

Abstract
Objective:
The ongoing presence of asbestos in products used across workplaces in Canada reinforces the importance of occupational exposure surveillance. This study evaluates the usefulness of the Ontario Asbestos Workers Registry.
Methods:
The study includes 30,829 workers aged 15 to 80 years. Researchers reported on the data quality and analyzed the proportions of workers exposed by industry, and standardized rates by geographic areas and over time.
Results:
The incidence of exposure started to decrease around 1990; but about 2000 workers were still exposed annually until 2006. Results showed large geographical disparities. Unexpectedly, workers from industries other than construction reported exposure.
Conclusions:
The Ontario Asbestos Workers Registry is a useful but challenging source of information for the surveillance of asbestos exposure in Ontario. The registry could benefit from well-defined surveillance objectives, a clear exposure definition, systematic enforcement, regular data analyses, and results dissemination.
Asbestos has been classified by the International Agency for Research on Cancer as carcinogenic to humans,1,2 and it is widely recognized as a cause of mesothelioma (a rare form of cancer that affects cells of the membrane that lines several body cavities), as well as cancers of the lung and larynx in both men and women, and to a lesser extent, ovarian cancer in women.3,4 Workers are subject to numerous carcinogens, including asbestos, in workplaces.5
The health outcomes related to exposure to asbestos occur over the long term, with a latency period of up to 30 years after the exposure has taken place.6 Thus, past and ongoing exposure to asbestos are likely to result in an increasing incidence of related cancers in the coming decades.
The vast majority of asbestos-related cancer cases have occurred as a result of occupational exposure to asbestos. Studies have also demonstrated the presence of high concentrations of asbestos fibers in and around various workplaces,7–11 which have affected the health of people living near those asbestos facilities.12–14
Although the widespread use of asbestos has substantially decreased over time and safety measures have been implemented, workers today are still at risk for being exposed. Currently, the largest number of workers exposed to asbestos in Canada are those from the construction-related industries, where approximately 88% of all workers are from specialty trades and building.15 They are exposed during renovations, maintenance, and demolition of buildings containing asbestos.16,17
For example, the highest asbestos levels ever recorded in a Canadian workplace occurred in the Holmes Caposite plant located in Sarnia, Lambton.10 The second highest was at the Johns-Manville factory in Scarborough, Toronto. Scarborough and Sarnia offer particularly useful case studies for understanding asbestos-manufacturing operations, subsequent health impacts, and asbestos-related policies.
Moreover, the use of asbestos has not been banned in North America, and asbestos is still present in some cement products, floor tiles, friction materials, and textiles used across workplaces in Canada.18
The prevalence of occupational exposure to carcinogens like asbestos and the related health hazards highlight the importance of occupational exposure surveillance, which can provide evidence-based understanding of occupational hazards that builds upon the anecdotal reports of workers.
Surveillance can successfully rely on administrative databases, specifically for chronic conditions.19 For this purpose, data should be systematically collected with an effective case or exposure definition; these should be frequently and consistently analyzed, and the results would need to be periodically disseminated to those who need to know. Another source of information could be exposure registries. There are various registries that aim to assess exposure to occupational hazards. Although surveillance does not constitute their primary objective, these registries could be of great use for monitoring exposure.
In Ontario, the Ontario Asbestos Workers Registry (OAWR) was created in 1986. The Registry originated from an asbestos regulation that was originally filed in 1985 (OReg [Ontario Regulation] 654/85, “Regulation respecting asbestos on construction projects and in buildings and repair operations.” This subsequently became RRO [Revised Regulations of Ontario] 1990 Regulation 838 that established the procedures for the handling of asbestos and placed requirements on building owners to develop an “asbestos control program.” Regulation 838 was revoked and replaced with OReg 278/05 in 2005.)
The OAWR's goal is to collect and store data on workers exposed to asbestos in construction and repair operations.20 This information is used to notify both the worker and his or her physician of the need for a medical examination when the worker has accumulated 2000 hours of exposure (the equivalent of one full year's employment), even though that is not part of the regulation. The registry includes demographic and other personal data, employer and physician details, and the number of occupational asbestos exposure hours as a result of type 2 or type 3 operations (including but not limited to removal, enclosure, breaking, cleaning, or application of asbestos-containing material).18,20 The registry is updated on a weekly basis, and all employers are obligated to report the exposure at least once a year for each eligible worker. The data are submitted to the provincial physician through a completed “Asbestos Work Report” form once within a 12-month period for each worker and when the employment of a worker is terminated. A copy of the form must be given also to the worker. Although there is enforcement of these requirements by the Ministry of Labour (MoL) inspectors, such enforcements are not systematic and therefore not all work sites are visited. Also, no information is collected on the use of personal protective equipment.
The OAWR has the potential to be a relevant source of information for monitoring the occupational exposure to asbestos. Nevertheless, its utility and potential use as a surveillance tool have never been evaluated.
Thus, the primary objective of this study was to evaluate the validity and usefulness of the data contained in the OAWR. This evaluation focused on the face validity of the registry by assessing the data accuracy, the coverage or representativeness, and the accuracy in measuring asbestos exposure. To achieve our primary objective, this evaluation reported on the temporal and geographic variations of the exposure and described the characteristics of workers reporting asbestos exposure in the registry. It also analyzed how these characteristics reflect the intended purpose of the registry to report on exposure to asbestos.
This will help inform managers and public health authorities in their decision-making regarding the surveillance and control of asbestos exposure. The conclusions can help guide decision-making in developing or improving similar registries for other exposures. It will also be useful in informing future projections of asbestos-related cancer incidence.
METHODS
Analytical Approach
This article assessed the face validity of the OAWR by using different criteria, including data accuracy, the coverage or representativeness of the data, and the accuracy in measuring asbestos exposure.
