

Abstract
Purpose
Robot-assisted radical prostatectomy with pelvic lymph node dissection (RALP-PLND) is a feasible treatment option for high-risk prostate cancer (HPCa), but remains controversial for very high-risk prostate cancer (VHPCa). We aimed to assess the feasibility of RALP-PLND in men ≥70 years with VHPCa features by comparing outcomes to those of HPCa.
Methods
Among patients aged ≥70 years who underwent RALP-PLND between 2005 and 2012, 101 HPCa patients (31%) (PSA≥20 ng/mL or biopsy Gleason 8–10 or cT3a) and 53 VHPCa patients (16%) (≥cT3b or cN1) were identified. Perioperative, functional, and oncological outcomes were compared between groups.
Results
Perioperative outcomes including operative time (P=0.917), estimated blood loss (P=0.181), and complications (P=0.239) were comparable. Due to Gleason score downgrading, 19% of HPCa and 4% of VHPCa were actually of intermediate risk. VHPCa revealed higher LN involvements (P=0.002). Discrepancy between clinical and pathological nodal status was more frequent in VHPCa (36% vs. 7%, P<0.01). Nodal metastasis would have been missed in 23% patients without PLND, while 13% of cN1 patients were shown to be metastasis-free by PLND. Continence rates were lower for VHPCa (32% vs. 56%, P=0.013). Although biochemical recurrence-free survival rates were comparable (P=0.648), risk for later adjuvant treatments was higher for VHPCa patients (14% vs. 34%, P<0.01).
Conclusions
RALP-PLND is a feasible option for VHPCa in elderly patients with satisfactory oncologic outcomes; however, functional outcomes were not as favorable. Patients who are unable to accept the risk of adjuvant therapy and its side effects or incontinence should be deterred from surgical treatment, and other options such as radiation therapy could be an alternative.
Keywords: Aged, Prostate neoplasms, Robotics, Treatment outcome
INTRODUCTION
Prostate cancer (PCa) is the most common malignancy among elderly men and the second most common cause of cancer-related death in industrialized nations [1]. Men aged ≥70 years are known to harbor higher grade cancer with more aggressive features than their younger counterparts [2]. In the context of demographic shifts in the Korean population, the life expectancy has exponentially increased in recent years, as a 70-year-old man today will still have a life expectancy of 13.8 years. With this increase, the percentage of the population aged ≥60 years is projected to increase from 11.4% in 2011 to an estimated 40.1% by 2060 [3]. In line with this expeditious demographic change, age at diagnosis will be higher, and more cases are likely to present high risk features.
Radical prostatectomy (RP) is the preferred treatment option for localized PCa that provides oncological control by decreasing the risks of metastasis and local tumor progression [4]. Although RP is considered feasible as first-choice of a multidisciplinary strategy for high-risk PCa (HPCa), its role in very high-risk PCa (VHPCa) is debatable. With advancements in surgical techniques, studies have suggested that RP with pelvic lymph node dissection (PLND) allows for excellent long-term cancer control for HPCa with cancer-specific and overall survival rates comparable to radiation and hormone combined therapy and higher rates than radiation alone [5]. However, the optimal upper age limit for RP has not been clearly defined, with the current recommendation that at least a 10-year life expectancy should be a prerequisite for an attempted curative therapy [6]. However, with the growth of the elderly population, more men diagnosed with PCa will present higher performance status with less comorbidities, suggesting their suitability as candidates for surgery. Thus, in the near future, calls for reconsideration of therapeutic options for HPCa or VHPCa in elderly men will become more common, as more healthy elderly patients will be considered for surgery among different multidisciplinary options.
It has been reported that robot-assisted laparoscopic radical prostatectomy with PLND (RALP-PLND) allows favorable outcome in elderly men with HPCa; however, there have been no reports regarding VHPCa [7–9]. The objective of this study was to assess the feasibility of RALP-PLND as a first-choice treatment for VHPCa patients by comparing surgical, oncologic, and continence outcomes to those of HPCa patients.
