

Abstract
Spigelian hernias were first described by Joseph Klinkosch in the 18th century, and have since posed a diagnostic and surgical problem owing to their non-specific presentation and rarity. While the management of unilateral hernias is fairly well described in today’s literature, bilateral Spigelian hernias are very rare. We describe the emergency management of a patient with bilateral Spigelian hernias, diagnosed on computed tomography.
Keywords: Bilateral Spigelian hernia, Emergency, Management
Case history
A 52-year-old woman was admitted to the surgical assessment unit after having developed right iliac fossa pain over the previous 12 hours. The onset was gradual and the pain had worsened with time. She had noticed a swelling over the right side. She had opened her bowels normally that day and, despite being nauseated, she had not vomited. She had no urinary or gynaecological symptoms. The patient was otherwise fit and well, and had not undergone any previous surgery. She was on no regular medication. She smoked 15 cigarettes a day and drank alcohol rarely.
On arrival, the patient’s vital observations were entirely normal. Examination revealed a very tender right iliac fossa with voluntary guarding. There was a distinct 10cm × 10cm smooth mass palpable, which appeared to be intra-abdominal rather than in the abdominal wall. This was particularly tender and did not have a cough impulse. The remainder of the abdomen was soft. Rectal examination revealed an empty rectum. Her routine blood results on admission were within the normal limits and an arterial blood gas showed a normal lactate level of 0.9mmol/l.
In view of the rapid onset of symptoms and despite the lack of inflammatory features, the main differential diagnosis at this stage was an appendicular mass and computed tomography (CT) was organised. This revealed bilateral Spigelian hernias (Figs 1 and 2). The left contained small bowel loops and the descending colon. The right contained the caecum and ileum with surrounding fat stranding, suggesting the presence of reactive inflammatory changes.
Figure 1.

Coronal computed tomogaphy demonstrating bilateral Spiegelian hernias
Figure 2.
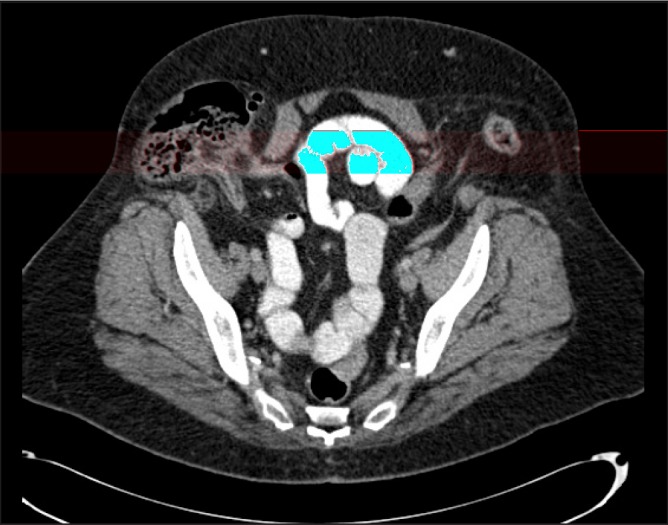
Axial computed tomogaphy demonstrating bilateral Spiegelian hernias
A laparoscopy was performed and reduction of the right-sided hernia (Fig 3) was attempted. The left side had reduced prior to surgery. The plan was to repair both hernias simultaneously at laparoscopy. Unfortunately, this was not possible as it was impossible to reduce the incarcerated caecum safely. A midline laparotomy incision was made and the hernia reduced manually via an intra-abdominal approach. The caecum, appendix and terminal ileum were extracted and deemed viable. The right-sided peritoneal defect was plicated using 3/0 Vicryl® (Ethicon, Somerville, NJ, US) interrupted sutures. The midline incision was then closed in a standard fashion. A transverse incision was made over the right hernial orifice and the defect repaired with size 0 Prolene® (Ethicon) continuous sutures. The left hernia was not fixed on this occasion.
Figure 3.
