

Abstract
Introduction
Erection hardness is an elemental component of men's sexual quality of life that can be easily measured by the Erection Hardness Score (EHS). However, there are few published data regarding EHS, and there is little understanding of its relationships to aging, men's sexual behavior, sexual confidence, and risk factors in Japan.
Aim
To assess EHS and how it correlates to aging, sexual behaviors, sexual self-confidence, and risk factors in a Japanese population database.
Methods
A web-based cross-sectional nationwide survey conducted between March and May 2009 in Japan.
Main Outcome Measures
EHS, lifestyle factors, comorbidities, general health, sexual confidence, frequency of sexual behaviors, and attitudes toward treatment of erectile dysfunction (ED).
Results
A total of 7,710 men with a mean age of 39.3 ± 13.0 years participated in this survey. In 6,528 participants who were not using phosphodiesterase type 5 inhibitors, 3,540 (54.2%) had EHS ≤ 3 and 1,196 (18.3%) had EHS ≤ 2. We found a significant age-dependent decrease in EHS, sexual confidence, and frequency of sexual activities. Sexual confidence was strongly associated with higher EHS but was also associated with older age groups, presence of offspring, awareness of better general health, and greater frequency of sexual activity. In age-adjusted multivariate logistic regression, risk factors for a lower EHS (defined as EHS ≤ 2) were heavy smoking, which was defined as more than two packs per day (odds ratio [OR], 1.7) or a history of metabolic syndrome (OR, 1.4), hypertension (OR, 1.2), and diabetes mellitus (OR, 1.4).
Conclusions
EHS correlates to various elements, such as aging, sexual behaviors, sexual confidence, and ED-related risk factors, and can be a valuable tool in clinical practice for monitoring and treating ED and thereby improving the quality of life for men and their sexual partners. Kimura M, Shimura S, Tai T, Kobayashi H, Baba S, Kano M, and Nagao K. A web-based survey of Erection Hardness Score and its relationship to aging, sexual behavior, confidence, and risk factors in Japan. Sex Med 2013;1:76–86.
Keywords: Erection Hardness, Erectile Dysfunction, Japanese, Sexual Confidence, Sexual Behavior, ED Risk Factors
Introduction
It has been more than 20 years since the National Institutes of Health Consensus Panel declared that erectile dysfunction (ED) is an important public health issue [1]. The panel emphasized the importance of understanding its etiology, risk factors, pathophysiology, diagnostic assessment, and treatments and the need for further assessment regarding the diversity of ED across geographic, racial, ethnic, socioeconomic, and cultural groups [1]. In this context, several researchers have investigated erectile function, focusing on aforementioned topics using several validated objective measures, such as the International Index Erectile Function (IIEF) [2], Sexual Health Inventory for Men, Sexual Encounter Profile [3], and the Self-Esteem And Relationship Questionnaire (SEAR) [4].
Satisfaction with erection hardness initiates a cascade of psychosocial benefits, such as higher self-confidence and self-esteem, which ultimately lead to overall sexual satisfaction for men and their partners [5]. With the aim of measuring erection hardness as a targeted goal of ED therapy, the Erection Hardness Score (EHS) was developed by Goldstein et al. in the sildenafil clinical trial program [6]. The EHS is a robust, single-item, self-reported tool that scores erection hardness on a four-point scale and can be used in daily clinical practice [5]. Recently, psychometric analysis supported the use of EHS as a simple, reliable, and valid tool for the assessment of erection hardness in the research setting [7], but there are few studies using the EHS in a population-based sample.
Aims
It has been reported that ED is associated with aging, unhealthy lifestyle choices, and comorbidities as well as psychological elements, including low self-esteem, low sexual confidence, depression, anxiety, and relationship problems [8–13]. These findings suggest that ED is a major factor associated with men's physical and mental health. However, there have been no published data from Japan in terms of an investigation of EHS and its relationship with the aforementioned factors. The aim of the present study is to provide updated information about the relationship between EHS and aging, sexual behavior, sexual confidence, and risk factors using a web-based, nationwide, Japanese population database.
Methods
Study Population
A web-based cross-sectional nationwide study was conducted in Japan between March 19 and May 31, 2009. Regarding the enrollment of this study, we recruited the participants through a special website entitled “Hardness of Erected Penis is Pride of Men” in conjunction with a campaign for the 10th anniversary of the introduction of sildenafil to the Japanese market. The targeted population of this survey was nonspecific Japanese male citizens older than 20 years. Because these findings were to be based on an observational web-based survey, we did not set strict exclusion criteria, except for age. They provided informed consent and voluntarily reported their private information. There was no compensation for participants in this study. The survey included questions regarding demographics, lifestyles, comorbidities, self-reported confidence for general and sexual health, EHS, subjective assessment of erectile function, sexual behaviors, attitudes toward ED treatment, and phosphodiesterase type 5 (PDE5) inhibitor use (Appendix 1).
Erection hardness was assessed using the EHS in the provided questionnaire (question 10). Briefly, EHS1 indicates erection hardness at sexual stimulation as larger but not hard, EHS2 indicates hard but not hard enough for penetration, EHS3 indicates hard enough for penetration but not completely hard, and EHS4 indicates completely hard and fully rigid [14]. In the present study, translation and linguistic validation of the Japanese version of EHS were conducted according to accepted methods (forward translation, back translation, and cognitive debriefing) [15]. First, two translators independently reviewed the EHS questionnaire as translated by a Japanese consultant and modified the translation on the basis of cultural differences. Subsequently, a draft of the Japanese version of EHS was produced. Then, cognitive debriefing was performed with five patients with ED, and the appropriateness of expressions and word use were assessed as well as whether questionnaire items were important, meaningful, and generally acceptable. The final decision was made based on discussion in an international harmonization meeting evaluating the first and second versions and back translation to confirm conceptual equivalence during the process of translation and linguistic validation [16].
Main Outcome Measures
The main outcome measures for this study were the EHS, lifestyle factors, comorbidities, general health, sexual confidence, frequency of sexual behaviors, and attitudes toward treatment of ED.