We started with preliminary data validation to assess the accuracy and reliability of the information available and to inform our decision to exclude or derive data. Exclusion criteria were documented, and changes by industry and overtime were also discussed. We then performed descriptive statistics by count, changes over time and by industry. This aimed to evaluate the coverage of the registry, comparing this data to the existing data on companies and the labor force in Ontario. Finally, the accuracy in measuring asbestos exposure was assessed by reporting temporal and geographical distribution of rates of exposure. We made the assumption that if exposure to asbestos is being accurately captured in the registry, we would observe higher rates in specific areas (eg, Lambton) or during earlier years compared with more recent periods (likely a drop in exposure over time resulting from the asbestos regulation). Furthermore, exposure would be more prevalent in certain industries (eg, construction). In addition, to add to the face validity and provide some evidence of the burden of asbestos exposure, we used an ecological analysis linking rates of asbestos exposure to incidence of cancers relevant to that exposure. The underlining hypothesis was that geographical areas with high exposure would likely have higher incidence of specific cancers. To do so, we compared and evaluated the spatial clustering of high levels of exposure to the geographical distribution of mesothelioma.
Analyses were performed with SAS 9.1 (SAS Institute, Cary, NC). The results are discussed in light of the original objective of the OAWR, as well as the general characteristics of surveillance systems.
Data Sources and Study Population
For this study, three data sources were used: (1) The OAWR, (2) Statistics Canada Census data, and (3) Statistics Canada Labour Force Survey data. First, the study included as a primary source, information on individuals working in any asbestos industry in Ontario and who had their exposure reported in the provincial Asbestos Registry maintained by the Ontario MoL. The Asbestos Registry was obtained through a MoL Access to Information request that was filed in 2012.
Second, population data that was relevant to calculating the rates of exposure were obtained through the Statistics Canada census database.21 This included population data by year, age, and sex, and also by local health units. There are a total of 36 local health units/public health units in the province of Ontario.
Third, data on the labor force were used to calculate the rates of workers exposed to asbestos. Labor force survey estimates offer information by sex and by detailed age group. They are calculated annually, based on the “Number of persons who, during the reference week, worked for pay or profit, or performed unpaid family work or had a job but were not at work due to own illness or disability, personal or family responsibilities, labor dispute, vacation, or other reason.”22 The total number of workers is also reported in this database by industry, according to the North American Industry Classification System. The North American Industry Classification System was converted to the Standard Industry Classification–Establishment, which is used by the Asbestos Registry. Industries were classified into 18 groups, according to the 1980 version of the Standard Industry Classification–Establishments.
Measures
Asbestos exposure was measured by the number of workers involved in type 2 or type 3 operations and the number of hours spent in those operations, as recorded in the registry. We estimated the incident exposure, as well as ongoing exposure. Incident exposure included only workers exposed for the first time in a given year, while ongoing exposure traced any worker having a record of exposure during that year.
Crude and standardized rates of exposure were calculated per capita for the population and per workers for the labor force. The rates per capita were standardized by age, using the provincial distribution in 2011 as a reference. The standardization was performed to allow for a comparison between geographic areas and years of exposure.
Standardized incidence rates of mesothelioma from 1986 to 2007 by Health Unit were obtained from Cancer Care Ontario (Ontario Cancer Registry, 2011) and are age-standardized to the 1991 Canadian population. Other variables reported in the study included workers' demographics (age and sex), as well as local health units (public health unit) and industry type of the employers.
RESULTS
Evaluation of Data Accuracy
For each record, we explored the concordance between the different dates in the registry (birth dates, start and end dates of employment) and checked the correctness and completeness of age, the number of hours reported, industry names, and postal codes. Table 1 summarizes the proportion of entries with inconsistent or unexpected data by period of exposure.
TABLE 1.
Proportion of Inconsistent or Unexpected Data by Period (Reported Start Date)
| Before 1986 | 1986–2000 | After 2000 | ||
|---|---|---|---|---|
| (n = 6,132) | (n = 55,549) | (n = 25,350) | Total | |
| Birth dates ≥ start date or ≥ end date of employment | 415 (6.8) | 1,609 (2.9) | 0 (—) | 2,024 (2.3) |
| Ages <15 yrs | 447 (7.3) | 2,098 (3.8) | 419 (1.6) | 2,964 (3.4) |
| Workdays <1 (end date ≤ start date) | 3,430 (55.9) | 1,614 (2.9) | 309 (1.2) | 5,353 (6.1) |
| 0 hr reported | 0 (—) | 26 (0.05) | 185 (0.7) | 211 (0.2) |
| Worked >16 hr/d | 2,748 (44.8) | 974 (1.7) | 99 (0.4) | 3,821 (4.4) |
| Records covering more than 12 mo | 1,692 (27.6) | 11,107 (20.0) | 4,844 (19.1) | 17,646 (20.3) |
| Records covering more than 18 mo | 1,197 (19.5) | 1,989 (3.5) | 521 (2.1) | 3,710 (4.3) |
| Nonconstruction sectors or unknown | 2,724 (44.4) | 18,611 (33.5) | 6,048 (23.8) | 27,383 (31.5) |
Regarding the organizations' names and industry type, there were some instances of multiples or missing names, some changes in names over time, and some discordance between individuals' and organizations' files. Information was reconciled and unique names assigned when needed. A Google search helped in making some decisions for both names and industry categories. Using this information, a single primary industry was also assigned to each worker. We were unable to assign an industry to 186 organizations of the 976 (accounting for 6888 entries, ie, 7.8% of all entries) in the registry. Also, 113 organizations and 4193 entries (4.8%) had a missing postal code.
We cross-validated birth dates against the employment start and end date. We found 2.3% of the entries with birth dates greater than or equal to start or end date (ie, age less or equal to zero), mostly among exposure reported before 1986. There were also people with very young ages in the registry and a few entries had 0 hours of exposure reported. The number of hours reported was also compared with the work duration (estimated from employment dates). Some records had one or less workdays, and yet reported a substantial number of hours worked in type 2 or type 3 operations, mostly 2001 hours (which represents the cutoff for the provincial lead to take action). This happened more frequently before 1986, and the proportion of these inconsistencies decreased over time. Furthermore, even with reasonable duration of employment, we found some unrealistic numbers of hours reported per day (eg, an average of more than 16 hours to more than 24 hours a day). Once again, these inconsistencies appeared more frequently during earlier periods of exposure (44.8% before 1986 vs 0.6% after 2000).
