

Abstract
We report a man presenting with dyspnea, cough, and hemoptysis due to left lung collapse from an endobronchial tumor obstructing the left main bronchus. Endobronchial biopsy of the tumor showed renal cell carcinoma, identical to a previous specimen of renal cell carcinoma removed by a radical left nephrectomy five years ago. The endobronchial tumor was removed by snare diathermy through a flexible bronchoscope, following which his symptoms resolved and the left lung re-expanded. Endobronchial metastasis from renal cell carcinoma is rare and can mimic obstruction from other endobronchial etiologies, such as bronchogenic carcinoma. Total lung collapse as a result is even more uncommon, although atelectasis is well described. Endobronchial techniques, such as snare diathermy, can relieve obstruction, providing symptom palliation even in advanced disease.
Keywords: Endobronchial metastasis, renal cell carcinoma, snare diathermy, total lung collapse
Introduction
Endobronchial metastases secondary to extrathoracic malignancies are rare [1]. Such metastases causing entire lung collapse have not been reported to date. We report a case of left lung collapse caused by endobronchial metastasis from renal cell carcinoma resected five years ago.
Case Report
A 63-year-old man, a former smoker with a 45 pack-years smoking history, presented with reduced effort tolerance for four months and cough with blood-streaked sputum for three months. Twelve weeks earlier, he had sought treatment at another hospital where a chest radiograph taken was normal. He was treated for chronic obstructive pulmonary disease without clinical improvement. One week prior to his presentation to us, he presented to another hospital with frank hemoptysis and dyspnea. A chest radiograph taken revealed complete left lung collapse. He was then referred to our institution.
On examination, he had a respiratory rate of 30 breaths per minute with an oxygen saturation of 92% breathing room air. The trachea was deviated to the left and there was reduced left-sided chest wall movement. Percussion note was dull and breath sounds were reduced throughout the left hemithorax. He had a left nephrectomy scar.
Thoracic computed tomography (CT) scan revealed left lung collapse and a left main bronchus endobronchial lesion (Fig. 1). During bronchoscopy, a white polypoidal mass was found totally occluding the left main bronchus (Fig. 2). The necrotic appearing surface of this mass was removed piecemeal with a biopsy forceps to reveal a hemorrhagic core, which was then biopsied.
Figure 1.
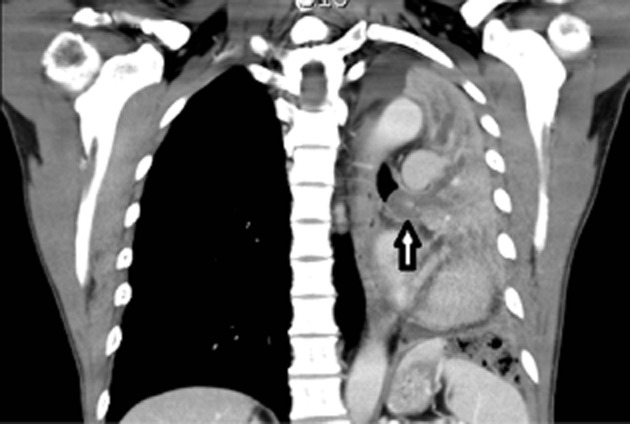
Computed tomography of the chest shows the intraluminal occlusion in the left main bronchus causing left lung collapse (coronal view).
Figure 2.

Flexible bronchoscopy revealed a white polypoidal mass occluding the left main bronchus.
The biopsied specimen revealed renal cell carcinoma. A review of his records from another hospital revealed that he underwent a radical left nephrectomy five years ago for a solitary Fuhrman grade 2 renal cell carcinoma involving the upper two-thirds of the kidney with no renal vein or large vessel invasion. The surgical margins were clear. No adjuvant therapy was given. Ultrasonography one year later did not reveal any evidence of local recurrence.
During a second flexible bronchoscopy, the left main bronchus tumor was excised by diathermy using a snare around the base of the tumor. A follow-up chest radiograph four weeks later revealed a fully expanded left lung. He was subsequently treated with pazopanib, an angiogenesis inhibitor for advanced renal cell carcinoma.
Discussion
The lung is a common site for metastasis from extrathoracic tumors, but endobronchial metastases are rare [2]. Metastatic involvement of a major airway was found in only 2%–5% of autopsies performed on patients who died of extrapulmonary malignancies [2]. A retrospective analysis of 438 cases of endobronchial malignancies biopsied in Korea over a period of 10 years revealed only 18 (4.1%) to be of extrapulmonary in origin [1]. The most common extrathoracic malignancies associated with endobronchial metastases are breast, colorectal, and renal cell carcinoma 1–4. Of 82 patients who underwent radical nephrectomy for renal cell carcinoma at a centre in South Korea, only four patients (5%) had endobronchial metastases [5].
The most common symptoms are dyspnea, cough, and hemoptysis as seen in this patient 1–3. The mean interval from the initial diagnosis of the primary tumor to the diagnosis of endobronchial metastases ranges from zero to 112 months [1, 3, 5]. Endobronchial metastases can involve any airway level but have a predilection for the right lung in up to 80% of cases, although the reason for this is not clear [4]. This case was rather unique in that the tumor occluded the left main bronchus, resulting in left lung collapse. The five years delay in presentation is a little unusual but has been reported in patients with long-term survival [5].
The therapeutic approach to an endobronchial tumor is determined by the characteristics of the primary tumor, biological behavior, anatomic location of the endobronchial metastasis, and the patient's performance status [4]. We chose snare diathermy for its convenience and safety. In conclusion, endobronchial techniques, such as snare diathermy, can relieve obstruction, providing symptom palliation even in advanced disease.
Acknowledgments
We wish to thank Ken-Siong Kow, Chee-Kuan Wong, and Raymond George Varughese for their support toward our work.
Disclosure Statements
No conflict of interest declared.
Appropriate written informed consent was obtained for publication of this case report and accompanying images.
References
- 1.Kim JH, Min D, Song SH, et al. Endobronchial metastases from extrathoracic malignancies: recent 10 years' experience in a single university hospital. Tuberc. Respir. Dis. 2013;74:169–176. doi: 10.4046/trd.2013.74.4.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Braman SS, Whitcomb ME. Endobronchial metastasis. Arch. Intern. Med. 1975;135:543–547. [PubMed] [Google Scholar]
- 3.Akoglu S, Ucan ES, Celik G, et al. Endobronchial metastases from extrathoracic malignancies. Clin. Exp. Metastasis. 2005;22:587–591. doi: 10.1007/s10585-005-5787-x. [DOI] [PubMed] [Google Scholar]
- 4.Kiryu T, Hoshi H, Matsui E, et al. Endotracheal/endobronchial metastases: clinicopathologic study with special reference to developmental modes. Chest. 2001;119:768–775. doi: 10.1378/chest.119.3.768. [DOI] [PubMed] [Google Scholar]
- 5.Park CM, Goo JM, Choi HJ, et al. Endobronchial metastasis from renal cell carcinoma: CT findings in four patients. Eur. J. Radiol. 2004;51:155–159. doi: 10.1016/S0720-048X(03)00209-2. [DOI] [PubMed] [Google Scholar]