Statistical Analysis
To determine the association among EHS, aging, and sexual behaviors, the Spearman Rank Test was applied to calculate the Spearman rho (r). To determine predictive factors for sexual confidence, we conducted multivariate logistic regression analysis in 7,710 participants. In this model, explanatory variables were age groups (range 1–6), presence of offspring (yes vs. no), self-reported awareness of better health (range 1–5), alcohol consumption (range 1–4), smoking status (range 1–4), history of metabolic syndrome (yes vs. no), medical history of comorbidities including hypertension, dyslipidemia, and diabetes mellitus (yes vs. no), self-reported confidence in erectile function (yes vs. no), EHS (range 1–4), frequency of sexual intercourse (range 1–6), frequency of masturbation (range 1–6), experience with failure of sexual intercourse in past year (yes vs. no), awareness of ED in lifetime (yes vs. no), inclination to visit a clinic for ED treatment (yes vs. no), and PDE5 inhibitor use (yes vs. no). Additionally, to determine predictive factors for a lower EHS (EHS ≤ 2), multivariate logistic regression analyses were employed among 6,528 participants not using PDE5 inhibitors. In this analysis, age groups, lifestyle factors (e.g., alcohol consumption and smoking status), history of metabolic syndrome, and comorbidities (e.g., hypertension, dyslipidemia, and diabetes) were assigned as explanatory variables. Statistical significance was defined as P < 0.05. All statistical analyses were performed with STATA software version 11.2 (Stata Corporation, College Station, TX, USA). Descriptive data are reported as mean ± standard deviation or number (percentage) unless otherwise specified.
Results
Characteristics of the Participants
A total of 7,710 men with a mean age of 39.3 ± 13.0 (ranged from 20 to 89) years participated in this survey. The demographics and clinical characteristics are summarized in Table 1. More than half 4,454 (57.8%) were married, and 3,750 (48.6%) had offspring. In terms of lifestyle factors, 2,714 (35.2%) drank alcohol every day and 4,997 (64.8 %) were nonsmokers. Twenty-four percent had been diagnosed with metabolic syndrome. Regarding comorbidities, 1,538 (20%), 2,003 (26%), and 581 (7.5%) had a history of hypertension, dyslipidemia, and diabetes, respectively. Comparing participants not using PDE5 inhibitors (n = 6,528) with those using PDE5 inhibitors, nonusers were more likely to be younger (37.9 ± 12.5 vs. 46.6 ± 13.1 years) and have a lower rate of alcohol consumption and cigarette smoking and were less likely to have history of metabolic syndrome, hypertension, dyslipidemia, and diabetes (all P < 0.001).
Table 1.
Characteristics of the 7,710 participants
| Number of Participants, % | |
|---|---|
| Marital status | |
| Married | 4,454 (57.8) |
| Unmarried | 3,256 (42.2) |
| Age, year | |
| 20–29 | 1,935 (25.1) |
| 30–39 | 2,304 (29.9) |
| 40–49 | 1,798 (23.3) |
| 50–59 | 966 (12.5) |
| 60–69 | 539 (7.0) |
| ≥70 | 168 (2.2) |
| Presence of offspring | 3,750 (48.6) |
| Alcohol consumption | |
| None | 1,888 (24.5) |
| 2–3 times in a month | 1,455 (18.9) |
| 1–2 times in a week | 1,653 (21.4) |
| Every day | 2,714 (35.2) |
| Smoking status | |
| Nonsmoker | 4,997 (64.8) |
| A few cigarettes per day | 781 (10.1) |
| One pack per day | 1,662 (21.6) |
| More than 2 packs per day | 270 (3.5) |
| Metabolic syndrome | 1,867 (24.2) |
| History of comorbidities | |
| Hypertension | 1,538 (20.0) |
| Dyslipidemia | 2,003 (26.0) |
| Diabetes mellitus | 581 (7.5) |
EHS
Among the 6,528 participants who did not use PDE5 inhibitors, the number of participants with EHS1, EHS2, EHS3, and EHS4 was 431 (6.6%), 765 (11.7%), 2,344 (35.9%), and 2,988 (45.8%), respectively. Furthermore, 3,540 (54.2%) participants had EHS ≤ 3 and 1,196 (18.3%) participants had EHS ≤ 2. Stratifying EHS by age group showed that EHS decreased with increasing age, which was found to be statistically significant by the Spearman rank correlation (r = −0.32, P < 0.001; Figure 1).
Figure 1.
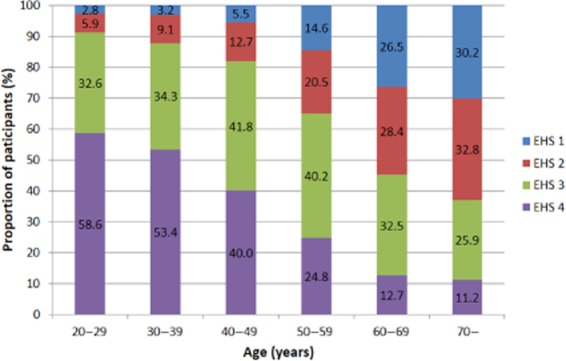
Erection Hardness Score (EHS) in various age groups among 6,528 participants who were not using phosphodiesterase type 5 (PDE5) inhibitors.
Sexual Behaviors
Frequency of sexual activity in 7,710 participants is summarized in Figure 2. With respect to frequency of sexual intercourse, 28% of participants answered “no intercourse within past half-year” whereas 59% had intercourse at least once per month. Regarding frequency of masturbation, 7.6% participants answered “no masturbation within the past half-year,” and 88% masturbated at least once per month, a higher frequency compared with that of sexual intercourse.
Figure 2.