Finally, the reported duration between start and end date of employment reached 50 years. This explained the presence of records with employment before 1986. For the most recent years, records were most often related to exposure within a 12- to 18-month period; 19.5% of exposure reported before 1986 covered more than 18 months compared with 3.5% and 2.1% of entries from 1986 to 2000 and after 2000, respectively. It seems that in the first year of operation of the registry, people took the opportunity to record all known past exposure. Nevertheless, 95.7% of all records were related to employment within 1.5 years and 79.7% within 12 months. We used the starting date of work as our reference date for subsequent analyses.
In summary, the original sample comprised more than 87,000 entries for a total of 33,011 workers who were exposed from 1934 to June 2012. We excluded entries with ages less than (but not equal to) 15 years and those with more than 84 years, as well as null number of hours. In addition, if the reported number of hours exceeded 16 hours per day, this was considered inaccurate and the reason for excluding those hours when analyzing duration of exposure. Apart from missing postal codes, addresses outside of Ontario (2.5% of the records) were also excluded from the analyses of geographic variations.
The final sample for subsequent analyses included 30,829 workers aged between 15 and 80 years (no one was 80 to 84 years old), who reported an exposure to asbestos from 1934 to June 2012. Approximately 10% of all entries in the final sample included exposure information before 1986 (when the registry started). We also observed some peaks in the numbers of workers and hours worked during the years 1987 and 1989. An examination of the data revealed that a high level of reporting occurred from Boards of Education around 1989. Table 2 gives some examples of companies with variable number of workers and hours from year to year from 1987 to 1989. There were in total 3306 entries from Boards of Education, of which 1556 were recorded in 1989 only (representing 76.6% of the hours and 22.4% of all entries in the registry for that year). Nevertheless, the peak in reported hours in 1987 was not explained by reporting from the School or Education Boards but rather by unknown asbestos organizations. There were a total of 1135 entries from companies categorized as unknown asbestos organizations, and 63.5% of these entries were recorded for a starting date in 1987 only (representing 15.1% of entries and 74% of hours in that year). In summary, trends over time, particularly in the number of hours, look somewhat more consistent when the Boards of Education and unknown organizations are excluded (Fig. 1).
TABLE 2.
Example of Data Inconsistency
| 1987 | 1988 | 1989 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| People (With | People (With | People (With | |||||||
| Organizations | People, n | Valid Hours), n | Hours | People, n | Valid Hours), n | Hours | People, n | Valid Hours), n | Hours |
| Insurance company #1 | 2 | 2 | 25,463 | ||||||
| Utilities company #2 | 12 | 12 | 1,386 | ||||||
| Asbestos company #3 | 341 | 338 | 29,550 | 49 | 49 | 2,804 | 751 | 728 | 48,908 |
| Board of education #4 | 6 | 6 | 12,000 | ||||||
| Board of education #5 | 9 | 9 | 184 | 8 | 8 | 50 | 2 | 2 | 6 |
| Construction company #6 | 13 | 13 | 5,429 | 12 | 12 | 1,611 | 24 | 23 | 2,569 |
| School board #7 | 23 | 23 | 6,853 | 60 | 60 | 49,445 | 189 | 189 | 338,664 |
| Utilities company #8 | 6 | 6 | 2,080 | 1 | 1 | 400 | |||
| University #9 | 258 | 258 | 6,745 | ||||||
| Government service #10 | 14 | 14 | 14,000 | ||||||
| Construction company #11 | 35 | 35 | 1,588 | ||||||
| Construction company #12 | 86 | 83 | 8,187 | 64 | 64 | 6,880 | |||
| Construction company #13 | 383 | 343 | 32,128 | ||||||
| Construction company #14 | 3 | 3 | 6,003 | 43 | 43 | 1,928 | |||
| Manufacturing company #15 | 19 | 19 | 3,251 | 3 | 3 | 300 | 96 | 96 | 6,941 |
| Manufacturing company #16 | 29 | 29 | 3,100 | 20 | 20 | 598 | 31 | 31 | 2,289 |
| Board of education #17 | 686 | 685 | 1,370,000 | ||||||
| University #18 | 55 | 55 | 1,149 | 32 | 32 | 449 | 40 | 40 | 580 |
| Asbestos company #19 | 15 | 15 | 1,977 | ||||||
| Board of education #20 | 13 | 13 | 10,564 | 1 | 1 | 13 | 1 | 1 | 325 |
| Board of education #21 | 10 | 10 | 20,000 | ||||||
| Utilities company #22 | 13 | 13 | 1,872 | ||||||
| Construction company #23 | 14 | 14 | 4,813 | 56 | 56 | 16,399 | |||
| Percentage of Grand Total | |||||||||
| All schools | 2.8 | 2.9 | 5.0 | 2.1 | 2.1 | 11.9 | 19.9 | 20.1 | 70.2 |
| 14 most common companies (excluding schools) | 25.8 | 25.2 | 25.3 | 2.0 | 2.1 | 2.4 | 18.4 | 18.2 | 4.5 |
| Grand total | 3,563 | 3,466 | 375,639 | 4,860 | 4,738 | 421,282 | 6,000 | 5,926 | 2,491,571 |
FIGURE 1.

The number of entries and hours by year and type of organizations.
Coverage or Representativeness of the Registry
As of 2012, the registry included up to 976 companies, mostly from the city of Toronto health unit. The eastern region has many asbestos companies, yet there were only 11 organizations in the registry from this region—this is an indication of underreporting. A total of 474 companies were primarily from the construction sector; while for more than 600, construction was the primary or secondary sector. In some cases, we found a few entries before the date of creation of some companies or more workers in the registry than their estimated workforce. In other cases, no record was provided for consecutive years of operation or there were inconsistencies or gaps in reporting over time.
We identified 36 asbestos removal services companies in Ontario.23 Of these 36 companies, only 12 were present in the registry and even those did not provide an exhaustive report of their workers' exposure. For example, while one asbestos-specialized company registered 114 of its 125 employees for a given year (91% of the eligible people), another company recorded zero of their 10 employees. Very few asbestos organizations have reported consistently over the observed period; in most cases, we observed a sporadic reporting regardless of the numbers of employees.
