

Abstract
Background
The reinforcing value of food is a reliable index of motivation to eat and energy intake. Obese adults find food more reinforcing than do nonobese adults.
Objective
The present study was designed to assess whether the relative reinforcing value of food differs as a function of weight status in 8–12-y-old children and whether the relative reinforcing value of food differs depending on the types of available nonfood alternatives.
Design
The reinforcing value of pizza (experiment 1) or snack foods (experiment 2) was measured on progressive ratio schedules of reinforcement in nonoverweight and overweight children. Experiment 2 also compared the relative reinforcing value of food and 2 nonfood alternatives: time to spend playing a hand-held video game or time to spend reading magazines or completing word searches or mazes.
Results
In both experiments, overweight children found food more reinforcing and consumed more energy than did their leaner peers. In experiment 2, the relative reinforcing value of food versus sedentary activity was higher in overweight children, but lower in nonover-weight children, regardless of the type of alternative activity available.
Conclusions
These results show that overweight children find food more reinforcing than do nonoverweight children. This individual difference was replicated in different experiments using different types of foods and food alternatives. These studies provide support for studying food reinforcement as a factor associated with overweight and obesity.
INTRODUCTION
Obesity is a disorder of positive energy balance, with energy intake exceeding energy expenditure. One of the factors that may relate to the positive energy balance in obese individuals is the difference in the motivation to eat (1). Food is a primary reinforcer because the motivation to eat does not need to be learned. One empirical index of motivation to eat is the reinforcing value of food. Reinforcing value is defined by how hard an individual is willing to work to gain access to a commodity (2). The reinforcing value of food can be measured in the laboratory by having individuals perform operant responses for portions of food on a progressive ratio schedule of reinforcement (3). Those who respond more for food find food more reinforcing and may allocate more time and effort to eating than do individuals who do not find food as reinforcing (1, 4).
Eating is often a choice that is made among several behavioral alternatives; thus, the study of the reinforcing value of food when it is the only behavioral option may not be a good index of eating in a naturalistic setting. One way to study eating in the context of multiple behavioral alternatives is to measure the relative reinforcing value of food and nonfood alternatives. The relative reinforcing value of food is the amount of work an individual will perform to gain access to food when multiple foods or nonfood alternatives are concurrently available. Research has shown that nonoverweight adults substituted healthy foods and sedentary activities for snack foods as the work required to gain access to snack foods increased (5). However, overweight individuals may find eating very reinforcing, whereas having fewer pleasurable alternatives in which to engage (6, 7) and may, thus, be more resistant to shifting behavioral allocation away from eating toward alternative activities.
Research has shown that overweight adults find food more reinforcing than leaner adults (4, 8, 9). Adult smokers (10) and nonsmokers (8) who find food reinforcing consume more food in an ad libitum eating situation than do individuals who do not find food highly reinforcing. To our knowledge there has been no research on the relation between weight status and the reinforcing value of food in children. In experiment 1, the reinforcing value of food was compared between nonoverweight and overweight children. Because eating is often a choice among several different alternative activities, and behavioral choice may differ depending on the reinforcing value of or access to alternatives (2), experiment 2 examined the relative reinforcing value of food and different types of nonfood alternatives (hand-held video games and mazes, word searches, and magazines) in nonoverweight and overweight children. Finally, previous research has shown that food liking and motivation to obtain food are independent processes that are regulated by different neurobiological systems (11–13), and studies in adults have shown that food reinforcement is a better predictor of energy intake than are food hedonics (8, 14). Childhood and adolescence are critical periods for the development of adult obesity (15); therefore, it is important to understand eating behavior in children as well as in adults. This study sought to determine whether our previous findings in adults extend to children.
SUBJECTS AND METHODS
Participants
In experiment 1, participants included 45 children aged 8–12 y (n = 20 overweight and n = 25 nonoverweight) recruited from an existing database, posted flyers, school, and mass mailings. Overweight was defined as equal to or greater than the 90th body mass index (BMI) percentile and nonoverweight at less than the 75th BMI percentile (16). Children were excluded if their BMI percentile was between the 75th and 89th percentiles to maintain separation between groups. Children were also excluded if they were below the 10th BMI percentile, did not report at least a moderate (4 on a 7 point Likert scale) liking for the foods and food alternatives used in the study, had a cold or upper respiratory distress that could influence olfactory and/or taste cues, had current psychopathology or developmental disability, had food allergies to the study food, or used medications or conditions that could influence taste, appetite, or olfactory sensory responsiveness (eg, methylphenidate).
