

Abstract
The aim of this study was to design an information leaflet for patients with paracetamol overdose based on Medicines and Healthcare products Regulatory Agency guidance and to assess its readability. A two-sided one page information leaflet was designed for patients being discharged from hospital after a paracetamol overdose. Patients presenting with an acute paracetamol overdose, irrespective of whether they were treated or not, were recruited to read the leaflet and then answer a brief structured questionnaire based on the leaflet. The readability of the information leaflet was assessed using the Flesch reading ease score. Thirty patients (15 male, 12 female, 3 not recorded; mean age 38 ± 13.0 years) were recruited, wherein 100% of patients reported the language used was understandable, 96.6% knew which symptoms would require urgent medical review after discharge and 100% of patients knew the liver was affected by paracetamol. The Flesch reading ease score was 67.6 (out of a maximum of 100), equivalent to a UK reading age of 10–11years old. Our information leaflet for all patients being discharged after paracetamol overdose was well received by patients, provided them with the required knowledge and had an appropriate reading age based on UK literacy rates. We would recommend that this leaflet could be used as a template on a national level, localized to individual hospitals, to improve patient knowledge of paracetamol toxicity, and facilitate early medical review in the event of deterioration following discharge from the hospital.
Keywords: Paracetamol, overdose, patient safety, outcome
Introduction
Acetylcysteine (NAC) is almost 100% effective in preventing liver damage if given within 8–10 h of ingestion of potentially toxic paracetamol overdose and it is therefore essential that patients who have consumed a toxic dose of paracetamol are identified and treated appropriately (Ferner et al. 2011). The ‘Medicines and Healthcare products Regulatory Agency’ (MHRA) in the UK released new guidance on the management of paracetamol overdose in September of 2012 with their document entitled ‘Paracetamol overdose: new guidance on treatment with intravenous acetylcysteine’ (Commission on Human Medicines 2012). This guidance included recommendations for both the assessment of paracetamol overdose and treatment with NAC (Commission on Human Medicines 2012; TOXBASE).
These recommendations, in particular those concerning the assessment of patients with paracetamol overdose, rely on information provided by the patient to the treating clinician regarding the time and circumstances of the overdose (TOXBASE). Therefore, the MHRA recommended that patients who do not require treatment with NAC should be given an information leaflet highlighting the importance of giving health professionals accurate information regarding the dose and time of ingestion which may prompt a reassessment by the clinician of the requirement for treatment (Commission on Human Medicines 2012). In addition, it was suggested that this leaflet should include information on symptoms which should prompt the patient to re-present for medical review (Commission on Human Medicines 2012). The National Poisons Information Service (NPIS) TOXBASE internet site recommends the use of two separate leaflets depending on whether the patient has received a full course of acetylcysteine treatment or not (TOXBASE).
We designed a single leaflet to be provided to all patients presented with suspected or proven paracetamol overdose, not only to those patients not treated with NAC as recommended by the MHRA. This incorporated the advice and guidance on the content of the advice leaflet not only from the MHRA, but also from the two UK NPIS leaflets (Commission on Human Medicines 2012; TOXBASE). We report here the design of this leaflet, assessment of its readability and a study assessing the patient review of the acceptability of the leaflet.
Methods
Leaflet design
A one page, two sided A4 information leaflet was designed incorporating the recommended advice from the MHRA and NPIS. This leaflet included information on the importance of the patient providing accurate information on the dose and time of their paracetamol ingestion, together with clinical features to be aware of after discharge that should prompt medical review, and local contact information (Fig. 1).
Figure 1.