It was challenging to assess the proportion of eligible companies reporting in the registry because of the difficulty in obtaining an accurate denominator of the number of construction companies in Ontario eligible to report their exposed workers in the registry. There are currently approximately 1200 companies registered as members of the Toronto Construction Association; however, this list is incomplete because it does not include the nonmembers and the different trades that may also be working with asbestos. As an alternative, we used the number of workers in the labor force by industry and estimated the number of workers in the registry as a fraction of the total number of workers in the labor force, namely for the construction sector. As expected, the registry had a higher proportion of the labor force in construction than that in other sectors (Fig. 2). From 1986 to 2011, an average of 144 workers per 100,000 (46 to 230) in the construction industry labor force were annually reported in the registry, which is almost 10 times higher than the exposure in others industries. Even though the registry was developed for the construction sector, we found entries from many other sectors, the highest rates being in the manufacturing and educational service industries. The average annual rates were 18 per 100,000 in the manufacturing industry, 16.7 and 5.5 per 100,000, respectively, in educational and government services, and 3.5 per 100,000 in the mining sector. There were less than 1.5 entries per 100,000 workers in all other industries. Finally, most workers registered were men (96%), adding to the face validity of the registry, because the construction sector is mostly composed of men.
FIGURE 2.
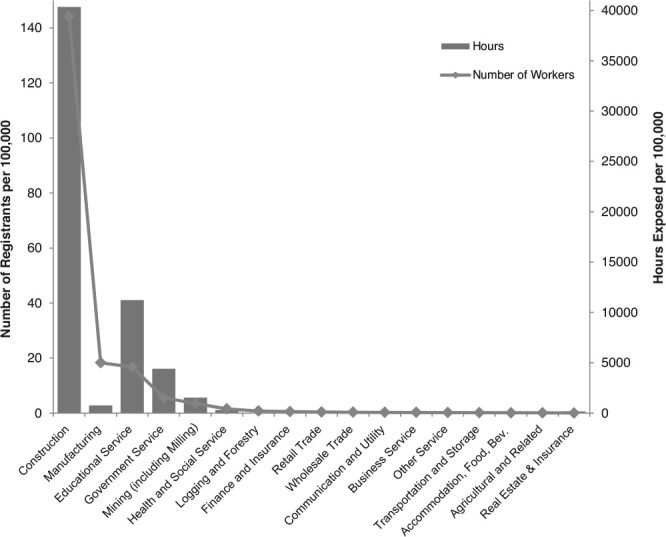
Average annual rate of exposure by industry type, 1986–2011.
Accuracy in Measuring Asbestos Exposure
We evaluated whether the prevalence and incidence of exposure to asbestos, as measured by the registry, corresponded to the assumptions of temporal and geographical variations. Also, we measured the ecological association between the exposure and rates of mesothelioma.
Prevalence and Incidence of Exposure (Number of Workers Exposed) by Year
Between 1986 and June 2012, there were 26,704 workers newly exposed to asbestos. The incidence of exposure started to decrease around 1990, but there remained about 2000 workers exposed each year until 2006. The proportion of new workers exposed to asbestos decreased over time. In 2011, a total of 263 new workers were reported compared with 1447 in 1986. This represented 37.1% of new people exposed that year compared with 84.6% in 1986. As for the prevalence of exposure, in 1986, 29.7 per 100,000 workers in Ontario were exposed to asbestos. In 1989, this proportion reached 70 per 100,000, then dropped to 20.5 per 100,000 in 2005, and 9.9 per 100,000 in 2011 (Fig. 3).
FIGURE 3.
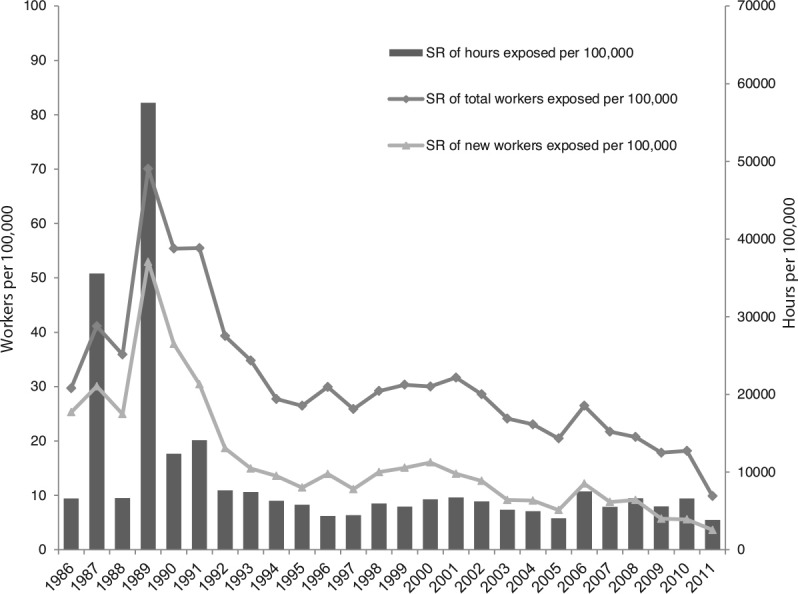
Standardized rates (standardized by age and sex distribution of 2011 labor force in Ontario) of exposure by current and first date of employment per 100,000 workers. SR, standardized rate.
The trends for ongoing asbestos exposure by industry type are similar to the overall trend for most sectors, with a decrease around 1990. Nevertheless, the rates of exposure remained at high levels until 2006 in the construction industry, while there was a dramatic drop in the mining industry around 1990 (not shown). This could be a reflection of mines closure and potentially an indication of more rigor in data collection targeting construction industry.
The number of hours of exposure showed some variations over time. It was at its maximum in 1987 and 1989, then dropped substantially after 1991 (Fig. 3). Nevertheless, as previously reported, the peaks in 1987 and 1989 are the reflection of unexpected reporting by Boards of Education, specifically from Lambton County. An analysis of the trends without data from the Boards of Education did not reveal peaks but confirmed the decreasing trend over time. Specifically, when considering records from only the construction sector, we observed a more consistent decrease over time with no striking peak (Fig. 4).