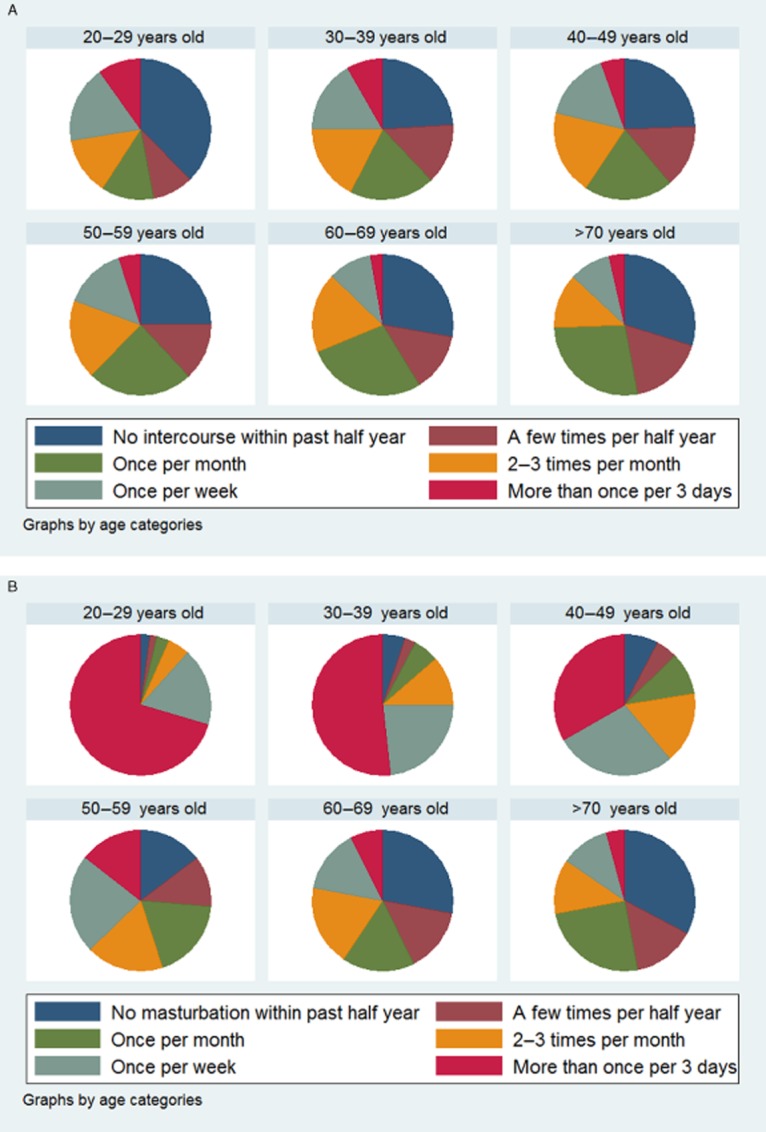
Relationships between aging and sexual behaviors in 7,710 participants. (A) Frequency of sexual intercourse stratified by age categories. (B) Frequency of masturbation stratified by age categories.
There was no association between frequency of sexual intercourse and aging (r = −0.01, P = 0.587; Figure 2A). On the contrary, we found a significant decreased frequency of masturbation with increased age (r = −0.49, P < 0.001; Figure 2B). Among 7,710 participants, a significant positive association was found between EHS and frequency of sexual intercourse (r = 0.17, P < 0.001). Similarly, there was significant positive association between EHS and frequency of masturbation (r = 0.30, P < 0.001).
Frequency of sexual activity stratified with PDE5 inhibitors use in 7,710 participants is summarized in Figure 3. A use of PDE5 inhibitors was significantly increased by age (r = 0.24, P < 0.001; Figure 3A), whereas frequency of sexual intercourse was statistically higher in PDE5 inhibitor user than nonuser (P < 0.001; Figure 3B).
Figure 3.
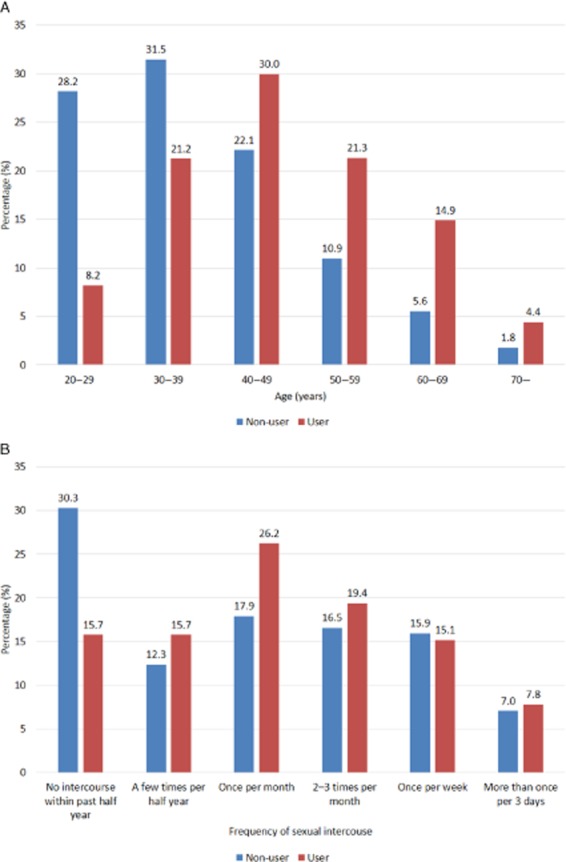
(A) A percentage of PDE5 inhibitors use based on age categories. (B) A percentage of frequency of sexual intercourse based on use of PDE5 inhibitors.
Confidence in Sexual Ability
Of the 7,710 men who participated in the present web-based survey, 3,172 (41.4%) reported confidence in their sexual ability, and 4,538 (58.6%) reported they were not confident. Just as EHS decreased with increased age, there was apparent association between a decrease in men's sexual confidence and older age, which was statistically significant (chi-square test, P = 0.001; Figure 4). Results of multivariate logistic regression for men's sexual confidence are listed in Table 2. In this analysis, higher EHS (odds ratio [OR], 3.36; P < 0.001) was identified as having strong association with confidence in sexual ability. We also found several significant predictive factors, such as age 60 to 69 years (OR, 1.58; P = 0.002), presence of offspring (OR, 1.22; P = 0.003), awareness of better health (OR, 1.24; P < 0.001), higher frequency of sexual intercourse (OR, 1.45; P < 0.001), and masturbation (OR, 1.06; P = 0.002). Conversely, marital status, lifestyle factors (e.g., cigarette smoking, drinking alcohol), metabolic syndrome, and comorbidities did not correlate with sexual confidence.
