

Abstract
Key Clinical Message
Right atrial thrombus is a rare medical emergency that should be suspected in all cases of pulmonary embolism, and rapid action should be taken to ensure a timely, proper management.
Keywords: Autopsy, free-floating thrombus, pulmonary embolism, right atrium
Introduction
For a 52-year-old patient with a fatal right atrial free-floating mass, at autopsy the presence of a heterogeneous mass in the pulmonary artery trunk was found. In this case we stress the importance of maintaining a high degree of alert for right atrial thrombus in all suspected pulmonary embolism.
Free-floating right atrial thrombus is a rare entity 1. It often appears as an irregular, curvilinear mass, moving from the right atrium to the right ventricle, simulating a myxoma 1. It can come from an embolus from a deep vein thrombosis, thus called “emboli-in-transit” 2. We describe the case of a patient with a large free-floating thrombus of the right atrium, whose evolution was fatal.
Case Report
A 52-year-old patient with a history of a long travel (720 km) by road, 1 month prior to presentation and which was followed by a painful swelling of the left lower limb that resolved spontaneously, was admitted for a left-sided chest pain of moderate intensity radiating to the epigastrium and associated with dyspnea at rest. Blood pressure was 100/60 mmHg in both arms, a heart rate of 115 beats per min, respiratory rate of 36 breaths per min, and a temperature of 36.5°C. Cardiovascular examination revealed regular heart sounds with no murmurs, a slightly raised jugular venous pressure, and pulses of good volume. There was a slight increase in volume of the left lower limb with discrete inflammatory signs. There were no signs of heart failure.
Laboratory studies found a normal hemoglobin level at 15 g/dL, thrombocytopenia of 51,000/mm3, an elevated serum C-reactive protein of 24 mg/L, and prothrombin level of 50.9%. Transthoracic electrocardiogram inscribed a regular sinus tachycardia with a heart rate of 114 cycles per min, an anterior hemiblock, an S1S2S3 pattern, and a low voltage in the limb leads.
Chest X-ray showed a slight cardiomegaly (cardiothoracic index = 0.56) with the apex above the diaphragm. Venous Doppler ultrasound of the lower limbs showed thrombosis in the left limb veins – middle and distal – superficial femoral veins, popliteal, peroneal, and posterior tibial.
Transthoracic echocardiography (Figs.1 and 2) showed:
A huge heterogeneous, polylobulated, horseshoe-shaped mass, floating in the right atrium, protruding into the right ventricle in diastole;
A rounded heterogeneous mass of 3.7 cm2 in the pulmonary artery trunk;
A moderate dilatation of the right heart chambers (right ventricle = 34 mm; right atrium = 25 cm2); and
Mild pulmonary hypertension (pulmonary arterial systolic pressure of 42 mmHg).
Figure 1.
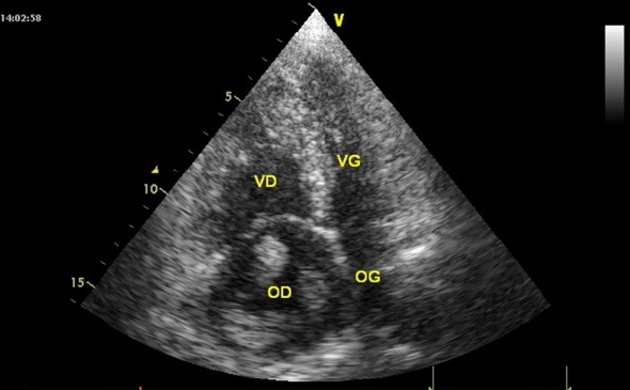
A transthoracic echocardiographic image; apical four-chamber view showing a dilatation of right chambers and a voluminous heterogeneous, polylobulated horseshoe-shaped mass, in the right atrium.
Figure 2.