MATERIALS AND METHODS
1. Patient population
From a cohort of 1,201 men who underwent RALP-PLND with or without neoadjuvant therapy by a single surgeon (K.H.R.) between July 2005 and December 2012, data of 325 men (27%) aged ≥70 years were retrospectively reviewed. Staging evaluations included preoperative serum prostate-specific antigen (PSA) level, biopsy Gleason grade, computed tomography (CT) or magnetic resonance imaging (MRI), and a bone scan. Patients were classified into HPCa and VHPCa according to the National Comprehensive Cancer Network (NCCN) criteria [10]: 101 (31%) HPCa, i.e., PSA≥20 ng/mL or a biopsy Gleason 8–10 or a cT3a disease, and 53 (16%) VHPCa, i.e., ≥cT3b or cN1 disease. There were no patients with distant metastasis who were treated by RALP. A detailed explanation of the therapeutic effects of RALP for HPCa and VHPCa, and potential for adjuvant treatments was provided prior to obtaining consent from all patients. Collection of retrospective data of the study was approved by the Institutional Ethics Committee after review of the protocol and procedures employed (2009-0131-001).
2. Operative technique
All RALP was performed via a transperitoneal approach with the extent of PLND being based upon the risk and extent of disease. Standard PLND included the external and obturator fossa area, while extended PLND included the intrapelvic area (obturator, internal and external iliac) and the common iliac area up to the ureteric crossings. Nerve-sparing procedures were performed when cancer lesions were single-sided. The perioperative data analyzed included operative time, estimated blood loss (EBL), and transfusion rates. Complications were categorized according to the Clavien-Dindo classification.
3. Pathological findings
Pathologic factors analyzed included biopsy and prostatectomy Gleason scores, lymphovascular and perineural invasion, positive surgical margin (PSM) status, seminal vesicle (SV), and lymph node (LN) involvement. Clinical stage was determined according to the 7th American Joint Committee on Cancer TNM system.
4. Follow-up
PSA measurements were monitored every three months for the first year and semiannually thereafter. Biochemical recurrence (BCR) was defined as the first of two or more consecutive increases in PSA>0.2 ng/mL at least three months after surgery. Continence was defined as using less than one safety liner per day at 12 months. The timing and intervals of adjuvant multimodal treatments were applied according to surgeon’s discretion based upon the gravity and extent of disease, in consideration of patient’s quality of life and life expectancy.
5. Statistical analysis
Comparisons between groups were assessed by the two-sided Mann-Whitney U-test for the analysis of continuous variables, and the chi-square test for analysis of two or more variables. The probability of BCR-free survival (BCRFS) was estimated and compared using the Kaplan-Meier method. Statistical analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Demographic and perioperative characteristics
The two risk groups showed comparable demographic characteristics including age, body mass index, prostate volume, American Society of Anesthesiologists category, and administration of neoadjuvant hormone therapy (Table 1). There were no disparities regarding perioperative characteristics, i.e., operative time, EBL, rates of transfusion, nerve sparing, or LN dissection. There were no complications of grades ≥IV during surgery or throughout the postoperative period. Rectal injuries occurred in one (2%) and two patients (2%) in the VHPCa and HPCa group, respectively. All were primarily repaired without the necessity of colostomy. Although a total of six (4%) lymphoceles and lymphedemas were observed, none were severe enough to require drainage procedures. Bladder neck contracture was observed in one VHPCa patient at 11 months, and was successfully managed by an endoscopic incision. The most common complication was inguinal hernia, probably due to the high-age cohort. One (2%) VHPCa and three (3%) HPCa patients received surgical repair due to hernia symptoms. In overall, there were no statistical differences in the rate of all Clavien-Dindo categories between groups (P=0.239), with the majority of complications being minor.
Table 1.