In experiment 2, participants included 45 children aged 8–12 y (n = 23 overweight and n = 22 nonoverweight) recruited from an existing database, posted flyers, and word of mouth. At risk of overweight or overweight was defined as equal to or greater than the 85th BMI percentile and nonoverweight as less than the 85th BMI percentile (16). Unlike the first experiment, children were not excluded if they were between the 75th and 89th BMI percentile to provide a more continuous assessment of BMI percentile values. All other exclusionary criteria were the same as in experiment 1.
Procedures
In experiment 1, interested parents were screened by phone, and eligible subjects were scheduled for 2 laboratory sessions on a weekend day around the usual lunchtime. At the first session, consent and assent forms were administered to both the parent and child. The parents then completed a questionnaire about demographics and socioeconomic level (17), and the children filled out a pizza liking scale assessed using a 7-point Likert scale anchored by “do not like” (1) and “like very much” (7). The children then had a 10-min exposure to activities that were alternatives to eating (hand-held video games, coloring, drawing materials, and popular children magazines), and the children completed the 7-point Likert rating scale and chose their favorite of these activities to be used in the experiment. Participants were instructed in the computer choice task and were provided practice on the task. The families were told that their children would be given a snack when they came to the laboratory for their next session and were asked to not let their children eat or exercise for ≥3 h before their appointment.
On arrival at the second session, the children were brought into the experiment room and filled out a 7-point Likert hunger scale anchored by “extremely hungry” (1) and “extremely full” (7), and a same-day food recall was conducted to determine adherence to the protocol. The children then consumed a preload of a Kellogg’s Krave Bar (Battle Creek, MI; 48 g, 200 kcal, 6 g fat, 30 g carbohydrate, 7 g protein) with a glass of water. The preload is designed to reduce hunger and food deprivation, because food deprivation will increase the reinforcing value of food (18, 19), and the reinforcer sensitivity theory suggests that the reinforcing value of food is best studied under nondeprivation conditions (20). The participant then engaged in the computer task to determine the reinforcing value of food. Postsession hunger levels were assessed, and a Dutch Eating Behavior Questionnaire was used to assess dietary restraint (21). A score of >8 on the Dutch Eating Behavior Questionnaire was considered high in dietary restraint. Finally, the height (cm) and weight (lb) of the children were measured with a Digi-Kit digital stadiometer (North Bend, WA) and a Tanita digital weight scale (Arlington Heights, IL), respectively, while the children were wearing light clothing and no shoes and after having voided. These measurements were then used to calculate BMI (in kg/m2), and BMI values were converted to BMI percentiles and zBMI (16). The participants were rescheduled if they had eaten within 3 h of their arrival or did not consume the preload (n = 1). The participants received $20 at the completion of the experiment.
In experiment 2, interested parents were screened by phone, and eligible subjects were scheduled for 2 laboratory sessions during the week between the hours of 1400 and 1730. Parents were instructed that their children were to refrain from eating or drinking anything other than water for 3 h before each experimental session. At the beginning of the first session, consent and assent forms were administered to both the parents and the children; the parents completed a questionnaire about demographics, and the children filled out a food-liking scale according to a 5-point Likert-type scale anchored by “do not like” (1) and “like very much” (5) and a food-ranking scale in which they ranked their liking of potato chips (Frito Lay, Purchase, NY), Skittles (Mars Inc, McLean, VA), and M&Ms (Mars Inc). Children, with the help of a parent, also completed a same-day dietary recall to ensure that they adhered to the experimental guidelines. The parents were then excused to the waiting area while their children consumed a preload of a Quaker (Chicago, IL) chewy granola bar (oatmeal raisin or cinnamon and sugar; 90 kcal). The preload used in experiment 1 was no longer available. The children then had a 10-min exposure to activities that were alternatives to eating. During one visit, the alternative was a hand-held video game (Game Boy; Nintendo Inc, Redmond, WA) with 3 different games: Frogger, Super Mario Brothers, and Brain Teasers. During another visit, the children had access to word searches, magazines, and mazes. The order of these visits was counterbalanced. At the end of the sampling period, the children were asked to rate their liking of each nonfood alternative on a 5-point Likert-type scale anchored by “do not like” (1) and “like very much” (5). They were also asked to rank these activities, and their favorite alternative was chosen for the experiment. Next, children rated their hunger on a 5-point scale anchored by “extremely hungry” (1) and “extremely full” (5). The children were then instructed in the computer choice task and were provided practice on the task (described above). Subjects then engaged in the computer task to determine the reinforcing value of food. The session ended when the participant stated that they no longer wished to earn points for food or food alternatives. Postsession hunger levels were assessed along with the Dutch Eating Behavior Questionnaire to assess dietary restraint (21). At the end of the second session, height and weight were obtained as described above. On the basis of height and weight, BMI (kg/m2) was calculated and converted to BMI percentile and zBMI (16). The participants were rescheduled if they had eaten within 3 h of their arrival (n = 1) or did not consume the entire preload (n = 0). The participants received a $40 gift card to a local mall at the completion of the experiment.