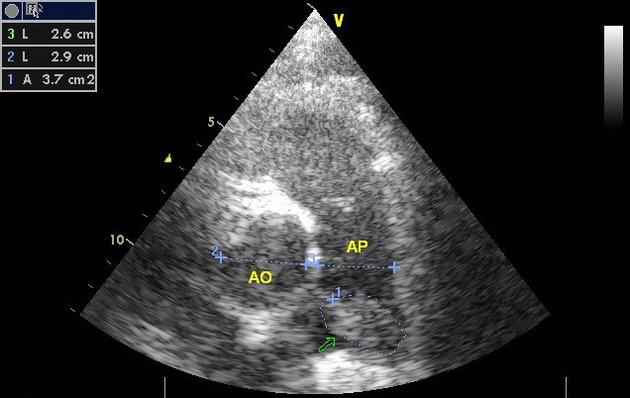
Parasternal short axis showing a rounded heterogeneous mass (arrow) of 3.7 cm2 in the trunk of the pulmonary artery (AO = 29 cm, AP = 26 cm). AO, aorta; AP, pulmonary artery.
The patient received oxygen therapy, anticoagulation with low-molecular-weight heparin (Lovenox 0.8 mL twice daily), vitamin K antagonist in the form of acenocoumarol (Sintrom) 4 mg daily, and Tramadol (Trabar) 50 mg thrice daily. He did not receive any treatment prior to admission. Given the high probability of pulmonary embolism associated with a huge thrombus in the right atrium, the indication for surgery was made. However, the evolution was marked by the sudden death of the patient. Autopsy done revealed the presence of a nonadherent clot in the right ventricle, completely obstructing the opening of the trunk of the pulmonary artery (Fig.3). The heart size was big with left ventricular hypertrophy of 2 cm. Furthermore, there were no signs of pulmonary embolism.
Figure 3.
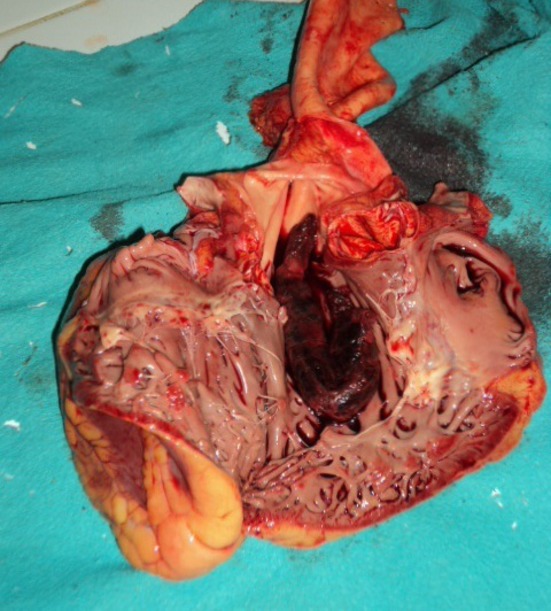
At autopsy, section of RV showing the presence of a nonadherent clot (arrow) in the right ventricle placed like a loop completely obstructing the opening of the pulmonary artery trunk.
Discussion
Intracavitary masses, including primitive or metastatic tumors, thrombi, vegetations, and calcification of a tricuspid valve or annulus, are uncommon in the right cavities 1. Similarly, free-floating thrombus of the right atrium is rare 1,3. The first cases were reported in the 1980s in patients with pulmonary embolism 1. It can come from emboli from deep vein thrombosis which are temporarily trapped in the right chambers and which are on their way toward the pulmonary circulation, thus called “emboli-in-transit” 2. Such was the case in our patient with extensive deep vein thrombosis of the left lower limb, probably lasting for a month.
Free-floating right atrial thrombus is almost exclusively found in the presence of clinical manifestations of pulmonary embolism 3, and in this context, transthoracic echocardiography is the technique of choice for detection 2,4. Transesophageal echocardiography can be performed in case of doubt 3. It appears as an irregular mass, curvilinear, floating freely in the right atrium and then moving from the atrium to the right ventricle through the tricuspid valve, so it can simulate a myxoma 1. In our patient who presented with a clinical picture suggestive of pulmonary embolism, echocardiography was able to detect such a mass.