Figure 4.
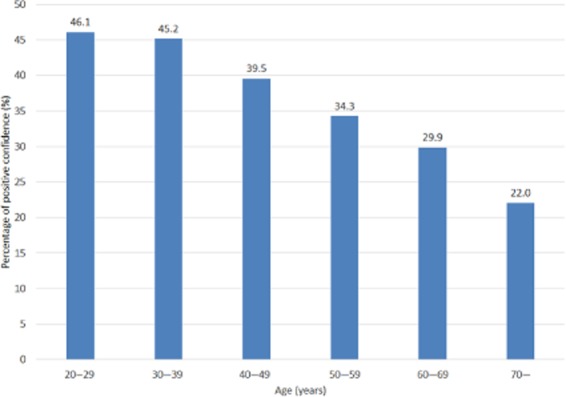
Relationship between men's confidence in sexual ability and aging.
Table 2.
Multivariate logistic regression analysis for men's confidence in sexual ability*
| Covariates | Odds ratio | 95% CI | P value |
|---|---|---|---|
| Age, y | |||
| 20–29 | Reference | — | — |
| 30–39 | 0.96 | 0.83–1.12 | 0.624 |
| 40–49 | 0.99 | 0.82–1.17 | 0.873 |
| 50–59 | 1.12 | 0.88–1.40 | 0.331 |
| 60–69 | 1.58 | 1.18–2.12 | 0.002 |
| ≥70 | 1.08 | 0.66–1.75 | 0.766 |
| Presence of offspring | 1.22 | 1.07–1.40 | 0.003 |
| Awareness of better health | 1.24 | 1.17–1.32 | <0.001 |
| Alcohol consumption | 1.03 | 0.98–1.08 | 0.220 |
| Smoking | 1.02 | 0.96–108 | 0.610 |
| Metabolic syndrome | 1.07 | 0.93–1.23 | 0.367 |
| Hypertension | 1.00 | 0.86–1.16 | 0.997 |
| Hyperlipidemia | 0.95 | 0.83–1.09 | 0.466 |
| Diabetes mellitus | 1.05 | 0.84–1.32 | 0.650 |
| Erection Hardness Score | 3.35 | 3.09–3.65 | <0.001 |
| Frequency of sexual intercourse | 1.45 | 1.40–1.50 | <0.001 |
| Frequency of masturbation | 1.06 | 1.02–1.11 | 0.002 |
Analysis was conducted in 7,710 participants.
CI = confidence interval
Factors Associated with Lower Erectile Hardness Score
Prevalence of low EHS was significantly higher among participants who were heavy smokers and had metabolic syndrome as well as those with a history of hypertension, dyslipidemia, or diabetes (chi-square test, all P < 0.001). Using a multivariate logistic regression model, we examined plausible factors associated with lower EHS (defined as EHS ≤ 2) among 6,528 participants who were not using PDE5 inhibitors (Table 3). The factor most strongly associated with lower EHS was older age, which demonstrated a 16-fold increased likelihood of lower EHS in the oldest (>70 years) compared with the youngest (20–29 years) group. Apart from aging effects, smoker had a 1.1-fold increased odds of low EHS compared with nonsmokers. If smoking status were analyzed as a categorical variable, men who smoke more than two packs per day had a 1.7-fold increased likelihood of low EHS compared with nonsmokers. However, those who drank alcohol did not show a significant association with lower EHS compared with nonalcohol drinkers. In terms of comorbidities, men who had metabolic syndrome demonstrated a 1.4-fold increased likelihood of lower EHS than men who did not. Similarly, history of hypertension and diabetes mellitus increased the likelihood of lower EHS by 1.2- and 1.4-fold, respectively, when compared with men with no history of these comorbidities. In contrast, history of dyslipidemia was not associated with increased likelihood of lower EHS (OR, 1.07; P = 0.368).
Table 3.
Multivariate logistic regression analysis predicting factors associated with EHS ≤ 2*
| Covariates | Odds ratio | 95% CI | P value |
|---|---|---|---|
| Age, year | |||
| 20–29 | Reference | — | — |
| 30–39 | 1.35 | 1.10–1.67 | 0.005 |
| 40–49 | 1.95 | 1.56–2.43 | <0.001 |
| 50–59 | 4.70 | 3.71–5.95 | <0.001 |
| 60–69 | 10.6 | 8.04–14.0 | <0.001 |
| ≥70 | 16.2 | 10.6–24.6 | <0.001 |
| Alcohol consumption | 0.97 | 0.92–1.03 | 0.301 |
| Cigarette smoking | 1.14 | 1.06–1.22 | <0.001 |
| Metabolic syndrome | 1.41 | 1.20–1.67 | <0.001 |
| History of comorbidities | |||
| Hypertension | 1.21 | 1.03–1.43 | 0.023 |
| Dyslipidemia | 1.07 | 0.92–1.26 | 0.368 |
| Diabetes mellitus | 1.38 | 1.09–1.74 | 0.008 |
Analysis was conducted in 6,528 men who were not using phosphodiesterase type 5 inhibitors.
EHS = Erection Hardness Score; CI = confidence interval
Discussion
In this study, we utilized EHS instead of using the IIEF or the Quality of Erection Questionnaire because EHS is simple measure that can be easily used in routine clinical practice, both as a screening tool and a monitoring tool, as well as in clinical trial research as a validated outcome measure [7]. To the best of our knowledge, this is the first study to investigate EHS in a Japanese cohort as well as the first study to elucidate the association between EHS and several factors, including sexual confidence, sexual behaviors, and risk factors. Previous studies investigating the prevalence of ED have reported varying rates, such as 19–36% in the United States [17,18], 32% in France, 32% in Korea, and 45% in the Middle East [19]. With regard to studies in Japan, previously reported prevalence of ED was inconsistent, ranging from 36% to 89% [20–22]. This large difference is likely explained by differences in the definition of ED, methodology, and small sizes of study population. In this study, we analyzed data from 6,528 participants and found that 54% and 18% of surveyed Japanese men had EHS ≤ 3 and EHS ≤ 2, respectively. This is in contrast to an EHS ≤ 3 rate of 26% reported as a result of a telephone survey conducted in Taiwan. The lower rate in the Taiwan study could easily be due to increased embarrassment of participants in the phone interview versus an Internet survey [19].