Perioperative characteristics
| Characteristic | High-risk (n=101) | Very high-risk (n=53) | P-value |
|---|---|---|---|
| Age (yr) | 73.2 (71–75) | 73.5 (71–75) | 0.594 |
| Body mass index (kg/m2) | 23.9 (22.2–25.4) | 23.6 (21.7–25.3) | 0.448 |
| Preoperative PSA (ng/mL) | 16.8 (6.3–21.7) | 26.3 (8.1–35.3) | <0.001 |
| Prostate volume (gm) | 38.2 (25.4–47.1) | 38.4 (24.6–43.8) | 0.928 |
| ASA category | 0.501 | ||
| 1 | 45 (60) | 25 (52) | |
| 2 | 30 (40) | 23 (48) | |
| Neoadjuvant hormone therapy | 20 (26) | 18 (36) | 0.139 |
| Nerve sparing | 0.729 | ||
| No | 13 (19) | 6 (17) | |
| Unilateral | 11 (17) | 4 (11) | |
| Bilateral | 43 (64) | 25 (72) | |
| Lymph node dissection | |||
| Standard | 49 (66) | 28 (60) | |
| Extended | 25 (33) | 19 (41) | |
| Operative time (min) | 199.1 (168–219) | 200.1 (170–230) | 0.917 |
| Estimated blood loss (mL) | 284.2 (150–400) | 347.4 (200–500) | 0.181 |
| Complicationsa) | 13 (12) | 9 (15) | 0.239 |
| Grade I | |||
| Lymphedema/lymphocele | 4 (4) | 2 (4) | |
| Grade II | |||
| Transfusion | 1 (1) | 1 (2) | |
| Grade III | |||
| Bladder neck contracture | 0 (0) | 1 (2) | |
| Inguinal hernia | 6 (6) | 4 (8) | |
| Rectal injury | 2 (2) | 1 (2) | |
Values are presented as median (interquartile range) and number (%). PSA, prostate-specific antigen; ASA, American Society of Anesthesiologists.
Complications are categorized by the Clavien-Dindo classification.
2. Pathologic characteristics
Pathologic characteristics of both groups are shown in Table 2. VHPCa patients had higher Gleason grades on final pathology (P=0.007), whereas distributions of biopsy grades were similar. When the rates of Gleason upgrading and downgrading were analyzed within each group, VHPCa patients showed significantly less rates of downgrading compared to HPCa patients (9% vs. 32%, P=0.001). Tumor volumes, PSM rates, and lymphovascular and perineural invasion rates were comparable between the groups (P>0.05). However, VHPCa patients had more SV invasion (23% vs. 7%, P=0.005) and LN involvement (25% vs. 7%, P=0.002), even though LN yields were comparable (15.3±7.9 vs. 15.9±7.7, P=0.663). As shown in Table 3, a substantial discrepancy between clinical and pathologic nodal status was noted. Among VHPCa patients, nodal metastasis would have been missed in 12 patients (23%) if PLND had not been performed. On the other hand, seven patients (13%) who were suspected of LN metastasis were proven to be metastasis-free by PLND.
Table 2.
Perioperative characteristics
| Characteristic | High-risk (n=101) | Very high-risk (n=53) | P-value |
|---|---|---|---|
| % Cores positive at biopsy | 33.3 (16.7–50) | 55.8 (30–85.7) | <0.001 |
| Biopsy Gleason sum | 0.258 | ||
| ≤6 | 20 (20) | 10 (19) | |
| 7 | 25 (25) | 11 (21) | |
| ≥8 | 55 (55) | 31 (60) | |
| Pathologic Gleason sum | 0.007 | ||
| ≤6 | 10 (10) | 3 (6) | |
| 7 | 51 (52) | 21 (40) | |
| ≥8 | 38 (38) | 29 (54) | |
| Upgrading | 26 (26) | 14 (26) | 0.904 |
| Downgrading | 33 (32) | 5 (9) | 0.001 |
| Positive surgical margin | 47 (47) | 43 (60) | 0.103 |
| Tumor volume | 4.1 (0.9–4.5) | 5.5 (1.5–8.7) | 0.239 |
| Seminal vesicle invasion | 7 (7) | 12 (23) | 0.005 |
| Lymph node involvement | 7 (7) | 13 (25) | 0.002 |
| Lymph node yield | 15.3 (9–21) | 15.9 (11–21) | 0.663 |
| Lymphovascular invasion | 11 (11) | 7 (13) | 0.656 |
| Perineural invasion | 65 (65) | 34 (65) | 0.962 |
Values are presented as median (interquartile range) and number (%).
Table 3.