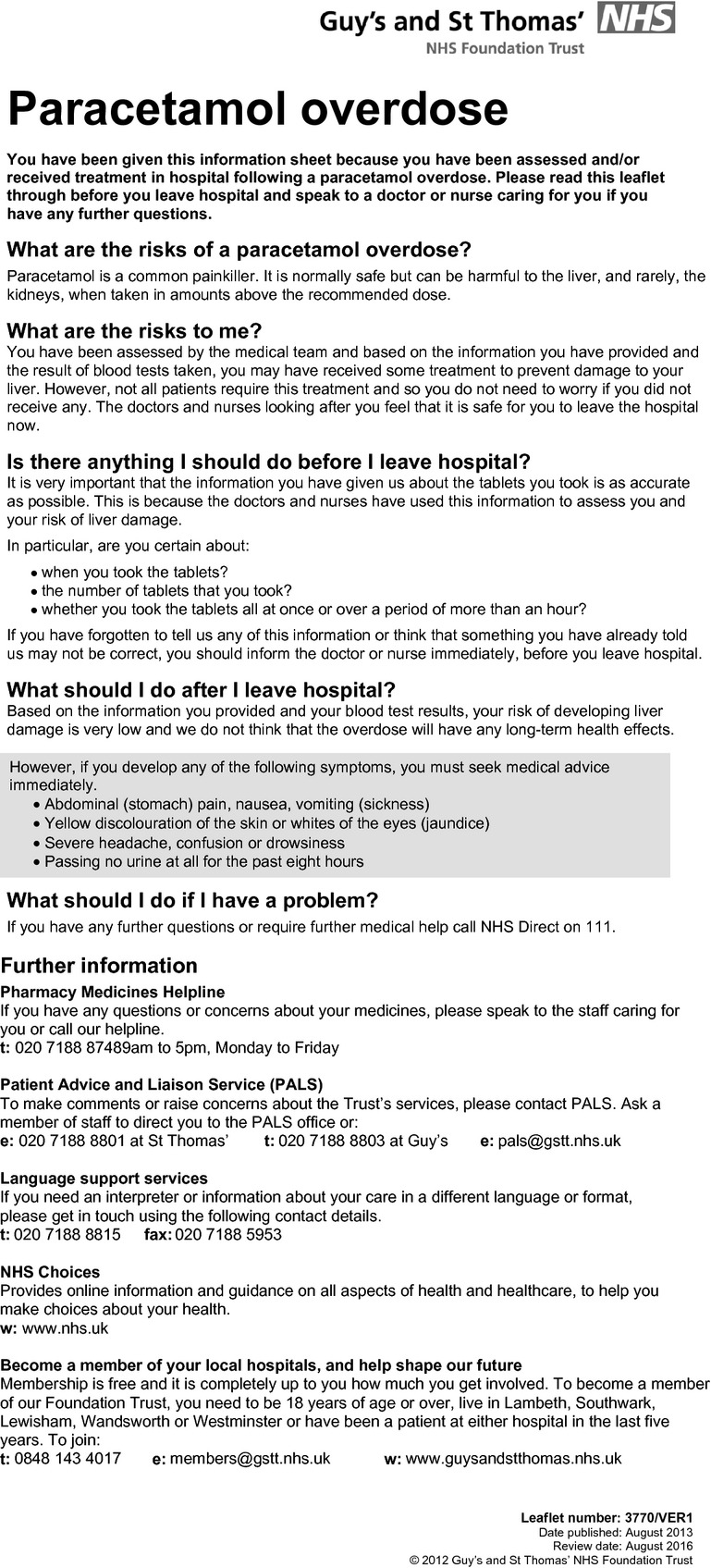
Local patient information leaflet.
Patient review
The leaflet was given to all adult patients who could speak English admitted with both acute single and staggered/supra-therapeutic paracetamol overdose after a decision to discharge was made over a 2-month period. We included those not treated with NAC, those who received a full or extended course of NAC, and those treated with a shortened course of NAC started empirically pending paracetamol concentrations.
Patients were asked to read the leaflet and then self complete a brief structured questionnaire regarding the content of the leaflet. Individuals were not provided with space for free text responses to clarify any of the responses.
The first questions, which were graded by patients as strongly agree, agree, disagree or strongly disagree, on the content were:
I understand why it is important to tell the medical staff exactly what tablets were taken;
I know what symptoms I should watch out for after going home;
I know who to contact if I develop any symptoms; and
The language used in the leaflet was understandable.
To assess understanding of paracetamol-related toxicity after reading the leaflet, patients were asked ‘the organ most affected by paracetamol overdose is the pancreas, liver, heart or lungs.’ Finally, they were asked whether three symptoms would alert them to seeking medical review after discharge: abdominal pain, yellow discolouration of the skin, headache.
Assessment of leaflet readability
We used an adult literacy readability calculator known as the ‘Flesch reading ease score’ and the ‘Flesch–Kincaid grade level’ to calculate the reading ability required to read our leaflet. These are based on formulae which approximate the readability of a document based on sentence length and frequency of polysyllable words. The Flesch reading ease score rates texts on a 100-point scale where the higher the score the easier a document is to understand. The Flesch–Kincaid grade score gives a score equivalent to a US school Grade level – this score can be converted to a UK reading age by adding 5. These formulae are now commonly incorporated into software such as Microsoft Word, and can help guide authors to produce suitable text for their target audience (Special Needs Information Press).
Results
Patient review
Thirty patients (15 male, 12 female, 3 not recorded; mean ± SD age 38 ± 13.0 years) participated in the review of the leaflet.