Assessment of reinforcing value of food
In experiment 1, the experimental environment included a computer station on which the participants earned points toward pizza or the food alternative. The computer screen displayed 3 boxes that varied in shape and color, which rotated and changed color each time the mouse button was pressed. A point was awarded each time the shapes matched. The schedule of reinforcement began at a variable ratio (VR4/VR4) concurrent schedule, which meant that, for the food and nonfood alternative, one point was awarded for 4 button presses on average. After 5 points were earned, a portion of pizza (80 g; 188 kcal) or 5 min to spend engaged in an alternative activity was awarded. The progressive ratio schedule for the food item doubled (VR8, VR16, VR32, VR64, VR128, and VR256) each time the children earned 5 points, while the schedule for the food alternative remained at VR4. Water was available ad libitum. The food alternatives included a hand-held video game, a popular children’s magazines, and drawing and coloring materials.
In experiment 2, the computer task used to assess reinforcing value and the laboratory environment were the same as described above. In this experiment, both the food and the nonfood alternative were earned on independent, progressive ratio schedules beginning at VR4 and doubling each time (VR4, VR8, VR16, VR32, VR64, VR128, VR256, VR512, and VR1024). Point totals were displayed at the top of the screen; 5 points was worth a 50-kcal portion of the snack food that the participant ranked the highest. Water was available ad libitum. Earning 5 points on the computer for the nonfood alternative provided the children 2 min of access to their highest ranked alternative. The reward was changed from experiment 1 because we wanted to make the time engaged in eating and alternative activities similar, and, based on previous studies with these types of foods, children took, on average, 1–2 min to consume each food portion.
Laboratory environment
The experimental room was interfaced with an intercom and a video camera for communication. The laboratory used for this experiment was specially constructed for eating experiments. The laboratory is equipped with an air-delivery system that circulates new air through each room ≈10 times/h and HEPA air purifiers containing a CPZ (carbon, permanganate, zeolite) filter to remove airborne odorants. All procedures were conducted in accordance with National Institutes of Health guidelines for the ethical conduct of research in human participants and with the approval of the University at Buffalo Children & Youth Institutional Review Board.
Analytic plan
Participant characteristics; baseline hunger, food, and nonfood alternative hedonic ratings; and choice of nonfood alternatives were assessed using analysis of variance and chi-square tests, where appropriate, with weight status and sex as the between subjects variables. Any factors that differed as a function of weight status were used as covariates in the remaining analyses. Changes in hunger from before to after the session were analyzed by repeated-measures analysis of covariance (ANCOVA) with weight status as the between-subjects factor, pre-and post session hunger as the repeated measure, and dietary restraint as the covariate. In experiment 1, differences in laboratory energy intake were determined by AN-COVA with weight status and sex as the between-subjects factors and dietary restraint score as the covariate. In experiment 2, differences in laboratory energy intake were determined with a mixed-effects regression model (MRM), with zBMI, sex, age, preexperimental hunger, and dietary restraint score as time-invariant predictors and type of alternative as the time-variant predictor. Reinforcing value was analyzed with an MRM to compare the pattern of operant responding as a function of schedules of reinforcement for food with zBMI, sex, age, preexperimental hunger, and dietary restraint as time-invariant predictors and schedule of reinforcement (experiment 1 = VR4 – VR256; experiment 2 = VR4 – VR1024) as the time-variant predictor. For experiment 2, type of alternative behavior (hand-held video games, mazes, word searches, and magazines) was also included as a time-variant predictor. Each of the time-invariant predictors was tested as a moderator of responding by interacting it with zBMI and schedule of reinforcement (22). Because more trials were added to experiment 2, the progressive ratio schedules of reinforcement showed an increase followed by a late-session decrease in responding (2); the MRM included both linear and quadratic components. Improvement of fit of the linear plus quadratic trends was tested using a 2-tailed log likelihood test with 2 df. In both experiments, the relation among the reinforcing value of food, liking of food, and energy intake was determined by using Pearson product-moment correlation coefficients.
RESULTS
Experiment 1
Participant characteristics, hedonics, and hunger levels are presented in Table 1. Overweight children had significantly greater weight, percentage overweight values, and dietary restraint (all P < 0.05). Twenty-seven percent of the participants were minorities.
TABLE 1.