Discrepancies between clinical and pathologic lymph nodal status
| pN0 | pN1 | |
|---|---|---|
| High risk | ||
| cN0 | 94 (93) | 7 (7) |
| cN1 | 0 (0) | 0 (0) |
| Very-high risk | ||
| cN0 | 31 (58) | 12 (23) |
| cN1 | 7 (13) | 3 (6) |
Values are presented as number (%).
3. Follow-up characteristics
Median follow-up period for HPCa and VHPCa patients were 31.1 and 36.1 months, respectively. Overall BCRFS rates of VHPCa and HPCa patients were 58% and 77%, respectively (Fig. 1) (P=0.648), with no difference in the time to BCR (13.3 months vs. 12.4 months, P=0.803). However, higher rates of adjuvant treatments were noted for VHPCa patients compared with HPCa patients (38% vs. 15%, P<0.001). The rate of urinary continence was lower in VHPCa patients at 12 months (32% vs. 56%, P=0.013), although there were no differences in the incidence of either previous TURP or bladder neck reconstruction during RALP (Table 4).
Fig. 1.
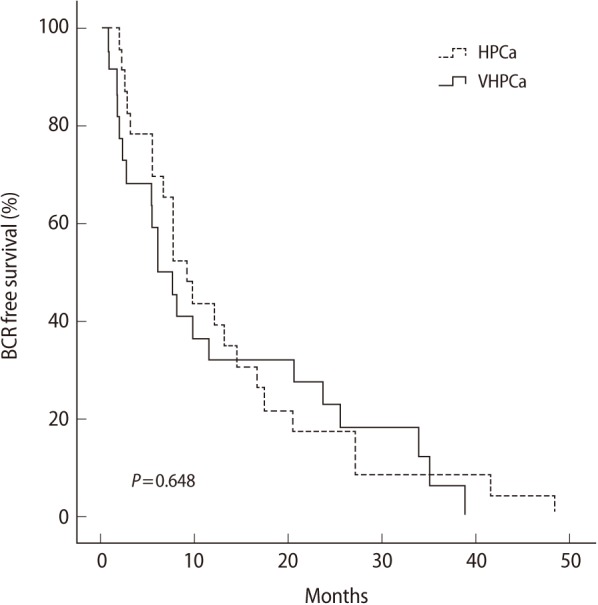
Kaplan-Meier curves for biochemical recurrence (BCR)-free survival of patients with high risk and very-high risk prostate cancer. HPCa, high-risk prostate cancer; VHPCa, very high-risk prostate cancer.
Table 4.
Follow-up characteristics
| Characteristic | High-risk (n=101) |
Very high-risk (n=53) |
P-value |
|---|---|---|---|
| Follow-up period | 31.1 (17.9–41.9) | 36.1 (24.7–49.9) | 0.053 |
| Continent at 12 months | 38 (56) | 14 (32) | 0.013 |
| Overall BCR-free survival | 78 (77) | 31 (58) | 0.648 |
| Time to BCR | 13.3 (5.5–17.5) | 12.4 (2.1–24.1) | 0.803 |
| Adjuvant treatment | <0.001 | ||
| Hormone | 11 (11) | 14 (26) | |
| Radiation | 2 (2) | 2 (4) | |
| Both | 2 (2) | 2 (4) |
Values are presented as median (interquartile range) and number (%). BCR, biochemical recurrence.
DISCUSSION
Key determinants to consider when deciding upon PCa treatment are Gleason grade, PSA level, and remaining life expectancy [11]. The optimal treatment for HPCa in elderly men is especially controversial given the heterogeneous nature of PCa in this particular group [12]. The traditional view is that the outcomes of surgery in these risk settings do not surpass those of radiation or hormone monotherapy, with combined therapy accepted as the preferred treatment [13]. However, recent data suggest that surgery has expanded its indications to higher risk settings and that it yields long-term cancer control comparable to radiation and hormone combined therapy, and higher than radiation alone [5,13,14]. We expanded upon these studies in terms of surgical, functional, and oncologic outcomes to assess the feasibility of RALP-PLND as a first-choice among multidisciplinary treatments in elderly men with VHPCa.