We found that more than half of adults aged ≥65 years were sexually active (defined as intercourse more than once per month), although the aged population of this survey might have relatively specific characteristics. In previous studies, Japanese men were considered to be less sexually active and to have less interest in their sexual function compared with men in Western countries [23,24]. However, our results show a discrepancy with this previous understanding. Japanese cultural attitudes toward sexuality may have become more liberal in recent decades, perhaps as a result of influence from other countries. Another plausible reason could be the difference of rate of PDE5 inhibitor users between current and previous cohorts. In present-day Japan, PDE5 inhibitors are widely distributed and available at many clinics, which may enhance the sexual ability and activity in older Japanese men. However, regarding treatment for ED among older adults, sexual problems are infrequently discussed with physicians even in the United States [25]. A previous study in two communities showed that there is a greater decline in sexual activity in Japanese men compared with American men, especially in older age groups [23]. However, this could mean that older Japanese men might be more likely to seek treatment for ED, which may reduce the gap of sexual function between Japan and Western countries in this subset of age groups.
One important finding from the present study is that men who have higher EHS are more likely to have higher frequency of sexual activities and higher sexual confidence. Similarly, previous studies from Western countries reported that erection hardness was directly associated with improvement in outcomes, including intercourse enjoyment, sexual satisfaction (i.e., frequency of satisfactory intercourse and satisfaction with sex life and sexual relationship), emotional well-being (i.e., self-esteem, personal relationships, confidence in erectile function, and confidence overall) and satisfaction with their ED treatment [5,26–30]. Although causality is difficult to determine, an implication from our result could be that men who improve their erection hardness through medical intervention, such as use of PDE5 inhibitors, are more likely to become sexually active and confident than men without treatment. Therefore, some effort is warranted in Japan to educate middle-aged and older adults in their sexuality; encouraging communication between physician and patient about sex is essential to maintain or improve sexual health. We expect that the use of EHS in clinical practice could aid this communication.
We found that participants who had higher EHS demonstrated a 3.4-fold increased likelihood of sexual confidence, suggesting that erectile function is a strong predictor for confidence in sexual ability. Previous observations showing an association between ED and depression may further support our findings, given that depression is known to cause low self-esteem/confidence [31,32]. Numerous studies demonstrated that PDE5 inhibitors can improve erectile function in men with ED and are well-tolerated treatments, even in older men [6,33,34]. We found that older men who used PDE5 inhibitors had a higher EHS than men in the same age group who did not, suggesting that the use of PDE5 inhibitors might have resulted in enhancing their sexual confidence.
In the present study, we identified factors that contribute to lower EHS, some of which have not been reported previously in a Japanese population. Because the EHS has a strong convergent relationship with the IIEF Erectile Function (EF) domain [7,35], we assumed that the EHS might correlate with ED risk factors. In addition, EHS is focused only on physiologic factors (i.e., hardness of erect penis), which can represent real physiologic erectile function if the individual's perception is accurate. In this age-adjusted, multivariate, logistic regression analysis, we defined lower EHS as EHS ≤ 2 (i.e., men who responded that their erection is “larger, but not hard” or “hard, but not hard enough for penetration”), representing men with moderate to severe ED by IIEF EF domain evaluation based on the aforementioned studies [7,35]. A similar study from Taiwan analyzing EHS in 1,060 men defined ED as EHS ≤ 3 (i.e., all men who did not respond “completely hard and fully rigid”) [36], which corresponds to mild to severe ED on the IIEF EF domain.
As we expected, aging contributes most strongly to the decline of EHS in multivariate logistic regression analysis (Table 3), which was also reported in several previously published studies [22,23,37]. Examination of the impact of lifestyle factors (e.g., alcohol consumption, cigarette smoking) and metabolic syndrome to EHS has been limited in the Asian population. In present study, we found that cigarette smoking was a significant predictive factor for lower EHS/ED using Japanese population data, but that alcohol consumption had no association, which is consistent with previous reports from Western countries [38–42]. Regarding metabolic syndrome, we found that it too was a significant predictive factor for EHS ≤ 2. However, two previous studies exploring the association between obesity and ED in Japan [21,37] showed that obesity was not identified as a risk factor for ED. This discrepancy might be attributed to a relatively small sample size owing to a lower incidence of obesity in Japanese men, resulting in insufficient statistical power. Comorbidities as risk factors for ED have been well researched in many countries. Hypertension and diabetes were strongly associated with lower EHS, which is consistent with previous reports from Western countries as well as from Japan [20,22,43,44]. In contrast, dyslipidemia was not associated with lower EHS in our study, which contradicts some reports from Western countries [45,46], but is consistent with all previous reports from Japan [20,22,37].
There are several limitations in our study. First, this web-based survey data might have sampling biases because of the nature of web-based cross-sectional data acquisition. Individuals who responded to this survey might be more interested in Japanese sexual function and behavior than those who did not volunteer for this survey. In addition, participants may be younger in this study than other studies because the participants needed to be familiar with current communication technology to access the Internet [20]. By the same token, older participants who have these skills may be more intellectually and sexually active than those of the same age group who do not. Second, the confidence measure on this study is not based on a psychometrically validated measure, such as the SEAR questionnaire, which could weaken present results. Third, the survey did not ask for information regarding drug use. Because some cases of ED could be a side effect of specific medications, such as beta-blockers, we cannot determine causality of ED in men who have comorbidities. Finally, certain participants perhaps could not realize their comorbidity profiles if these are subclinical, which can bias the analyzed results.