Characteristics of participants and baseline hunger by experiment and weight status1
| Experiment 1
|
Experiment 2
|
|||||
|---|---|---|---|---|---|---|
| Nonoverweight2 | Overweight3 | P | Nonoverweight2 | Overweight3 | P | |
| Sex (M/F) | 15/10 | 10/10 | NS | 11/11 | 11/12 | NS |
| Age | 10.7 ± 1.2 | 10.2 ± 1.0 | NS | 10.3 ± 1.4 | 10.9 ± 1.5 | NS |
| Height | 142.5 ± 9.6 | 146.9 ± 8.6 | NS | 141.3 ± 9.9 | 148.2 ± 12.2 | NS |
| Weight | 77.0 ± 13.3 | 119.6 ± 15.7 | <0.0001 | 75.9 ± 13.8 | 116.2 ± 23.0 | <0.0001 |
| zBMI | −0.09 ± 0.5 | 1.9 ± 0.3 | <0.0001 | −0.03 ± 0.8 | 1.5 ± 0.6 | <0.0001 |
| Overweight (%) | −0.56 ± 6.4 | 49.2 ± 14.6 | <0.0001 | 1.0 ± 9.2 | 38.7 ± 21.1 | <0.0001 |
| Restraint score | 4.0 ± 2.4 | 7.0 ± 2.7 | 0.0003 | 3.7 ± 2.4 | 6.6 ± 2.7 | 0.001 |
| Baseline hunger | 4.8 ± 1.4 | 5.1 ± 1.2 | NS | 2.5 ± 0.9 | 2.3 ± 0.8 | NS |
Differences in participant characteristics were analyzed by using ANOVA and chi-square tests where appropriate.
Defined as <75th BMI percentile in experiment 1 and <85th BMI percentile in experiment 2.
Defined as ≥90th BMI percentile in experiment 1 and ≥85th BMI percentile in experiment 2.
There were no significant differences as a function of weight status in the type of alternative activity chosen (P >0.10). There were, however, sex differences in the choice of alternative (P = 0.0003); boys were more likely to choose the video game (20/25), and girls were more likely to choose the reading materials (11/19). There were no differences in hedonic ratings of pizza between the overweight (6.0 ± 0.9) and nonoverweight (6.0 ± 1.0) youth (P > 0.05). Similarly, there were no differences in liking of the favorite nonfood alternative between the overweight (6.7 ± 0.7) and nonoverweight (6.4 ± 0.8) youth. There were no differences in baseline hunger (F[1, 42] = 0.62, P = 0.42). A significant reduction in hunger (P < 0.001) was observed from before (6.0 ± 0.5) to after (2.4 ± 0.7) the session, but no differences in hunger reduction were observed between the overweight (−3.6 ± 0.9) and nonoverweight (−3.6 ×1.2) youth (P >0.60).
There was a significant interaction of zBMI and reinforcement schedule (P < 0.001); children with higher zBMI values responded significantly more for food as the reinforcement schedules progressed (Figure 1A). For the purposes of exploring the interaction with zBMI, children were divided into nonover-weight (<85th BMI percentile or <1 zBMI unit) or at risk of overweight or overweight (≥85th BMI percentile or ≥1 zBMI unit; 15). None of the time-invariant predictors (dietary restraint, age, sex, and preexperimental hunger) acted as moderators in this model. Overweight youth consumed significantly more energy than leaner youth (P = 0.003; Figure 1B), and boys consumed significantly more energy than did the girls (P < 0.001); however, there were no interactions between sex and weight status (P = 0.47).
FIGURE 1.
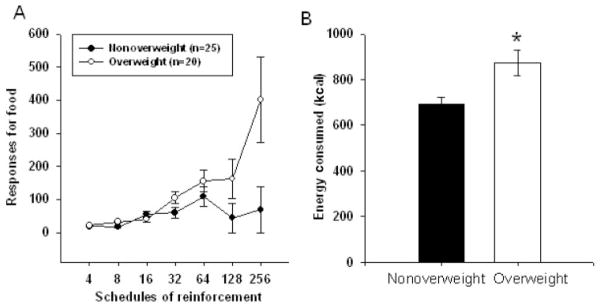
Results from experiment 1. A: Mean ( ± SEM) number of responses at each schedule of reinforcement in nonoverweight (<75th BMI percentile; n = 25) and overweight (≥90th BMI percentile; n = 20) children. Reinforcing value was analyzed with a mixed-effects regression model to compare the pattern of operant responding as a function of schedules of reinforcement for food with zBMI, sex, age, preexperimental hunger, and dietary restraint as time-invariant predictors and schedule of reinforcement (VR4 – VR256) as the time-variant predictor. There was a significant interaction of zBMI and reinforcement schedule (P <0.001), with children with higher zBMI values responding significantly more for food as the reinforcement schedules progressed. B: Mean ( ± SEM) energy consumed in the laboratory in nonoverweight and overweight children. Differences in laboratory energy intake were determined by using ANCOVA with weight status and sex as the between-subjects factors and dietary restraint score as the covariate. Overweight children made significantly more responses for food over trials (P = 0.044). *Significantly different from nonoverweight children, P = 0.003.