The optimal upper age limit for surgery in PCa is not clearly defined. The current recommendation is that a 10-year life expectancy should be a prerequisite for attempted curative therapy due to the perception that elderly men are unlikely to gain benefit [15]. In fact, rates of RP have been shown to decline in patients aged ≥70 years [2]. However, with an exponential increase in life expectancy, these men are expected to have more than a 13-year remaining life expectancy and are thus likely to present higher performance status and less comorbidities at diagnosis. With this demographic shift, Albertsen et al. [16] observed that men aged ≥70 years with HPCa are likely to have higher morbidity and mortality from their cancer than from other causes without curative treatment.
It is noteworthy that the elderly population shows parameters consistent with aggressive disease, with higher grade and lower prevalence of organ-confined disease than their younger counterparts [17]. It has been reported that potentially curative therapy may confer gain in life expectancy for poorly differentiated PCa even for men upto the age of 75 [15]. Hence, old age should not be the sole criterion to rule out curative therapy. Rather, the focus should be on gaining control of the cancer, as these patients with Gleason score ≥8, are significantly at risk of morbidity or mortality from disease progression as opposed to other causes. Within a high-risk setting, recent studies have reported 5- and 10-year BCRFS rates to range from 45% to 62% and 43% to 51%, respectively [5,18]. Although studies lacked homogeneity with respect to study settings, the 3-year BCRFS rates of our VHPCa and HPCa groups fell safely into the range of these studies. A bias exists when our results are compared, in that the definition of HPCa was different; most prior studies have defined it as ≥T2c, whereas we used ≥T3a as the definition. Therefore, presuming that our results did not overestimate BCRFS rates, we believe the benefit of RALP-PLND in VHPCa is comparable to that of HPCa.
Accurate Gleason grading is an important determinant for staging evaluation and planning of future management. However, a downgrading rate of 20% and an upgrading rate of 9% to 27% have been reported for cT3 disease [5,13]. If accurate biopsy grades were reported for our patients, 19% of HPCa and 4% of VHPCa patients would have fallen into the intermediate risk group; accordingly, only 9% of patients in our overall cohort had developed BCR. Considering that surgery is the only treatment that allows for Gleason grade restaging, the general exclusion of these risk groups from surgery may have placed them at risk of adverse effects implicit with adjuvant therapy.
Radiographically diagnosed metastatic LNs in VHPCa pose a dilemma regarding the selection of optimal therapy [19]. Many clinicians recommend hormone therapy and are reluctant to suggest definitive local therapy [20]. However, recent data suggest that debulking of the primary tumor with PLND could improve cancer-specific and overall survival by means of regional disease control [14]. Bader et al. [21] proposed that there is heterogeneity in the degree of metastasis and that patients with a minimal extent of metastasis may benefit from meticulous PLND. Moreover, patients who received surgery for metastatic PCa were shown to have better response and survival outcomes upon adjuvant hormonal ablation [14].
Inaccuracy of imaging modalities in detecting LN metastasis is another limitation that precludes surgery in cases of nonmetastatic VHPCa [19]. While patients misinterpreted as having positive nodes would have immediately started systemic therapy if PLND had not been performed, those without evidence of LN metastasis can be observed to determine when or if at all adjuvant therapy is needed. In contrast, patients proven to have nodal metastasis by PLND can be considered for early adjuvant therapy. Overall, RALP-PLND could be considered as the standard for accurate nodal staging and local disease control, especially for LN metastatic patients.
In the context of post-RALP functional outcomes in the elderly population, studies have reported 1-year continence rates of men aged 60, 70, and 75 to be 53%, 63%, and 46%, respectively [18,22]. However, these results need to be interpreted with caution, considering various definitions of continence and the distinct populations utilized in assessing outcomes. By defining continence as requiring less than one safety liner per day, rates of the HPCa group were comparable to those of prior studies [18,22]. However, VHPCa patients showed lower rates, probably in part due to aggressive extra-fascial approaches along with wider bladder neck resections.