FIGURE 4.
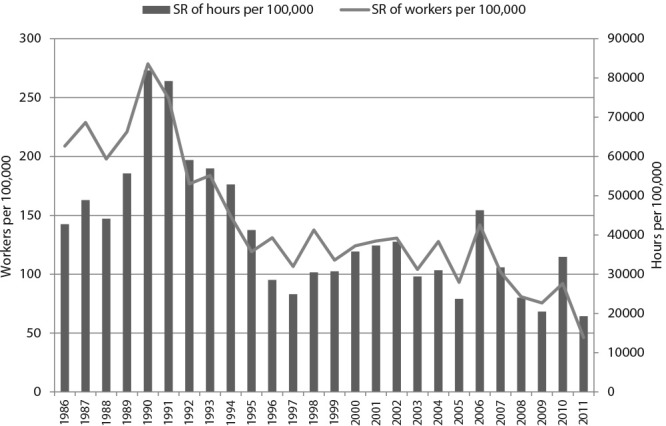
Standardized rates (standardized by age and sex distribution of 2011 labor force in Ontario) of exposure by current year of employment per 100,000 workers in the construction industry. SR, standardized rate.
Geographical Variations of Exposure
Overall, the age-standardized incidence of exposure from 1986 to 2012 varied significantly from 4.7 per 100,000 in Leeds, Grenville, and Lanark District Health Unit to as high as 2954.4 per 100,000 capita in Lambton Health Unit (Fig. 5).
FIGURE 5.
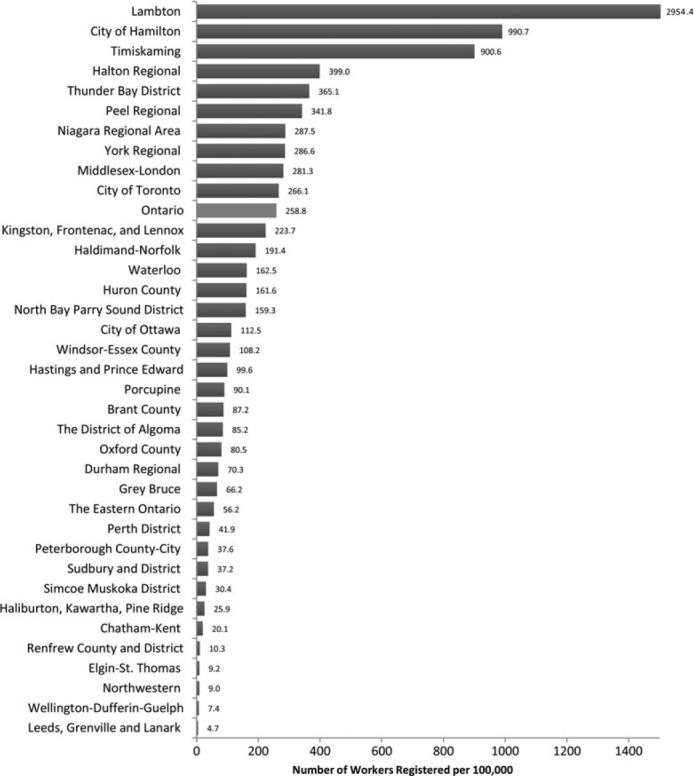
Age-standardized incidence rates of exposure per 100,000 capita by public health unit, 1986–2012.
We also observed significant geographic variations by year, in both the age-standardized incidence and ongoing rates of exposure. The temporal trends by local health units depended upon the health unit. There was a decrease over the years in the incidence of exposure to asbestos for most regions, except for the Lambton Health Unit where the exposure continued to reach high levels until 2008. As expected, the Lambton Health Unit showed the highest level of reporting of asbestos exposure over time.
Ecological Distribution of Asbestos Exposure and Health Outcomes
Mesothelioma, which is mainly caused by asbestos, shows some geographical variations in the incidence rates for Ontario. Thus, it was relevant to evaluate whether such variations aligned with those observed in the distribution of the exposure to asbestos. We found that the highest rates of mesothelioma were observed in regions that exhibited the highest rates of workers exposed to asbestos, such as the Lambton County Health Unit and the Hamilton Health Unit. Nevertheless, the Northwestern Health Unit and some of the eastern health units (Eastern, Leeds, and Haliburton) exhibited high rates of mesothelioma cancer although they are among the places that reported the fewest numbers of workers exposed.
A Public Health Concern
It is noteworthy that although fewer women were exposed, they accumulated, on average, more hours of exposure than men. Fifty percent of women exposed had more than 346 hours of exposure compared with 86 hours among men. The average number of hours of exposure among women was almost twice the male average. The most frequent age group at first exposure was 25 to 34 years for both men (29.5%) and women (25.6%). These workers would be aged 50 or 60 years, and there is now a likelihood of them developing cancers.
After 2010, 22 of the 36 health units did not have any new workers exposed to asbestos. In regard to ongoing exposure, most regions had a low level, which has remained stable over time. Nevertheless, in a few health units, including Lambton, Hamilton, and Timiskaming, there has been substantial variation and high levels of exposure until recently. Unlike almost all other regions, Kingston showed an ongoing increase in exposure to asbestos over the years since 1986. Also of concern is that there has been a peak in exposure in recent years in Huron County Health Unit.
DISCUSSION
This first validation of the OAWR suggests that it could be useful for surveillance of asbestos exposure if some key issues are corrected. The original intent of the OAWR was to collect data that could be analyzed for trends and geographical variations. The results have demonstrated the usefulness of the OAWR despite some issues with the data quality and missing or incomplete information. The registry has the ability to identify at least some of the workers exposed to asbestos in Ontario. The data allows for an analysis of the distribution of exposure by workers' characteristics, years of exposure, geographical regions, and industry. As required for a surveillance tool, the OAWR has been collecting exposure data on workers over many years. It provides a large sample of the population of workers exposed. There were more than 600 organizations and more than 10,000 workers included from the construction sector over the 25 years of study. Nevertheless, the observed patterns by organization corresponded to irregular contract jobs, regardless of the number of employees or the number of hours. Also, there was no pattern in reporting by organization size (estimated by the total number of entries in the registry), and most of the nonconstruction companies reported more irregularly over the 25-year period. Because the reports are mandatory for the construction sector (only), this could contribute to the success of using this registry for the purposes of surveillance among this industry group specifically. In fact, the registry included a larger proportion of workers from the construction sector than from any other industry.