There was a significant correlation between reinforcing value and laboratory energy intake (r = 0.59, P < 0.001), but no relation between food liking and energy intake (r = −0.06, P = 0.27). In addition, the reinforcing value of food was not related to food liking (r = −0.03, P = 0.83).
Experiment 2
Participant characteristics, hedonics, and baseline hunger are shown in Table 1. The overweight group had a significantly higher body weight, BMI, BMI percentile, percentage overweight, zBMI, and dietary restraint score (all P < 0.05). The overweight group had a significantly smaller percentage of parents whose highest educational achievement was a college degree and a significantly greater percentage of parents who completed a graduate degree (P <0.01). Twenty-four percent of the participants were minorities.
There were no differences in the liking of any of the foods or activities, with the exception of magazines, which were rated as significantly less liked by the overweight children than by the nonoverweight children (P = 0.02). There were no sex differences in the self-rated liking of video games (P = 0.46), word searches, mazes, and magazines (P = 0.09). All groups showed a significant decrease in hunger after the session (P <0.001). No differences between the groups (P = 0.23) were observed; non-overweight children reduced hunger by 1.3 ± 0.8 and overweight children by 1.4 ± 0.9.
The MRM showed a significant interaction among weight status, reinforcement schedule, and type of reinforcer (food or nonfood alternative) (P < 0.001). The overweight children always found food more reinforcing than nonfood alternatives, regardless of the alternative, whereas the nonoverweight children found nonfood alternative more reinforcing than food (Figure 2). None of the potential moderators had any effect on this interaction. In addition, there was a significant interaction of zBMI and reinforcement schedule (P < 0.001) (Figure 2).
FIGURE 2.
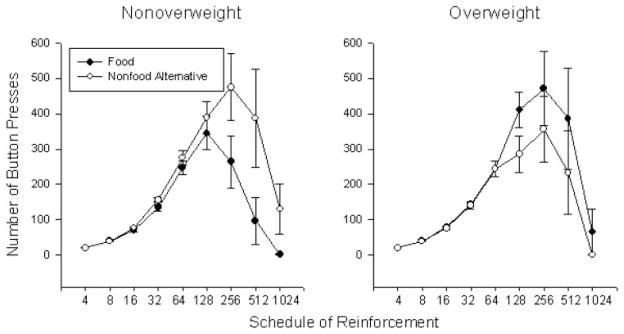
Mean ( ± SEM) number of points earned for food or nonfood alternatives (ie, activity) in nonoverweight (<85th BMI percentile; n = 22) and overweight (≥85th BMI percentile; n = 23) children. Reinforcing value was analyzed with mixed-effects regression models with zBMI, sex, age, preexperimental hunger, parental education, liking of magazines, and dietary restraint score as time-invariant predictors and schedule of reinforcement (VR4 – VR1024) and type of alternative (hand-held video games, mazes, word searches, and magazines) as the time-variant predictors. There was a significant interaction between weight status, type of reinforcer, and schedule of reinforcement such that overweight children found food more reinforcing than nonfood alternatives, and nonoverweight children found food less reinforcing than nonfood alternatives (P = 0.003). There was no interaction with type of activity.
There was a main effect of zBMI (P = 0.019; Figure 3) on laboratory energy intake; overweight children consumed more energy than did the nonoverweight children. There was also a main effect of type of nonfood alternative (P < 0.001) on energy intake; more energy was consumed when the mazes, words searches, and magazines were the alternative than when the alternative was the hand-held video game. There was no interaction between zBMI and type of alternative (P = 0.48). There was a significant interaction between zBMI and dietary restraint score on laboratory energy intake (P = 0.03); energy intake increased as restraint scores increased in children with lower zBMI scores, but energy intake decreased as restraint scores increased in children with higher zBMI scores.
FIGURE 3.

Mean ( ± SEM) amount of energy consumed in the laboratory in nonoverweight (≥85th BMI percentile) and overweight (≥85th BMI percentile) children. Differences in laboratory energy intake were determined with a mixed-effects regression model with zBMI, sex, age, preexperimental hunger, and dietary restraint score as time-invariant predictors and type of alternative (hand-held video game versus mazes, word searches, and magazines) as the time-variant predictor. There was a main effect of weight status: *significantly different from nonoverweight children, P = 0.036.