We note that our study had several limitations. First was the small number of the cohort due to patient selection of a single surgeon. Furthermore, surgeries performed by a single high-volume surgeon may have affected treatment outcomes, as several studies have reported that BCR is associated with surgical experience [23]. Second, the cohort may not represent all men with HPCa and VHPCa, due to the selection of relatively healthy patients aged ≥70 years who were willing to undergo surgery even when given multidisciplinary treatment options. Therefore, our findings may not hold true for the younger counterpart. Third, the NCCN risk stratification criteria for HPCa or VHPCa are one of many definitions to date, causing heterogeneity in the comparison of outcomes of prior studies. Fourth, the learning curve of the surgeon during the study period of eight years was not accounted for in the analysis; thus, surgical and oncologic outcomes may have been affected by such confounder. Lastly, our thesis stands on the solid hypothesis that surgery is a feasible treatment option for HPCa; however, without well-designed randomized control trials, the question whether these patients will benefit from RALP-PLND in terms of both oncological and functional results will need to be further investigated.
In conclusion, RALP-PLND is a feasible option for elderly patients with VHPCa in terms of surgical and oncological outcomes, but not functional outcomes. Our data will assist in preoperative counseling of elderly patients, whereas those who are unable to accept the higher risk of adjuvant therapy and its related side effects and incontinence would need to consider alternate treatment options such as radiation therapy.
ACKNOWLEDGMENTS
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (grant number: NRF-2012R1A1A1042668).
Footnotes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.Lee SH, Kim KH, Choi JH, Koo KC, Lee DH, Chung BH. Can microfocal prostate cancer be regarded as low-risk prostate cancer? Prostate Int. 2013;1:158–62. doi: 10.12954/PI.13028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kunz I, Musch M, Roggenbuck U, Klevecka V, Kroepfl D. Tumour characteristics, oncological and functional outcomes in patients aged ≥ 70 years undergoing radical prostatectomy. BJU Int. 2013;111(3 Pt B):E24–9. doi: 10.1111/j.1464-410X.2012.11368.x. [DOI] [PubMed] [Google Scholar]
- 3.National vital statistics reports [Internet] Daejeon: Statistics Korea; c2008. [cited 2013 Dec 2]. Available from: http://kostat.go.kr/portal/english/surveyOutlines/1/4/index.static. [Google Scholar]
- 4.Liss MA, Lusch A, Morales B, Beheshti N, Skarecky D, Narula N, et al. Robot-assisted radical prostatectomy: 5-year oncological and biochemical outcomes. J Urol. 2012;188:2205–10. doi: 10.1016/j.juro.2012.08.009. [DOI] [PubMed] [Google Scholar]
- 5.Xylinas E, Dache A, Roupret M. Is radical prostatectomy a viable therapeutic option in clinically locally advanced (cT3) prostate cancer? BJU Int. 2010;106:1596–600. doi: 10.1111/j.1464-410X.2010.09630.x. [DOI] [PubMed] [Google Scholar]
- 6.Greco KA, Meeks JJ, Wu S, Nadler RB. Robot-assisted radical prostatectomy in men aged > or =70 years. BJU Int. 2009;104:1492–5. doi: 10.1111/j.1464-410X.2009.08718.x. [DOI] [PubMed] [Google Scholar]
- 7.Ou YC, Yang CK, Wang J, Hung SW, Cheng CL, Tewari AK, et al. The trifecta outcome in 300 consecutive cases of robotic-assisted laparoscopic radical prostatectomy according to D’Amico risk criteria. Eur J Surg Oncol. 2013;39:107–13. doi: 10.1016/j.ejso.2012.10.003. [DOI] [PubMed] [Google Scholar]
- 8.Punnen S, Meng MV, Cooperberg MR, Greene KL, Cowan JE, Carroll PR. How does robot-assisted radical prostatectomy (RARP) compare with open surgery in men with high-risk prostate cancer? BJU Int. 2013;112:E314–20. doi: 10.1111/j.1464-410X.2012.11493.x. [DOI] [PubMed] [Google Scholar]