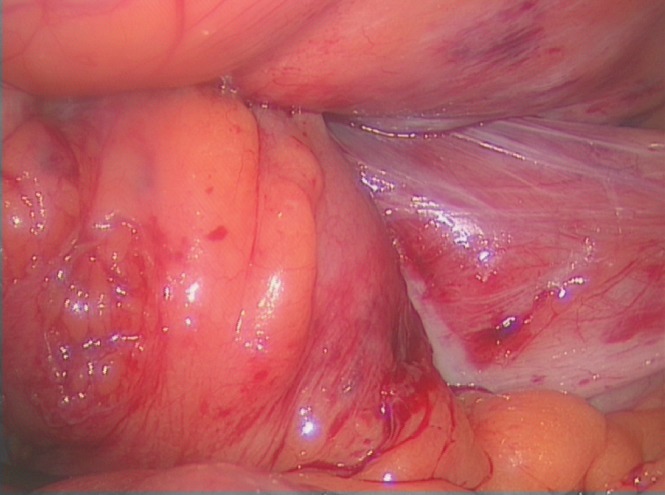
Laparoscopic view of right Spigelian hernia with caecum entering the defect
Discussion
Spigelian hernias were first described by Joseph Klinkosch in the 18th century. 1 They are a rare type of abdominal hernia that protrudes through a defect in the linea semilunaris, usually in the lower abdomen owing to an absence of the posterior sheath. The hernial orifice is a well defined defect in the transversus aponeurosis. Spigelian hernias can either be congenital or acquired. Bilateral hernias are very rare, especially in adults. In children, they have been associated with other congenital anomalies.
Diagnosis of Spigelian hernias is notoriously difficult, partly owing to the presence of non-specific symptoms and partly owing to their rarity. In our case, where a so-called intra-abdominal mass was felt and considering the diffuse tenderness over the right iliac fossa with associated guarding, the diagnosis of an intra-abdominal pathology, more specifically appendicitis, seemed most likely. Furthermore, no left-sided mass or defect was felt despite CT revealing a contralateral hernia.
Traditionally, Spigelian hernias were repaired via an open approach but the majority of unilateral cases are now repaired laparoscopically via a transperitoneal approach. Once a diagnosis of Spigelian hernia is established, repair (either as an emergency or elective procedure) is essential due to high strangulation rates. A paper from 2012 describing 16 cases of Spigelian hernias reported that half of the cases required emergency repair. 2
Management of bilateral hernias is more complex as very few cases are described in the literature. A search using OvidSP and PubMed with the terms ‘Spigelian hernia’ and ‘bilateral’ in the title/abstract revealed five articles reporting bilateral cases of Spigelian hernias after excluding those not written in the English language and those reporting congenital paediatric cases. 1–5 Both the laparoscopic and the open approach in their management have been reported. Naik et al describe a case of bilateral hernias in an elderly man that were repaired laparoscopically using two-layered Prolene® meshes 3 while Safioleas et al describe a more traditional open approach in a middle aged woman. 4
Our case had to be managed as an emergency in view of the incarcerated right-sided hernia. In an ideal situation, both hernias would have been reduced once the patient was fully anaesthetised and relaxed, subsequently allowing laparoscopic bilateral repair with mesh as in Naik et al’s case. 3 As it was impossible to reduce the right-sided hernia, a laparotomy had to be performed. It was decided not to use a mesh owing to the presence of inflammatory changes. Adequate exposure of the sheath required for primary repair was not possible via the midline incision. Further lateral incisions over the defects were therefore necessary. As the right hernia had been incarcerated and contained the caecum, it was decided that this defect required more urgent repair. To spare the patient a third incision, the left defect was not repaired on this occasion. The patient will be brought back to have this repaired electively.
Conclusions
Bilateral Spigelian hernias are very rare and their management is therefore poorly reported in the literature. We feel that a laparoscopic approach is the most feasible, allowing repair of both sides simultaneously. This was not possible in our case owing to the incarcerated right side. A laparotomy with open reduction and subsequent open repair with sutures of the right-sided hernia was performed while the left side will be repaired in the near future.
References
- 1.Zeina AR, Mahamid A, Sakran N, Troitsa A. Computed tomographic diagnosis of incarcerated Meckel’s diverticulum in a patient with bilateral Spigelian hernia. J Gastrointest Surg 2012; 16: 447–449. [DOI] [PubMed] [Google Scholar]
- 2.Perrakis A, Velimezis G, Kapogiannatos Get al Spigel hernia: a single center experience in a rare hernia entity. Hernia 2012; 16: 439–444. [DOI] [PubMed] [Google Scholar]
- 3.Naik S, Kapoor S, Sharma SK, Varshney S. Bilateral Spigelian hernia treated by two-layered prolene mesh. Surg Pract 2006; 10: 82–83. [Google Scholar]
- 4.Safioleas M, Stamatakos M, Moulakakis Ket al Spigelian hernia. A rare case of bilateral hernia and presentation of our experience. Chirurgia 2007; 102: 429–432. [PubMed] [Google Scholar]
- 5.Torzilli G, Carmana G, Lumachi Vet al The usefulness of ultrasonography in the diagnosis of the Spigelian hernia. Int Surg 1995; 80: 280–282. [PubMed] [Google Scholar]