Although the registry's focus was on the construction sector and captured more workers from this sector, we also found an elevated risk of being exposed among workers from the manufacturing industries and educational services. The peak that was observed, particularly among the Boards of Education, could be the result of either a blitz of inspections by the MoL because of the implementation of regulation 654/85 in 1985 or because of renovations performed at that time in the schools. This could reflect either the true level of exposure or an overreporting by the boards. Although construction, mining, and manufacturing sites, known to have high exposures, are either closing or are regulated, the registry highlights the need to focus on those sectors with less-apparent exposure, including educational service, government, and health and social science industries.
Moving Forward With Registry Design and Implementation
The original intent of the OAWR was to register workers from the construction sector, and we found that most workers are in fact from this industry. Nevertheless, it seems that the registry has expanded beyond its initial intended purpose because we found entries from other industries. Although these industries are not coded as construction, the specific occupation/job task might be related to construction, for example, a civil engineer working and registered in the telecommunication industry. Nevertheless, we did not have adequate information on workers' occupation to make this presumption. Hence, it would be beneficial to have some fixed criteria for including entries in the registry, or space to include more occupational information in the registry.
In order for the OAWR to be a satisfactory surveillance tool, the registry needs to ensure better data quality and representativeness of the sample. It needs to undergo frequent analysis of the data and the results need to be disseminated. The provincial physician in charge of the registry at the MoL could play an important role in championing this work. Until these steps are taken, the registry cannot be used for policy-level decision-making.
Specificity and positive predictive value constitutes key characteristics of any surveillance tool. To achieve high levels of these characteristics, the registry should specify a clear definition of the intensity as well as the duration of the exposure being measured. It would also be beneficial to have a process whereby data are validated upon receipt of the completed forms. Basic quality control regarding dates of employment and the numbers of hours would contribute to improved data quality. Accurate and valid information regarding the location of exposure or the worker's sector of occupation is also needed. It would be useful if both head offices and worksite locations were reported for each exposure. Currently, all workers are included regardless of the number of hours that they were exposed to asbestos, their specific occupation, or their place of work. This approach has allowed the inclusion of as many workers as possible. Nevertheless, this has introduced errors and a lack of specificity, as we found in our analysis.
Moreover, the data were not representative of all potentially exposed workers, which may have resulted in biased estimates of the prevalence of workers exposed. For example, there were only a few organizations in the registry from the eastern region of Ontario, which is known for having many asbestos facilities. Unfortunately, we were also limited in our ability to fully explore the reporting patterns of all eligible construction companies in Ontario because of the lack of data. Organizations were not consistently reporting every year, and even when they did report, there were substantial differences in the number of entries by year. Also, although employers are requested to report exposure once in each 12-month period (or at the end of employment, which could be less than a year), we counted some records covering more than 1 year. Logically, a report could overlap two fiscal years because it covers a 12-month period, but should not exceed 12 months. For exposure reported in earlier years, entries covered much longer periods of employment, justifying the presence of historic exposures before the implementation of the system in 1986. We also counted some entries from unknown organizations, but there was no unknown organization reporting data after 1990, suggesting a better management/control of data quality. Systematic enforcement would help ensure that the sample obtained is representative of the population of interest.
About the Registry Face Validity
There was a decline observed around 1990 in both the number of workers and the number of hours exposed. This observation corresponds to a multitude of events and circumstances regarding asbestos exposure. For instance, during the mid-1980s, as the public became more aware of the fatal health risks of asbestos, asbestos exposure became an important public health issue and of political interest in most countries producing or using asbestos. This was also true in Ontario, providing the impetus for establishing the Ontario Royal Commission on Asbestos. The Commission's report, tabled in 1984, recommended that the use of crocidolite and amosite asbestos be “prohibited indefinitely” in the province and that chrysotile be banned from textile manufacturing.24 Furthermore, the Commission specifically recommended that changes be made to the Workers' Compensation Act so that both asbestosis and mesothelioma would be classified as “irrefutable.”24 In 1992, mesothelioma and asbestosis were given Schedule 4 designations, which provided an irrefutable presumption of the work-relatedness of the diseases and mandated automatic compensation.25,26 During this same period of time, many asbestos mines were closed in Canada (the last active mine was closed in 2013).
Like the temporal trends, geographical patterns that emerge from the data in the OAWR met expectations, apart from a few exceptions. The two highest rates of exposure to asbestos were unsurprisingly observed in Lambton and the city of Hamilton health units. Industry in Sarnia is dominated by both large consumers and producers of asbestos.27 Asbestos was also an integral component of the production in all three of Sarnia's Holmes Foundry and Insulation factories.
Likewise, in Hamilton, manufacturing has been traditionally the biggest employer. The major steel companies in Canada (Stelco and Dofasco) were established in Hamilton and have provided the market with appliances, automobiles, and houses since 1945.28 Different asbestos-containing materials were used in both the construction of the plants before 1980s, and the production process (eg, parts of the ovens were constructed from chrysotile asbestos). Also, the workers' protective clothing against fire or excessive heat was made from asbestos.29 The construction sector, including the conversion of old buildings into residential apartments, has also recently grown significantly in the area.
