-achievements-2012-2013
- Elliott & Shanahan Research. (2009). Literature review: Evaluation of the effectiveness of the graphic health warnings on tobacco product packaging 2008 Prepared for the Australian Government Department of Health and Ageing. Retrieved from www.health.gov.au/internet/main/publishing.nsf/Content/823F3181EBB7F365CA25758800830CD3/$File/lit-rev-hw-eval.pdf
- Fathelrahman A. I., Omar M., Awang R., Cummings K. M., Borland R., Shalihin S. A. (2010). Impact of the new Malaysian cigarette pack warnings on smokers’ awareness of health risks and interest in quitting smoking. International Journal of Environmental Research and Public Health, 7, 4089–4099. 10.3390/ijerph7114089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong G. T., Cummings K. M., Borland R., Hastings G., Hyland A., Giovino G. A, … Thompson M. E. (2006). The conceptual framework of the International Tobacco Control (ITC) Policy Evaluation Project. Tobacco Control, 15(Suppl. 3), iii3–iii11. 10.1136/tc.2005.015438 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong G. T., Hammond D., Hitchman S. C. (2009). The impact of graphic pictures on the effectiveness of tobacco health warnings. Bulletin of the World Health Organization, 87, 640–643. 10.2471/BLT.09.069575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong G. T., Hyland A., Jiang Y., Li Q., Quah A. C. K., Driezen P., Yan M. (2010). Perceptions of tobacco health warnings in China compared with picture and text-only health warnings from other countries: An experimental study. Tobacco Control, 19(Suppl. 2), i69–i77. 10.1136/tc.2010.036483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammond D. (2011). Health warning messages on tobacco products: A review. Tobacco Control, 20, 327–337. 10.1136/tc.2010.037630 [DOI] [PubMed] [Google Scholar]
- Hammond D., Fong G. T., Borland R., Cummings K. M., McNeill A., Driezen P. (2007). Text and graphic warnings on cigarette packages: Findings from the international tobacco control four country study. American Journal of Preventive Medicine, 32, 202–209. 10.1016/j.amepre.2006.11.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammond D., Fong G. T., McDonald P. W., Cameron R., Brown K. S. (2003). Impact of the graphic Canadian warning labels on adult smoking behaviour. Tobacco Control, 12, 391–395. 10.1136/tc.12.4.391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammond D., Fong G. T., McNeill A., Borland R., Cummings K. M. (2006). Effectiveness of cigarette warning labels in informing smokers about the risks of smoking: Findings from the International Tobacco Control (ITC) Four Country Survey. Tobacco Control, 15 Suppl. 3, iii19–iii25. 10.1136/tc.2005.012294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hitchman S. C., Driezen P., Logel C., Hammond D., Fong G. T. (2013). Changes in effectiveness of cigarette health warnings over time in Canada and the United States, 2002–2011. Nicotine & Tobacco Research. Advance online publication. 10.1093/ntr/ntt196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Agency for Research on Cancer. (2008). Methods for evaluating tobacco control policies. In: International Agency for Research on Cancer (IARC) Handbook 12 on Cancer Prevention, Tobacco Control, 287–317. Lyon, France: WHO Press; [Google Scholar]
- ITC Project. (2012a). ITC Mauritius national report: Results of the wave 3 survey. Ontario, Canada: University of Waterloo; [Google Scholar]
- ITC Project (2012b). Health warnings on tobacco packages: ITC cross-country comparison report. Ontario, Canada: University of Waterloo [Google Scholar]
- Liang K., Zeger S. L. (1986). Longitudinal data analysis using generalized linear models. Biometrika, 73, 13–22 [Google Scholar]
- Pampel F. (2008). Tobacco use in sub-Sahara Africa: Estimates from the demographic health surveys. Social Science & Medicine, 66, 1772–1783. 10.1016/j.socs cimed.2007.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steptoe A., Wardle J., Cui W., Baban A., Glass K., Tsuda A., Vinck J. (2002). An international comparison of tobacco smoking, beliefs and risk awareness in university students from 23 countries. Addiction, 97, 1561–1571. 10.1046/j.1360-0443.2002.00269.x [DOI] [PubMed] [Google Scholar]
- Thrasher J. F., Hammond D., Fong G. T., Arillo-Santillán E. (2007). Smokers’ reactions to cigarette package warnings with graphic imagery and with only text: A comparison of Mexico and Canada. Mexican Journal of Public Health, 49, S233–S240. 10.1590/S0036-36342007000800013 [DOI] [PubMed] [Google Scholar]
- Thrasher J. F., Villalobos V., Szklo A., Fong G. T., Pérez C., Sebrié E, … Bianco E. (2010). Assessing the impact of cigarette package health warning labels: A cross-country comparison in Brazil, Uruguay, and Mexico. Mexican Journal of Public Health, 52, S206–S215. 10.1590/S0036-36342010000800016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tumwine J. (2011). Implementation of the framework convention on tobacco control in Africa: Current status of legislation. International Journal of Environmental Research and Public Health, 8, 4312–4331. 10.3390/ijerph8114312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Gemert F., Chavannes N., Nabadda N., Luzige S., Kirenga B., Eggermont C, … van der Molen T. (2013). Impact of chronic respiratory symptoms in a rural area of sub-Saharan Africa: An in-depth qualitative study in the Masindi district of Uganda. Primary Care Respiratory Journal, 22, 300–305. 10.4104/pcrj.2013.00064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. (2003). WHO framework on tobacco control. Geneva, Switzerland: World Health Organization; Retrieved from www.who.int/tobacco/framework/WHO_FCTC_english.pdf [Google Scholar]
- World Health Organization. (2008). Guidelines for implementation of Article 11 of the WHO framework convention on tobacco. Geneva, Switzerland: World Health Organization; Retrieved from www.who.int/fctc/guidelines/article_11.pdf [Google Scholar]
- Yong H. H., Fong G. T., Driezen P., Borland R., Quah A. C., Sirirassamee B, … Omar M. (2013). Adult smokers’ reactions to pictorial health warning labels on cigarette packs in Thailand and moderating effects of type of cigarette smoked: Findings from the International Control Southeast Asia Survey. Nicotine and Tobacco Research, 15, 1339–1347. 10.1093/ntr/nts241 [DOI] [PMC free article] [PubMed] [Google Scholar]