Despite these limitations, the present study, to the best of our knowledge, is the largest online survey to evaluate erection hardness using the validated EHS in Asia. This study has updated the knowledge base regarding epidemiology for ED, sexual behaviors, and risk factors in the Japanese population. These results revealed that erection hardness was strongly associated with age, sexual activity, confidence in sexual ability, and risk factors.
Conclusion
We found that there is a significant correlation among older age, a decrease in EHS, confidence in sexual ability, and frequency of sexual activities. In a risk factor analysis, we found that older age (i.e., >70 years [OR, 16.2]) and heavy smoking (OR, 1.7) as well as a history of metabolic syndrome (OR, 1.4), hypertension (OR, 1.2), and diabetes mellitus (OR, 1.4) were significant predictive factors for ED in this Japanese population. When men, regardless of age, encounter problems with erectile function, a conversation about sexual health between physician and patient might be necessary to improve erectile function, which could consequently lead to a better quality of life. Our findings may help encourage men to be aware of their sexual health and seek proper treatment options for ED. The EHS may be useful in aiding the interaction between physician and patient.
Acknowledgments
The authors thank Caroline C. Hadley, BS, for her assistance with manuscript preparation. The authors are also grateful to Dr. Vera Stecher, senior medical director at Pfizer Inc USA for her intellectual advice. Additional editorial support was provided by Diane Werner and Janet E. Matsuura, PhD, of Complete Healthcare Communications, Inc. (Chadds Ford, PA) and was funded by Pfizer Inc.
Appendix 1: Questionnaire Survey
-
Are you married?
Married
Unmarried
How old are you?
-
Do you have children?
Yes
No
-
What is your current general health?
Excellent
Very good
Good
Fair
Poor
-
Do you have a habit of drinking?
None
2–3 times a month
1–2 times a week
Every day
-
Do you smoke?
None
A few cigarettes per day
One pack per day
More than two packs per day
-
Have you ever been diagnosed as having metabolic syndrome?
Yes
No
-
Have you ever been diagnosed as having
hypertension
dyslipidemia
diabetes
No
-
Are you confident in your erection hardness?
Yes
No
-
Which is most frequent condition of your penis during sexual activity?
Larger, but no hard
Hard, but not hard enough for penetration
Hard enough for penetration, but not completely hard
Completely hard and fully rigid
-
How often do you have sexual intercourse?
More than once per 3 days
Once per week
2–3 times per month
Once per month
A few times per half year
No intercourse within past half year
-
How often do you masturbate?
More than once per 3 days
Once per week
2–3 times per month
Once per month
A few times per half year
No masturbation within past half year
-
Do you have experience that you fail to sexual intercourse due to insufficiency of erection during past year?
Yes
No
-
Do you have confidence in your sexual ability to satisfy your partner?
Yes
No
-
Have you ever been aware that you have erectile dysfunction?
Yes
No
-
Do you want to visit a clinic if your erectile function were decreased?
Yes
No
-
Have you used pills for erectile dysfunction such as Viagra, Levitra, Cialis during past year?
Yes
No
Conflict of Interest
The authors report no conflicts of interest.
References
- 1.NIH Consensus Development Panel on Impotence. NIH Consensus Conference. Impotence. JAMA. 1993;270:83–90. [PubMed] [Google Scholar]
- 2.Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11:319–326. doi: 10.1038/sj.ijir.3900472. [DOI] [PubMed] [Google Scholar]
- 3.Goldstein I, Kim E, Steers WD, Pryor JL, Wilde DW, Natanegara F, Wong DG, Ahuja S. Efficacy and safety of tadalafil in men with erectile dysfunction with a high prevalence of comorbid conditions: Results from MOMENTUS: Multiple observations in men with erectile dysfunction in National Tadalafil Study in the US. J Sex Med. 2007;4:166–175. doi: 10.1111/j.1743-6109.2006.00402.x. [DOI] [PubMed] [Google Scholar]
- 4.Cappelleri JC, Althof SE, Siegel RL, Shpilsky A, Bell SS, Duttagupta S. Development and validation of the Self-Esteem And Relationship (SEAR) questionnaire in erectile dysfunction. Int J Impot Res. 2004;16:30–38. doi: 10.1038/sj.ijir.3901095. [DOI] [PubMed] [Google Scholar]
- 5.Mulhall JP, Althof SE, Brock GB, Goldstein I, Jϋnemann K-P, Kirby M. Erectile dysfunction: Monitoring response to treatment in clinical practice—Recommendations of an international consensus panel. J Sex Med. 2007;4:448–464. doi: 10.1111/j.1743-6109.2007.00441.x. [DOI] [PubMed] [Google Scholar]
- 6.Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. N Engl J Med. 1998;338:1397–1404. doi: 10.1056/NEJM199805143382001. [DOI] [PubMed] [Google Scholar]
- 7.Mulhall JP, Goldstein I, Bushmakin AG, Cappelleri JC, Hvidsten K. Validation of the Erection Hardness Score (EHS) J Sex Med. 2007;4:1626–1634. doi: 10.1111/j.1743-6109.2007.00600.x. [DOI] [PubMed] [Google Scholar]