There was a significant correlation between reinforcing value and laboratory energy intake (r < 0.73, P < 0.001), but no relation between food liking and energy intake (r = 0.12, P = 0.42) and no correlation between food reinforcement and food liking (r = 0.15, P = 0.33) were found.
DISCUSSION
This study tested 2 hypotheses related to the influence of weight status on food reinforcement and energy intake. The first hypothesis was that food reinforcement and energy intake are higher in overweight than in nonoverweight children. We found in both studies that overweight children were more motivated to work for food and consumed more energy in the laboratory than did their leaner peers, as was previously shown in adults (9, 23). The second hypothesis was that food reinforcement is a better predictor of energy intake and weight status than are food hedonics. We found that motivation to obtain food was strongly correlated with both zBMI and energy intake, but self-reported liking for foods was not. These findings were replicated in 2 different experiments using similar methods, but different foods and nonfood alternatives. The greater reinforcing value of food in overweight children may be an important individual difference contributing to chronic excess energy intake, which can lead to overweight and obesity.
Consistent with research in adults (8), at risk of overweight and overweight children find food more reinforcing than do nonover-weight children. This suggests that the relation between weight status and food reinforcement can be established in childhood. Pediatric overweight predicts adult obesity (24), and studying factors that influence child eating behaviors may provide information that is useful in the treatment of pediatric obesity and the prevention of adult obesity. Although research has shown that overweight children and adults find food more reinforcing than do their leaner peers, there may be differences in the factors that influence the reinforcing value of food in children and adults. For example, there are aspects of motivated behavior that change as a function of age, such as behavioral impulsivity (25) and vulnerability to onset of addictive behaviors (26). Studying factors that modify food reinforcement in children may improve our understanding of child-specific influences on motivation to eat and energy intake.
Eating is often a choice that is made in the context of other behavioral alternatives. We found that overweight children responded more for food than did leaner children as the requirements to gain access to food increased, but there was no difference in choice when the response requirements were low and equal. Thus, in a typical choice situation in which subjects have equal access to the alternatives without constraints on the behaviors, nonoverweight and overweight children may make similar choices. However, when constraints are placed on access to food, overweight and nonoverweight children may make different choices about how to allocate their response effort.
Children who find food highly reinforcing are more motivated to eat and may choose to engage in activities that are compatible with eating, thereby increasing their access to food. For example, nonoverweight children spend more time engaged in physical activity than do their overweight peers, which is typically incompatible with eating, whereas overweight children engage in sedentary activities, such as television watching, which is compatible with eating (27). Studies in adults and children have shown that eating while watching television increases energy intake by 30–50% relative to control conditions (28–30). Therefore, one potential method to indirectly reduce energy intake may be to limit access to sedentary behaviors that are compatible with eating, such as television watching. Consistent with that hypothesis, we previously showed a significant reduction in energy intake when television watching was reduced (30). A second approach to reducing energy intake would be to not place constraints on sedentary activities or eating directly, but to forbid eating while engaged in these activities. A previous study in children showed that motivation to gain access to food was significantly increased by the presence of television relative to food alone, which suggests that the combination of television and food may be more reinforcing than either one alone (30). Thus, not allowing eating while engaged in complementary sedentary activities may reduce the reinforcing value of both the food as well as the sedentary activity.
In addition to differences in food reinforcement as a function of weight status, results showed that reinforcing value, or motivation to obtain food, and hedonic ratings of food were not related. Previous research with adults has shown that food reinforcement and liking are relatively independent processes and that food reinforcement is a better predictor of energy intake than is liking (8, 14). These, along with our current findings, support the hypothesis that motivation to obtain food and food hedonics are dissociable processes (11–13). We showed that while self-reported liking for foods and nonfood alternatives had no effect on energy intake, motivation to obtain food was highly correlated with energy intake. One possible reason that liking did not predict energy intake in this study was that the foods used were all highly liked, highly palatable foods, so there was little variability in the liking scores. These results need to be replicated and extended to other types of foods with different macronutrient compositions and a broader range of liking. Another limitation of this study was that it is possible that the preload acted as a priming stimulus for overweight children, but not nonoverweight children and, as a result, increased eating more for overweight than for leaner youth. For example, research shows that recent consumption of food decreases eating in nonoverweight individuals but increases eating in overweight individuals (31–33).
The results from these experiments support the hypothesis that motivation to eat differs as a function of weight status and is related to energy intake. These studies were limited to overweight youth in the 8–12-y-old age range and to specific high-energy-density foods. Research is needed to extend these findings to children of other ages and to study other types of foods. In addition, because overweight children and adults consistently demonstrate high levels of food reinforcement, future research should focus on determining ways to reduce the reinforcing value of food and/or to shift motivation away from eating and toward motivation to engage in other types of activities (34). One challenge to this, as we found in this study, was that when constraints are placed on access to preferred foods, overweight children are more resistant to shifting their efforts toward a nonfood reinforcer. Perhaps, instead of a sedentary activity, other healthier food options could be offered without constraints as an alternative to high-energy-density foods. Future studies are needed to determine the relative reinforcing value of healthy and less healthy foods in nonoverweight and overweight children to begin to explore strategies to translate these basic findings to clinical settings.