- 9.Pierorazio PM, Mullins JK, Eifler JB, Voth K, Hyams ES, Han M, et al. Contemporaneous comparison of open vs minimally-invasive radical prostatectomy for high-risk prostate cancer. BJU Int. 2013;112:751–7. doi: 10.1111/j.1464-410X.2012.11757.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mohler JL. The 2010 NCCN clinical practice guidelines in oncology on prostate cancer. J Natl Compr Canc Netw. 2010;8:145. doi: 10.6004/jnccn.2010.0010. [DOI] [PubMed] [Google Scholar]
- 11.Koo KC, Lee DH, Lee SH, Chung BH. Peripheral zone prostate-specific antigen density: an effective parameter for prostate cancer prediction in men receiving 5α-reductase inhibitors. Prostate Int. 2013;1:102–8. doi: 10.12954/PI.13022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sridharan S, Warde P. The importance of local control in high-risk locally advanced prostate cancer. Curr Oncol. 2012;19(Suppl 3):S6–12. doi: 10.3747/co.19.1279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jayram G, Decastro GJ, Large MC, Razmaria A, Zagaja GP, Shalhav AL, et al. Robotic radical prostatectomy in patients with high-risk disease: a review of short-term outcomes from a high-volume center. J Endourol. 2011;25:455–7. doi: 10.1089/end.2010.0349. [DOI] [PubMed] [Google Scholar]
- 14.Oderda M, Joniau S, Spahn M, Gontero P. Debulking surgery in the setting of very high-risk prostate cancer scenarios. BJU Int. 2012;110(6 Pt B):E192–8. doi: 10.1111/j.1464-410X.2012.10942.x. [DOI] [PubMed] [Google Scholar]
- 15.Alibhai SM, Naglie G, Nam R, Trachtenberg J, Krahn MD. Do older men benefit from curative therapy of localized prostate cancer? J Clin Oncol. 2003;21:3318–27. doi: 10.1200/JCO.2003.09.034. [DOI] [PubMed] [Google Scholar]
- 16.Albertsen PC, Hanley JA, Fine J. 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA. 2005;293:2095–101. doi: 10.1001/jama.293.17.2095. [DOI] [PubMed] [Google Scholar]
- 17.Ko J, Falzarano SM, Walker E, Streator Smith K, Stephenson AJ, Klein EA, et al. Prostate cancer patients older than 70 years treated by radical prostatectomy have higher biochemical recurrence rate than their matched younger counterpart. Prostate. 2013;73:897–903. doi: 10.1002/pros.22635. [DOI] [PubMed] [Google Scholar]
- 18.Rogers CG, Sammon JD, Sukumar S, Diaz M, Peabody J, Menon M. Robot assisted radical prostatectomy for elderly patients with high risk prostate cancer. Urol Oncol. 2013;31:193–7. doi: 10.1016/j.urolonc.2010.11.018. [DOI] [PubMed] [Google Scholar]
- 19.Hall MA, Kwon S, Robinson H, Lachance PA, Azhdarinia A, Ranganathan R, et al. Imaging prostate cancer lymph node metastases with a multimodality contrast agent. Prostate. 2012;72:129–46. doi: 10.1002/pros.21413. [DOI] [PubMed] [Google Scholar]
- 20.Cooperberg MR, Grossfeld GD, Lubeck DP, Carroll PR. National practice patterns and time trends in androgen ablation for localized prostate cancer. J Natl Cancer Inst. 2003;95:981–9. doi: 10.1093/jnci/95.13.981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bader P, Burkhard FC, Markwalder R, Studer UE. Disease progression and survival of patients with positive lymph nodes after radical prostatectomy. Is there a chance of cure? J Urol. 2003;169:849–54. doi: 10.1097/01.ju.0000049032.38743.c7. [DOI] [PubMed] [Google Scholar]
- 22.Shikanov S, Desai V, Razmaria A, Zagaja GP, Shalhav AL. Robotic radical prostatectomy for elderly patients: probability of achieving continence and potency 1 year after surgery. J Urol. 2010;183:1803–7. doi: 10.1016/j.juro.2010.01.016. [DOI] [PubMed] [Google Scholar]
- 23.Sooriakumaran P, Haendler L, Nyberg T, Gronberg H, Nilsson A, Carlsson S, et al. Biochemical recurrence after robot-assisted radical prostatectomy in a European single-centre cohort with a minimum follow-up time of 5 years. Eur Urol. 2012;62:768–74. doi: 10.1016/j.eururo.2012.05.024. [DOI] [PubMed] [Google Scholar]