To confirm the face validity, we conducted an exploratory ecological analysis linking exposure to health burden at the regional level. Nevertheless, it was not possible to find a definite link, probably because of the limitations in both the methods and the data quality. First, it was not possible to perform an association analysis at the individual level. Also, the attribution of place of exposure to individual workers is not completely accurate in the Asbestos Registry. Considering worker mobility, the designated place of incidence of cancer is not necessarily the place where the workers were exposed. Nevertheless, the Lambton and Hamilton Health Units, which have the two highest exposure rates to asbestos, exhibit the highest rates of mesothelioma, supporting the use of geographical analyses. In fact, exposure to asbestos in the Holmes facilities in Sarnia is largely responsible for the fact that Lambton currently has the highest rates of pleural mesothelioma in Ontario.30
There could be many other reasons for the discrepancies between regions with high rates of mesothelioma yet low numbers of workers exposed. First, there could be an underreporting of the exposure. In fact, there are many known asbestos facilities in the eastern region of Ontario, yet these regions showed low rates of exposure. Second, peripheral exposure to asbestos could also explain the higher rates of cancers. Because the OAWR includes only employed workers, it would be of interest to determine whether some of the men with mesothelioma did not work in asbestos facilities or whether they were self-employed, thus not reporting to the registry. Third, the reported cancers could originate from exposures in places other than the place of diagnosis, given that seasonal workers most often travel to work out of their place of residence.
Finally, since the exposure to asbestos was assessed from 1986, and given the average latency period of 30 years, we could not expect a strong association with incidence rates of cancer reported for mesothelioma and asbestos-related lung cancer before 2012. Thus, the rates of cancers around 2016 might be more relevant to this cohort, and we might expect to see an increasing incidence of related cancers over the next few decades, especially for regions or industries with higher asbestos exposure.
If the design and implementation of the registry are improved to encompass the qualities outlined in the previous sections, we believe that the methodological issues we faced would be largely resolved for a better use of the data.
Public Health Utility
The analysis revealed some differences in worker characteristics and industries, mostly in the expected directions. Men and young adults (25 to 34 years old), who constitute the greatest portion of the workforce, were more likely to be exposed to asbestos. Because of the latency period between asbestos exposure and disease onset, workers with exposures reported in 1986 in the registry will only now be contributing to the public health burden.
Unexpectedly, women tended to be exposed at older ages and accumulated, on average, more hours of exposure. Unlike men, a higher proportion of female workers were found in the health and social science industries, accommodation, food and beverage service, as well as the educational service industries. One explanation for this may be that more women are working in industries requiring longer shifts and, thus, are accumulating more hours of exposure. It is also plausible that women in occupations such as education would consider themselves continuously exposed during their workday (ie, 8-hour shifts of working in a building with asbestos) as opposed to men in occupations such as construction who would consider themselves sporadically exposed during their workday (ie, the sum of 2 hours over the workday when they worked directly with a product).
Our results have shown that exposure to asbestos in Ontario, despite having declined over the years, remains a matter of concern. In 2011, almost 10 per 100,000 workers were still being exposed to asbestos in the province, and this included 263 people who were newly exposed that year. This is likely an underestimation because of the limitations we have described in previous sections. In addition, existing materials that contain asbestos are being disturbed during construction and renovation, which continues to put workers at risk of exposure.
In addition, the recent exposures and the peaks in exposure that were noted in Kingston and Huron County raise some concerns. These areas have had relatively low levels of exposure to asbestos until recently. This increase might be linked to new or ongoing renovations or demolition projects of old buildings. There is a need to monitor exposure to asbestos everywhere but particularly in those regions with rising exposure.
CONCLUSION
In summary, this is the first evaluation of the OAWR or analysis of its data since its creation. Such an evaluation is necessary to enable the registry to be considered for use as a surveillance tool. This first evaluation provides some interesting results and demonstrates the relevance of frequent and consistent analysis of the data and dissemination of the results. The dissemination of this analysis could contribute to raise public awareness and help inform decision-making about exposure to asbestos and could be useful when determining workers' compensation.
This analysis is already making an impact on enforcement practices at the MoL. As part of the strategy to protect workers' health and safety on the job, MoL inspectors check that asbestos operations are conducted in accordance to regulation. Because of preliminary results of this study that have been disseminated to the MoL, inspectors will now also address asbestos worker registry reporting requirements.
As mentioned by Collegium Ramazzini, who has called for a universal ban on asbestos, “there is no safe level of exposure to asbestos” and “the so-called ‘controlled use’ of asbestos is a fallacy”.31(pp202–204) Also, despite the closure of major asbestos sites, there are operations and workplaces where exposure to asbestos still occurs. This underlines the need to monitor and evaluate any potential exposure to asbestos. The Ontario Asbestos Registry is a useful source of information of asbestos exposure, providing not only insights but also challenges for the interpretation of the levels of exposure in Ontario. The geographical and temporal trends should be continuously monitored, and this is possible only if the registry continues to actively collect information. This study revealed some limitations relating to how information is collected for the Ontario Asbestos Registry, which if addressed, would increase the relevance of the registry for surveillance purposes.
This research initiates conversations on whether or not the trends and geographic variations depicted are meaningful. Further work needs to be conducted to ascertain the temporal and spatial trends in asbestos exposure, as well as the distribution by industry, using this data source.
The results support the advocacy work for the elimination of asbestos exposure. It provides some useful evidence that a substantial number of workers have been exposed to asbestos for decades and may ultimately die of asbestos-related cancer.
Footnotes
This work has not received funding from any organizations mentioned. Dr Genesove is however the provincial physician in charge of the Ontario Asbestos Workers Registry.
The authors declare no conflicts of interest.
REFERENCES
- 1.IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. IARC monographs on the evaluation of carcinogenic risks to humans. A Review of Human Carcinogens: Metals, Arsenic, Fibres, and Dusts; vol 100 (c). Lyon: International Agency for Research on Cancer; 2012: v–vii, 1–412. [Google Scholar]
- 2.Institute of Medicine of the National Academy of Science. Asbestos: Selected Cancers. Committee on Asbestos: Selected Health Effects Board on Population Health and Public Health Practices. Washington, DC: The National Academies Press; 2006 [Google Scholar]
- 3.Cancer Care Ontario; Candido E, Theis B, Marrett L, Navaranjan G, Del Bianco A, Demers PA. Cancer Risk Factors in Ontario: Evidence Summary. Toronto, ON; Cancer Care Ontario; 2013 [Google Scholar]
- 4.Carex Canada. Occupational exposure estimates: asbestos. Available at http://www.carexcanada.ca/en/asbestos/occupational_exposure_estimates/phase_2/ Published 2011. Accessed February 13, 2013.