Acknowledgments
We thank Brian Wrotniak for assistance with subject recruitment.
Footnotes
The authors’ responsibilities were as follows—CML and AMG: primarily responsible for data collection and data entry; and JLT, S-JS, and LHE: responsible for data analysis, interpretation, and manuscript preparation. LHE is a consultant for Kraft Foods. None of the other authors had any potential conflicts of interest.
References
- 1.Epstein LH, Saelens BE. Behavioral economics of obesity: food intake and energy expenditure. In: Bickel WK, Vuchinich RE, editors. Reframing health behavior change with behavioral economics. Philadelphia, PA: Lawrence Erlbaum; 2000. pp. 293–311. [Google Scholar]
- 2.Bickel WK, Marsch LA, Carroll ME. Deconstructing relative reinforcing efficacy and situating the measures of pharmacological reinforcement with behavioral economics: a theoretical proposal. Psychopharmacology (Berl) 2000;153:44–56. doi: 10.1007/s002130000589. [DOI] [PubMed] [Google Scholar]
- 3.Epstein LH, Leddy JJ, Temple JL, Faith MS. Food reinforcement and eating: a multilevel analysis. Psychol Bull. 2007;133:884–906. doi: 10.1037/0033-2909.133.5.884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Saelens BE, Epstein LH. Reinforcing value of food in obese and non-obese women. Appetite. 1996;27:41–50. doi: 10.1006/appe.1996.0032. [DOI] [PubMed] [Google Scholar]
- 5.Goldfield GS, Epstein LH. Can fruits and vegetables and activities substitute for snack foods? Health Psychol. 2002;21:299–303. [PubMed] [Google Scholar]
- 6.Doell SR, Hawkins RC. Pleasures and pounds: an exploratory study. Addict Behav. (2) 1982;7:65–9. doi: 10.1016/0306-4603(82)90026-0. [DOI] [PubMed] [Google Scholar]
- 7.Jacobs SB, Wagner MK. Obese and nonobese individuals: behavioral and personality characteristics. Addict Behav. 1984;9:223–6. doi: 10.1016/0306-4603(84)90062-5. [DOI] [PubMed] [Google Scholar]
- 8.Epstein LH, Temple JL, Neaderhiser BJ, Salis RJ, Erbe RW, Leddy JJ. Food reinforcement, the dopamine D2 receptor genotype, and energy intake in obese and nonobese humans. Behav Neurosci. 2007;121:877–86. doi: 10.1037/0735-7044.121.5.877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Johnson WG. Effect of cue prominence and subject weight on human food-directed performance. J Pers Soc Psychol. 1974;29:843–8. doi: 10.1037/h0036390. [DOI] [PubMed] [Google Scholar]
- 10.Epstein LH, Wright SM, Paluch RA, et al. Relation between food reinforcement and dopamine genotypes and its effect on food intake in smokers. Am J Clin Nutr. 2004;80:82–8. doi: 10.1093/ajcn/80.1.82. [DOI] [PubMed] [Google Scholar]
- 11.Berridge KC, Robinson TE. What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Brain Res Rev. 1998;28:309–69. doi: 10.1016/s0165-0173(98)00019-8. [DOI] [PubMed] [Google Scholar]
- 12.Berridge KC, Robinson TE. Parsing reward. Trends Neurosci. 2003;26:507–13. doi: 10.1016/S0166-2236(03)00233-9. [DOI] [PubMed] [Google Scholar]
- 13.Robinson TE, Berridge KC. Addiction. Annu Rev Psychol. 2003;54:25–53. doi: 10.1146/annurev.psych.54.101601.145237. [DOI] [PubMed] [Google Scholar]
- 14.Epstein LH, Wright SM, Paluch RA, et al. Food hedonics and reinforcement as determinants of laboratory food intake in smokers. Physiol Behav. 2004;81:511–7. doi: 10.1016/j.physbeh.2004.02.015. [DOI] [PubMed] [Google Scholar]
- 15.Dietz WH. Periods of risk in childhood for the development of adult obesity—what do we need to learn? J Nutr. 1997;127(suppl):1884S–6S. doi: 10.1093/jn/127.9.1884S. [DOI] [PubMed] [Google Scholar]
- 16.Kuczmarski RJ, Ogden CL, Guo SS, et al. CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2000;2002:1–190. [PubMed] [Google Scholar]