The patient responses to the questionnaire on the leaflet are shown in Table 1. Overall, it appeared that patients understood why it was important to tell staff exactly what tablets were taken and what to do after going home. Twenty-eight (29 respondents, 96.6% of respondents) patients reported that they knew which symptoms would require urgent medical review. Only one patient disagreed with the statement “I know who to contact if I develop any symptoms.” Interestingly, this patient who reported that they did not know which symptoms to watch out after discharge subsequently responded correctly to questions about the three symptoms requiring urgent medical review; this suggests that in fact they were aware of what symptoms to be aware of after discharge.
Table 1.
Responses from the participants review of the content and acceptability of the patient information leaflet
| Number of respondents | Strongly agree | Agree | Disagree | Strongly disagree | |
|---|---|---|---|---|---|
| 1. I understand why it is important to tell the medical staff exactly what tablets were taken | 30 | 22 | 8 | 0 | 0 |
| 2. I know what symptoms I should watch out for after going home | 29 | 15 | 13 | 1 | 0 |
| 3. I know who to contact if I develop any symptoms | 30 | 8 | 21 | 1 | 0 |
| 4. The language used in the leaflet was understandable | 30 | 15 | 15 | 0 | 0 |
All 30 participants were aware “the organ most affected by paracetamol overdose” was the liver. The responses to the questions about the three symptoms requiring medical review are shown in Table 2.
Table 2.
Responses to three symptoms after discharge mentioned in the patient information leaflet that should prompt medical review
| Specific symptom requiring medical review | Number of responses | True | False |
|---|---|---|---|
| Abdominal pain | 29 | 28 (96.6%) | 1 (3.4%) |
| Yellow discoloration of the skin or eyes | 30 | 29 (96.7%) | 1 (3.3%) |
| Headache | 29 | 22 (75.9%) | 7 (24.1%) |
Assessment of leaflet readability
The Flesch reading ease calculator gave a score of 67.6 which is equivalent to a ‘standard’ reading ability (0–29 very difficult, 30–49 difficult, 50–59 fairly difficult, 60–69 standard, 70–79 fairly easy, 80–89 easy, 90–100 very easy). The Flesch–Kincaid grade level gave a score of 5.7 which approximately equates to a UK reading age of between 10 and 11years old.
Discussion
Following the updated MHRA guidance on the management of paracetamol overdose, we designed a 1 page, 2-sided information leaflet for all patients with reported or suspected paracetamol overdose. The leaflet was generally well received with 100% of patients reporting the language used was understandable and 97% reporting that they knew which symptoms would require urgent medical review. This was reflected by the mostly correct responses to the true–false questions regarding symptoms requiring medical review. Interestingly, 24% of patients felt a headache would not require medical review; in our opinion, most clinicians would consider this is a fairly nonspecific symptom, and that they would therefore not typically mention this symptom to paracetamol overdose patients despite the recommendation by the MHRA (Commission on Human Medicines 2012; TOXBASE).
The Flesch reading ease calculator indicated that our leaflet required a ‘standard’ reading ability, or a reading age of approximately 10 to 11 years old. It is of note, however, that this is an approximate measure of readability based primarily on the word length and the length of sentences. It does not take into account other important factors such as the text size, the layout of written material, and the motivation of the reader. The Flesch score does enable some comparison with other leaflets. Rees et al. (2003) compared 31 patient information leaflets for prostate cancer and found that readability varied considerably with Flesch scores ranging from 35.7 to 68.5. More than 75% had a reading difficulty of “fairly difficult” or “difficult,” and only 23% were classed as ‘standard.’ The authors did highlight that consideration should be given to patient familiarity with certain words rather than relying solely on Flesch scores. The National Literacy Trust estimates that as many as 16% of adults in England are functionally illiterate (defined as having a reading age at or below that expected of an 11-year old) (National Literacy Trust 2014). This should be considered and an appropriate measure of readability used when designing any leaflet, to ensure it is designed to an appropriate reading age/level of literacy. It is reassuring that not only did the Flesch score for our leaflet suggest that it has a reading age around this level, but the study participants reported that our leaflet was understandable.
Patient information leaflets are commonly used in a variety of settings to attempt to improve patient knowledge and subsequently improve health outcomes. While several studies have demonstrated an improvement in knowledge, there are relatively few studies demonstrating their effectiveness (Little et al. 1998; Humphris and Field 2003; Petti and Scully 2007). In patients with acute bronchitis in a primary care setting who did not require antibiotics at their initial consultation but were given a prescription for ‘rescue antibiotics’ and half were given an additional patient information leaflet (Macfarlane et al. 2002). Those who had received the leaflet were less likely to use antibiotics over the next 2 weeks (leaflet 46.2% vs. no leaflet 59.4%). Improving patient education by use of patient information sheets in procedures such as steroid injections and laparoscopy has been shown to improve knowledge about a procedure and its complications and lead to greater post-procedure patient satisfaction, without leading to increased levels of anxiety (Garrud et al. 2001; Coudeyre et al. 2002). We would hope, therefore, that our leaflet would similarly empower patients to represent if they develop symptoms of paracetamol toxicity through improved patient knowledge, without increasing anxiety around discharge.