- 5.Siemiatycki J, Richardson L, Straif K, et al. Listing occupational carcinogens. Environ Health Perspect. 2004;112:1447–1459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kirkham TL, Koehoorn MW, McLeod CB, Demers PA. Surveillance of mesothelioma and workers' compensation in British Columbia, Canada. Occup Environ Med. 2011;68:30–35 [DOI] [PubMed] [Google Scholar]
- 7.Williams PR, Phelka AD, Paustenbach DJ. A review of historical exposures to asbestos among skilled craftsmen (1940–2006). J Toxicol Environ Health B Crit Rev. 2007;10:319–377 [DOI] [PubMed] [Google Scholar]
- 8.Phanprasit W, Sujirarat D, Musigapong P, Sripaiboonkij P, Chaikittiporn C. Asbestos exposure among mitering workers. Saf Health Work. 2012;3:235–240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brunner WM, Williams AN, Bender AP. Investigation of exposures to commercial asbestos in northeastern Minnesota iron miners who developed mesothelioma. Regul Toxicol Pharmacol. 2008;52(suppl):S116–S120 [DOI] [PubMed] [Google Scholar]
- 10.Brophy J, Parent M. Documenting the asbestos story in Sarnia. New Solut. 1999;9:297–316 [DOI] [PubMed] [Google Scholar]
- 11.Liu P. Carcinogens in the Workplace: A Short History of Occupational Cancer Research in Ontario (1950–2010). Toronto, ON: Cancer Care Ontario; 2011 [Google Scholar]
- 12.Reid A, Heyworth J, de Klerk N, Musk AW. The mortality of women exposed environmentally and domestically to blue asbestos at Wittenoom, Western Australia. Occup Environ Med. 2008;65:743–749 [DOI] [PubMed] [Google Scholar]
- 13.Reid A, Segal A, Heyworth JS, de Klerk NH, Musk AW. Gynecologic and breast cancers in women after exposure to blue asbestos at Wittenoom. Cancer Epidemiol Biomarkers Prev. 2009;18:140–147 [DOI] [PubMed] [Google Scholar]
- 14.Ferrante D, Bertolotti M, Todesco A, Mirabelli D, Terracini B, Magnani C. Cancer mortality and incidence of mesothelioma in a cohort of wives of asbestos workers in Casale Monferrato, Italy. Environ Health Perspect. 2007;115:1401–1405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Carex Canada. Occupational exposure estimates: asbestos. Available at http://www.carexcanada.ca/en/asbestos/occupational_exposure_estimates/phase_2/ Published 2011. Accessed February 13, 2013.
- 16.Sharpe A, Hardt J. Five Deaths a Day: Workplace Fatalities in Canada, 1993–2005. Ottawa, ON: Centre for the Study of Living Standards; 2006 [Google Scholar]
- 17.Marrett LD, Ellison LF, Dryer D. Canadian cancer statistics at a glance: mesothelioma. Can Med Assoc J. 2008;178:677–678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ministry of Labour. A guide to the regulation respecting asbestos on construction projects and in buildings and repair operations. Available at http://www.labour.gov.on.ca/english/hs/pdf/asbestos_guide.pdf Published 2011. Accessed February 2013.
- 19.Kone Pefoyo AJ, Rivard M, Laurier C. Revue d'epidemiologie et de sante publique. [Public health surveillance and role of administrative data]. 2009;57:99–111 Importance de la surveillance en sante publique et utilite des donnees administratives. [DOI] [PubMed] [Google Scholar]
- 20.Ministry of Labour. Asbestos Workers Registry [Administrative Data]. Toronto, ON: Provincial Physician, Ontario Ministry of Labour; 2004. Available at http://ophid.scholarsportal.info/details/view.html?q=ray&uri=/phirn/awr_PHIRN_E.xml [Google Scholar]
- 21.Statistics Canada. Table 051-0032—Estimates of population, by age group and sex, census divisions and census metropolitan areas (component method), 1991 census boundaries, annual (persons unless otherwise noted), CANSIM (database). Available at http://www5.statcan.gc.ca/cansim/a05 Accessed January 21, 2013.
- 22.Table 282-0002—Labour force survey estimates (LFS), by sex and detailed age group, annual (persons unless otherwise noted), CANSIM (database). Available at http://www5.statcan.gc.ca/cansim/a26
- 23.Manta Media Inc. 36 asbestos removal services companies in Ontario, Canada [database]. Available at http://www.manta.com/world/North+America/Canada/Ontario/asbestos_removal_services–E031F0M9/ Published 2013. Accessed September 26, 2013.
- 24.Dupre S, Mustard J, Uffen R. Report of the Royal Commission on Matters of Health and Safety From the Use of Asbestos in Ontario. Toronto, ON: Ontario Ministry of the Attorney General; 1984 [Google Scholar]
- 25.Brophy JT, Keith MM, Schieman J. Canada's asbestos legacy at home and abroad. J Occup Environ Health. 2007;13:236–243 [DOI] [PubMed] [Google Scholar]
- 26.Lippel K. Workers' compensation for asbestos related disease in five Canadian provinces. Canada Research Chair in Occupational Health and Safety Law. 2010 [Google Scholar]
- 27.Mittlestaedt M. Dying For A Lying. Globe and Mail. March 13, 2004 [Google Scholar]
- 28.Hamilton. Available at http://www.thecanadianencyclopedia.com/articles/neutral Published 2012. Accessed 2013.
- 29.Vos MA. Asbestos in Ontario. Ontario Department of Mines and Northern Affairs; 1971 [Google Scholar]
- 30.Keith MM, Brophy JT. Participatory mapping of occupational hazards and disease among asbestos-exposed workers from a foundry and insulation complex in Canada. Int J Occup Environ Health. 2004;10:144–153 [DOI] [PubMed] [Google Scholar]
- 31.Ramazzini C. Asbestos is still with us: repeat call for a universal ban. J Occup Environ Med. 2010;52:469–472 [DOI] [PubMed] [Google Scholar]