- 17.Hollingshead AB. Four factor index of social status. New Haven, CT: Yale University; 1975. [Google Scholar]
- 18.Lappalainen R, Epstein LH. A behavioral economics analysis of food choice in humans. Appetite. 1990;14:81–93. doi: 10.1016/0195-6663(90)90002-p. [DOI] [PubMed] [Google Scholar]
- 19.Raynor HA, Epstein LH. The relative-reinforcing value of food under differing levels of food deprivation and restriction. Appetite. 2003;40:15–24. doi: 10.1016/s0195-6663(02)00161-7. [DOI] [PubMed] [Google Scholar]
- 20.Reiss S, Havercamp S. The sensitivity theory of motivation: implications for psychopathology. Behav Res Ther. 1996;34:621–32. doi: 10.1016/0005-7967(96)00041-1. [DOI] [PubMed] [Google Scholar]
- 21.Hill AJ, Pallin V. Dieting awareness and low self-worth: related issues in 8-year-old girls. Int J Eat Disord. 1998;24:405–13. doi: 10.1002/(sici)1098-108x(199812)24:4<405::aid-eat7>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 22.Kraemer HC, Frank E, Kupfer DJ. Moderators of treatment outcomes: clinical, research, and policy importance. JAMA. 2006;296:1286–9. doi: 10.1001/jama.296.10.1286. [DOI] [PubMed] [Google Scholar]
- 23.Saelens BE, Epstein LH. The rate of sedentary activities determines the reinforcing value of physical activity. Health Psychol. 1999;18:655–9. doi: 10.1037//0278-6133.18.6.655. [DOI] [PubMed] [Google Scholar]
- 24.Guo SS, Roche AF, Chumlea WC, Gardner JD, Siervogel RM. The predictive value of childhood body mass index values for overweight at age 35 y. Am J Clin Nutr. 1994;59:810–9. doi: 10.1093/ajcn/59.4.810. [DOI] [PubMed] [Google Scholar]
- 25.Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev. 2000;24:417–63. doi: 10.1016/s0149-7634(00)00014-2. [DOI] [PubMed] [Google Scholar]
- 26.Wagner FA, Anthony JC. From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology. 2002;26:479–88. doi: 10.1016/S0893-133X(01)00367-0. [DOI] [PubMed] [Google Scholar]
- 27.Epstein LH, Roemmich JN, Paluch RA, Raynor HA. Physical activity as a substitute for sedentary behavior in youth. Ann Behav Med. 2005;29:200–9. doi: 10.1207/s15324796abm2903_6. [DOI] [PubMed] [Google Scholar]
- 28.Bellisle F, Dalix AM, Slama G. Non food-related environmental stimuli induce increased meal intake in healthy women: comparison of television viewing versus listening to a recorded story in laboratory settings. Appetite. 2004;43:175–80. doi: 10.1016/j.appet.2004.04.004. [DOI] [PubMed] [Google Scholar]
- 29.Blass EM, Anderson DR, Kirkorian HL, Pempek TA, Price I, Koleini MF. On the road to obesity: television viewing increases intake of high-density foods. Physiol Behav. 2006;88:597–604. doi: 10.1016/j.physbeh.2006.05.035. [DOI] [PubMed] [Google Scholar]
- 30.Temple JL, Giacomelli AM, Kent KM, Roemmich JN, Epstein LH. Television watching increases motivated responding for food and energy intake in children. Am J Clin Nutr. 2007;85:355–61. doi: 10.1093/ajcn/85.2.355. [DOI] [PubMed] [Google Scholar]
- 31.Herman CP, Polivy J. A boundary model for the regulation of eating. Res Publ Assoc Res Nerv Ment Dis. 1984;62:141–56. [PubMed] [Google Scholar]
- 32.Jansen A, Theunissen N, Slechten K, et al. Overweight children overeat after exposure to food cues. Eat Behav. 2003;4:197–209. doi: 10.1016/S1471-0153(03)00011-4. [DOI] [PubMed] [Google Scholar]
- 33.Shide DJ, Caballero B, Reidelberger R, Rolls BJ. Accurate energy compensation for intragastric and oral nutrients in lean males. Am J Clin Nutr. 1995;61:754–64. doi: 10.1093/ajcn/61.4.754. [DOI] [PubMed] [Google Scholar]
- 34.Epstein LH, Roemmich JN, Stein RI, Paluch RA, Kilanowski CK. The challenge of identifying behavioral alternatives to food: clinic and field studies. Ann Behav Med. 2005;30:201–9. doi: 10.1207/s15324796abm3003_4. [DOI] [PubMed] [Google Scholar]