- 8.Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J Urol. 1994;151:54–61. doi: 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 9.Moore TM, Strauss JL, Herman S, Donatucci CF. Erectile dysfunction in early, middle, and late adulthood: Symptom patterns and psychosocial correlates. J Sex Marital Ther. 2003;29:381–399. doi: 10.1080/00926230390224756. [DOI] [PubMed] [Google Scholar]
- 10.Corona G, Mannucci E, Petrone L, Ricca V, Balercia G, Giommi R, Forti G, Maggi M. Psycho-biological correlates of free-floating anxiety symptoms in male patients with sexual dysfunctions. J Androl. 2006;27:86–93. doi: 10.2164/jandrol.05070. [DOI] [PubMed] [Google Scholar]
- 11.Shabsigh R, Perelman MA, Lockhart DC, Lue TF, Broderick GA. Health issues of men: Prevalence and correlates of erectile dysfunction. J Urol. 2005;174:662–667. doi: 10.1097/01.ju.0000165389.73148.d1. [DOI] [PubMed] [Google Scholar]
- 12.Rosen RC, Wing R, Schneider S, Gendrano N., 3rd Epidemiology of erectile dysfunction: The role of medical comorbidities and lifestyle factors. Urol Clin North Am. 2005;32:403–417. doi: 10.1016/j.ucl.2005.08.004. [DOI] [PubMed] [Google Scholar]
- 13.Althof SE, O'Leary MP, Cappelleri JC, Hvidsten K, Stecher VJ, Glina S, King R, Siegel RL. Sildenafil citrate improves self-esteem, confidence, and relationships in men with erectile dysfunction: Results from an international, multi-center, double-blind, placebo-controlled trial. J Sex Med. 2006;3:521–529. doi: 10.1111/j.1743-6109.2006.00234.x. [DOI] [PubMed] [Google Scholar]
- 14.Cappelleri JC, Stecher VJ. An assessment of patient-reported outcomes for men with erectile dysfunction: Pfizer's perspective. Int J Impot Res. 2008;20:343–357. doi: 10.1038/ijir.2008.8. [DOI] [PubMed] [Google Scholar]
- 15.Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J Clin Epidemiol. 1993;46:1417–1432. doi: 10.1016/0895-4356(93)90142-n. [DOI] [PubMed] [Google Scholar]
- 16.Nagao K. Development of Japanese version for Erection Hardness Score (EHS) Jpn J Sex Med. 2009;24:1–3. [Google Scholar]
- 17.Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: Prevalence and predictors. JAMA. 1999;281:537–544. doi: 10.1001/jama.281.6.537. [DOI] [PubMed] [Google Scholar]
- 18.Braun M, Wassmer G, Klotz T, Reifenrath B, Mathers M, Engelmann U. Epidemiology of erectile dysfunction: Results of the “Cologne Male Survey”. Int J Impot Res. 2000;12:305–311. doi: 10.1038/sj.ijir.3900622. [DOI] [PubMed] [Google Scholar]
- 19.Shaeer O, Shaeer K. The Global Online Sexuality Survey (GOSS): Ejaculatory function, penile anatomy, and contraceptive usage among Arabic-speaking Internet users in the Middle East. J Sex Med. 2012;9:425–433. doi: 10.1111/j.1743-6109.2011.02338.x. [DOI] [PubMed] [Google Scholar]
- 20.Sasayama S, Ishii N, Ishikura F, Kamijima G, Ogawa S, Kanmatsuse K, Kimoto Y, Sakuma I, Nonogi H, Matsumori A, Yamamoto Y. Men's Health Study: Epidemiology of erectile dysfunction and cardiovascular disease. Circ J. 2003;67:656–659. doi: 10.1253/circj.67.656. [DOI] [PubMed] [Google Scholar]
- 21.Imai A, Yamamoto H, Hatakeyama S, Iwabuchi I, Yoneyama T, Hashimoto Y, Koie T, Kamimura N, Danjyo K, Ohyama C. Risk factors for erectile dysfunction in healthy Japanese men. Int J Androl. 2010;33:569–573. doi: 10.1111/j.1365-2605.2009.00974.x. [DOI] [PubMed] [Google Scholar]
- 22.Marumo K, Nakashima J, Murai M. Age-related prevalence of erectile dysfunction in Japan: Assessment by the International Index of Erectile Function. Int J Urol. 2001;8:53–59. doi: 10.1046/j.1442-2042.2001.00258.x. [DOI] [PubMed] [Google Scholar]
- 23.Masumori N, Tsukamoto T, Kumamoto Y, Panser LA, Rhodes T, Girman CJ, Lieber MM, Jacobsen SJ. Decline of sexual function with age in Japanese men compared with American men—Results of two community-based studies [In Process Citation] Urology. 1999;54:335–344. doi: 10.1016/s0090-4295(99)00108-9. discussion 44–45. [DOI] [PubMed] [Google Scholar]
- 24.Namiki S, Kwan L, Kagawa-Singer M, Terai A, Arai Y, Litwin MS. Urinary quality of life after prostatectomy or radiation for localized prostate cancer: A prospective longitudinal cross-cultural study between Japanese and U.S. men. Urology. 2008;71:1103–1108. doi: 10.1016/j.urology.2008.02.025. [DOI] [PubMed] [Google Scholar]
- 25.Lindau ST, Schumm LP, Laumann EO, Levinson W, O'Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357:762–774. doi: 10.1056/NEJMoa067423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Stecher VJ, Collins S, Wang H. Improvement in erection quality is associated with treatment satisfaction and improved self-esteem, confidence, and sexual relationship satisfaction. J Urol. 2006;175:7–7. [Google Scholar]
- 27.King R, Juenemann KP, Levinson IP, Stecher VJ, Creanga DL. Correlations between increased erection hardness and improvements in emotional well-being and satisfaction outcomes in men treated with sildenafil citrate for erectile dysfunction. Int J Impot Res. 2007;19:398–406. doi: 10.1038/sj.ijir.3901549. [DOI] [PubMed] [Google Scholar]
- 28.Althof SE, Berner MM, Goldstein I, Claes HI, Cappelleri JC, Bushmakin AG, Symonds T, Schnetzler G. Interrelationship of sildenafil treatment effects on the physiological and psychosocial aspects of erectile dysfunction of mixed or organic etiology. J Sex Med. 2010;7:3170–3178. doi: 10.1111/j.1743-6109.2010.01882.x. [DOI] [PubMed] [Google Scholar]