The limitations of this study are that only a small number of patients were recruited and we excluded non-English speakers. It would be important in regions where a significant number of patients presenting are likely not to be native English speakers, that there should be consideration in producing the leaflet locally in the appropriate language. In addition, this leaflet was designed for use in adult patients only, similar to the advice of the MHRA and NPIS (Commission on Human Medicines 2012; TOXBASE). Further work is required to design a similar leaflet for parents of children presenting with paracetamol overdose.
In conclusion, we have developed a leaflet for patients being discharged from hospital after paracetamol overdose and demonstrated that this is well-received by patients. The reading age required to understand our leaflet that appeared appropriate for the target audience. Our study suggests that it appears to provide patients with appropriate information as suggested in the MHRA guidance. We would recommend that our leaflet be used as a template on a national level, localized to individual hospitals, to improve patient knowledge of paracetamol toxicity, and facilitate early medical review in the event of deterioration following discharge from hospital.
Glossary
- MHRA
Medicines and Healthcare products Regulatory Agency
- NAC
acetylcysteine
- NPIS
National Poisons Information Service
Disclosures
All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
References
- Commission on Human Medicines. 2012. Benefit risk profile of acetylcysteine in the management of paracetamol overdose. Available at http://www.mhra.gov.uk/home/groups/pl-p/documents/drugsafetymessage/con184709.pdf (accessed 1 April 2014)
- Coudeyre E, Poiraudeau S, Revel M, Kahan A, Drapé JL, Ravaud P. Beneficial effects of information leaflets before spinal steroid injection. Joint Bone Spine. 2002;69:597–603. doi: 10.1016/s1297-319x(02)00457-8. [DOI] [PubMed] [Google Scholar]
- Ferner RE, Dear JW, Bateman DN. Management of paracetamol poisoning. BMJ. 2011;342:d2218. doi: 10.1136/bmj.d2218. [DOI] [PubMed] [Google Scholar]
- Garrud P1, Wood M, Stainsby L. Impact of risk information in a patient education leaflet. Patient Educ Couns. 2001;43:301–304. doi: 10.1016/s0738-3991(00)00168-3. [DOI] [PubMed] [Google Scholar]
- Humphris GM, Field EA. The immediate effect on knowledge, attitudes and intentions in primary care attenders of a patient information leaflet: a randomized control trial replication and extension. Br Dent J. 2003;194:683–688. doi: 10.1038/sj.bdj.4810283. [DOI] [PubMed] [Google Scholar]
- Little P, Griffin S, Kelly J, Dickson N, Sadler C. Effect of educational leaflets and questions on knowledge of contraception in women taking the combined contraceptive pill: randomised controlled trial. BMJ. 1998;316:1948–1952. doi: 10.1136/bmj.316.7149.1948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macfarlane J, Holmes W, Gard P, Thornhill D, Macfarlane R, Hubbard R. Reducing antibiotic use for acute bronchitis in primary care: blinded, randomised controlled trial of patient information leaflet. BMJ. 2002;324:91–94. doi: 10.1136/bmj.324.7329.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Literacy Trust. 2014. How many illiterate adults are there in England?. Available at http://www.literacytrust.org.uk/adult_literacy/illiterate_adults_in_england (accessed 1 April 2014)
- Petti S, Scully C. Oral cancer knowledge and awareness: primary and secondary effects of an information leaflet. Oral Oncol. 2007;43:408–415. doi: 10.1016/j.oraloncology.2006.04.010. [DOI] [PubMed] [Google Scholar]
- Rees CE, Ford JE, Sheard CE. Patient information leaflets for prostate cancer: which leaflets should healthcare professionals recommend? Patient Educ Couns. 2003;49:263–272. doi: 10.1016/s0738-3991(02)00188-x. [DOI] [PubMed] [Google Scholar]
- Special Needs Information Press. Readability levels of text – how to find them…. Available at http://www.snip-newsletter.co.uk/pdfs/downloads/readability_briefing.pdf (accessed 1 April 2014)
- TOXBASE. TOXBASE (UK National Poisons Information Service): Paracetamol. Available at http://www.toxbase.org/Poisons-Index-A-Z/P-Products/Paracetamol———/ (accessed 1 April 2014)