Free-floating thrombus of the right atrium is a medical emergency because of the high risk of mortality 2,3; however, the most appropriate treatment is yet to be determined 2,5. In a series by Chartier et al. 3, 21.1% of patients died the same day of admission, and among those who had a very huge mobile thrombus, the hospital mortality rate was 44.7% due to the occurrence of a sudden pulmonary embolism.
Thrombolysis may be recommended as a first choice in the treatment of right atrial thrombus 6–9, and can cause the complete disappearance of the thrombus 10 and hence recommended as a bridge to surgery. 3 In case of large mobile thrombi, it is advisable to do an emergency surgery 2.
Any delay between the diagnosis and the treatment can be fatal for the patient, as was the case in our report.
Conclusion
Free-floating thrombus of the right atrium is a rare entity, and must be sought in all cases of suspected pulmonary embolism. Transthoracic echocardiography is the technique of choice for detection; transesophageal echocardiography can be used in case of doubt. It requires urgent management due to the high risk of mortality. Thrombolysis may result in the complete disappearance of the thrombus; however, emergency surgery is justified in the case of a large thrombus.
Conflict of Interest
None declared.
Funding Information
No funding information provided.
References
- Panidis I, Kotler M, Mintz G. Ross J. Clinical and echocardiographic features of right atrial masses. Am. Heart J. 1984;107:745–758. doi: 10.1016/0002-8703(84)90324-7. [DOI] [PubMed] [Google Scholar]
- European Working Group on Echocardiography. The European Cooperative Study on the clinical significance of right heart thrombi. Eur. Heart J. 1989;10:1046–1059. doi: 10.1093/oxfordjournals.eurheartj.a059427. [DOI] [PubMed] [Google Scholar]
- Chartier L, Béra J, Delomez M, Asseman P, Beregi JP, Bauchart JJ, et al. Free-floating thrombi in right heart: diagnosis, management, and prognostic indexes in 38 consecutive patients. Circulation. 1999;99:2779–2783. doi: 10.1161/01.cir.99.21.2779. [DOI] [PubMed] [Google Scholar]
- Acikel M, Erol MK, Yekeler I. Ozyazicioglu A. A case of free-floating thrombus in right atrium with tricuspid stenosis. Int. J. Cardiol. 2004;94:329–330. doi: 10.1016/j.ijcard.2003.04.042. [DOI] [PubMed] [Google Scholar]
- Kinney EL. Wright RJ. Efficacy of treatment of patients with echocardiographically detected right sided heart thrombi: a meta-analysis. Am. Heart J. 1989;118:569–573. doi: 10.1016/0002-8703(89)90274-3. [DOI] [PubMed] [Google Scholar]
- Goldhaber SZ. Optimal strategy for diagnosis and treatment of pulmonary embolism due to right atrial thrombus. Mayo Clin. Proc. 1988;63:1261–1264. doi: 10.1016/s0025-6196(12)65416-0. [DOI] [PubMed] [Google Scholar]
- Cuccia C, Campana M, Franzoni P, Faggiano P, Volterrani M, Musmeci G, et al. Effectiveness of intravenous rt-PA in the treatment of massive pulmonary embolism and right heart thromboembolism. Am. Heart J. 1993;126:468–472. doi: 10.1016/0002-8703(93)91075-p. [DOI] [PubMed] [Google Scholar]
- Leclercq F, Messner-Pellenc P, Beigbeder JY, Albat B, Thévenet A. Grolleau-Raoux R. Thrombus flottant de l'oreillette droite et embolie pulmonaire grave: intérêt de la thrombolyse intraveineuse. Arch. Mal. Coeur Vaiss. 1994;87:805–811. [PubMed] [Google Scholar]
- Goldhaber SZ, Nagel JS, Theard M, Levine JD. St John Sutton MG. Treatment of right atrial thrombus with urokinase. Am. Heart J. 1988;115:894–897. doi: 10.1016/0002-8703(88)90894-0. [DOI] [PubMed] [Google Scholar]
- Mansencal N. Dubourg O. Free-floating thrombus in right heart and pulmonary embolism. Int. J. Cardiol. 2006;112:e33–e34. doi: 10.1016/j.ijcard.2006.02.018. [DOI] [PubMed] [Google Scholar]