- 29.Donatucci C, Taylor T, Thibonnier M, Bangerter K, Gittelman M, Casey R. Vardenafil improves patient satisfaction with erection hardness, orgasmic function, and overall sexual experience, while improving quality of life in men with erectile dysfunction. J Sex Med. 2004;1:185–192. doi: 10.1111/j.1743-6109.2004.04027.x. [DOI] [PubMed] [Google Scholar]
- 30.Glina S, Damiao R, Abdo C, Afif-Abdo J, Tseng LJ, Stecher V. Self-esteem, confidence, and relationships in Brazilian men with erectile dysfunction receiving sildenafil citrate: A randomized, parallel-group, double-blind, placebo-controlled study in Brazil. J Sex Med. 2009;6:268–275. doi: 10.1111/j.1743-6109.2008.01026.x. [DOI] [PubMed] [Google Scholar]
- 31.Kubin M, Wagner G, Fugl-Meyer AR. Epidemiology of erectile dysfunction. Int J Impot Res. 2003;15:63–71. doi: 10.1038/sj.ijir.3900949. [DOI] [PubMed] [Google Scholar]
- 32.Sugimori H, Yoshida K, Tanaka T, Baba K, Nishida T, Nakazawa R, Iwamoto T. Relationships between erectile dysfunction, depression, and anxiety in Japanese subjects. J Sex Med. 2005;2:390–396. doi: 10.1111/j.1743-6109.2005.20354.x. [DOI] [PubMed] [Google Scholar]
- 33.Sharlip ID, Shumaker BP, Hakim LS, Goldfischer E, Natanegara F, Wong DG. Tadalafil is efficacious and well tolerated in the treatment of erectile dysfunction (ED) in men over 65 years of age: Results from Multiple Observations in Men with ED in National Tadalafil Study in the United States. J Sex Med. 2008;5:716–725. doi: 10.1111/j.1743-6109.2007.00712.x. [DOI] [PubMed] [Google Scholar]
- 34.Giuliano F, Donatucci C, Montorsi F, Auerbach S, Karlin G, Norenberg C, Homering M, Segerson T, Eardley I, Vardenafil Study G. Vardenafil is effective and well-tolerated for treating erectile dysfunction in a broad population of men, irrespective of age. BJU Int. 2005;95:110–116. doi: 10.1111/j.1464-410X.2004.05260.x. [DOI] [PubMed] [Google Scholar]
- 35.Cappelleri JC, Bushmakin AG, Symonds T, Schnetzler G. Scoring Correspondence in Outcomes Related to Erectile Dysfunction Treatment on a 4-Point Scale (SCORE-4) J Sex Med. 2009;6:809–819. doi: 10.1111/j.1743-6109.2008.01155.x. [DOI] [PubMed] [Google Scholar]
- 36.Hwang TI, Tsai TF, Lin YC, Chiang HS, Chang LS. A survey of erectile dysfunction in Taiwan: Use of the erection hardness score and quality of erection questionnaire. J Sex Med. 2010;7:2817–2824. doi: 10.1111/j.1743-6109.2010.01837.x. [DOI] [PubMed] [Google Scholar]
- 37.Terai A, Ichioka K, Matsui Y, Yoshimura K. Association of lower urinary tract symptoms with erectile dysfunction in Japanese men. Urology. 2004;64:132–136. doi: 10.1016/j.urology.2004.02.019. [DOI] [PubMed] [Google Scholar]
- 38.Feldman HA, Johannes CB, Derby CA, Kleinman KP, Mohr BA, Araujo AB, McKinlay JB. Erectile dysfunction and coronary risk factors: Prospective results from the Massachusetts male aging study. Prev Med. 2000;30:328–338. doi: 10.1006/pmed.2000.0643. [DOI] [PubMed] [Google Scholar]
- 39.McVary KT, Carrier S, Wessells H Subcommittee on S, Erectile Dysfunction Socioeconomic Committee SMSoNA. Smoking and erectile dysfunction: Evidence based analysis. J Urol. 2001;166:1624–1632. [PubMed] [Google Scholar]
- 40.Rosen MP, Greenfield AJ, Walker TG, Grant P, Dubrow J, Bettmann MA, Fried LE, Goldstein I. Cigarette smoking: An independent risk factor for atherosclerosis in the hypogastric-cavernous arterial bed of men with arteriogenic impotence. J Urol. 1991;145:759–763. doi: 10.1016/s0022-5347(17)38444-6. [DOI] [PubMed] [Google Scholar]
- 41.Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Glasser DB, Rimm EB. A prospective study of risk factors for erectile dysfunction. J Urol. 2006;176:217–221. doi: 10.1016/S0022-5347(06)00589-1. [DOI] [PubMed] [Google Scholar]
- 42.Mirone V, Imbimbo C, Bortolotti A, Di Cintio E, Colli E, Landoni M, Lavezzari M, Parazzini F. Cigarette smoking as risk factor for erectile dysfunction: Results from an Italian epidemiological study. Eur Urol. 2002;41:294–297. doi: 10.1016/s0302-2838(02)00005-2. [DOI] [PubMed] [Google Scholar]
- 43.Naya Y, Mizutani Y, Ochiai A, Soh J, Kawauchi A, Fujito A, Nakamura N, Ono T, Iwamoto N, Aoki T, Marumo K, Murai M, Miki T. Preliminary report of association of chronic diseases and erectile dysfunction in middle-aged men in Japan. Urology. 2003;62:532–536. doi: 10.1016/s0090-4295(03)00383-2. [DOI] [PubMed] [Google Scholar]
- 44.Sasaki H, Yamasaki H, Ogawa K, Nanjo K, Kawamori R, Iwamoto Y, Katayama S, Shirai M. Prevalence and risk factors for erectile dysfunction in Japanese diabetics. Diabetes Res Clin Pract. 2005;70:81–89. doi: 10.1016/j.diabres.2005.02.018. [DOI] [PubMed] [Google Scholar]
- 45.Wei M, Macera CA, Davis DR, Hornung CA, Nankin HR, Blair SN. Total cholesterol and high density lipoprotein cholesterol as important predictors of erectile dysfunction. Am J Epidemiol. 1994;140:930–937. doi: 10.1093/oxfordjournals.aje.a117181. [DOI] [PubMed] [Google Scholar]
- 46.Blanker MH, Bosch JL, Groeneveld FP, Bohnen AM, Prins A, Thomas S, Hop WC. Erectile and ejaculatory dysfunction in a community-based sample of men 50 to 78 years old: Prevalence, concern, and relation to sexual activity. Urology. 2001;57:763–768. doi: 10.1016/s0090-4295(00)01091-8. [DOI] [PubMed] [Google Scholar]