

Abstract
Background
A high level of resistance in Neisseria gonorrhoeae has developed against penicillins, sulphonamides, tetracyclines and quinolones, and recent surveillance data have shown a gradual reduction in sensitivity to current first-line agents with an upward drift in the minimum inhibitory concentration of ceftriaxone. Laboratory sensitivity testing suggests that gentamicin, an aminoglycoside, may be an effective treatment option for gonorrhoea infection when used as a single intramuscular dose.
Methods
A search of electronic reference databases and grey literature was used to identify randomised trials and well-conducted prospective studies with concurrent controls evaluating single-dose gentamicin against placebo or a comparator regimen in the treatment of uncomplicated gonorrhoea infection in men and women aged 16 years and over. The primary outcome was microbiological cure of N. gonorrhoeae.
Results
Eight hundred and thirty-nine studies were identified, of which five (1,063 total participants) were included. All five studies administered single-dose gentamicin via intramuscular injection to men with uncomplicated gonococcal urethritis. Three studies were randomised trials, one was quasi-randomised and one was non-randomised but included a comparator arm. Comparator antibiotics included an alternative aminoglycoside or antibiotic used in the syndromic management of male urethritis. Methodology was poorly described in all five included studies. The high risk of bias within studies and clinical heterogeneity between studies meant that it was inappropriate to pool data for meta-analysis. Cure rates of 62% to 98% were reported with gentamicin treatment. The relative risk of cure was comparable between gentamicin and comparator antibiotics.
Conclusions
The studies identified provide insufficient data to support or refute the efficacy and safety of single-dose intramuscular gentamicin in the treatment of uncomplicated gonorrhoea infection. Additional randomised trials to evaluate gentamicin for this indication are therefore required.
Systematic review registration
PROSPERO CRD42012002490
Keywords: Gonorrhoea, Neisseria gonorrhoeae, Gentamicin, Treatment
Background
Gonorrhoea, caused by Neisseria gonorrhoeae, is the second most common bacterial sexually transmitted infection in the UK. The number of gonorrhoea diagnoses continues to rise with latest data indicating a 52% increase in England from 16,835 to 25,525 infections between 2010 and 2012 [1]. The highest rates of infection are found in residents of urban areas, and infection is concentrated in core groups such as young people and men who have sex with men (MSM). Of male diagnoses in 2012, 42% were reported in MSM and 55% of heterosexual diagnoses were in those aged 15 to 24 years [1]. A number of factors, in addition to continuing levels of unsafe sexual behaviour, may have contributed to the observed increase in diagnosis of gonorrhoea including the introduction of highly sensitive nucleic acid amplification tests (NAATs), the introduction of self-testing including extra-genital sites (pharyngeal and rectal sites in MSM), an increase in sexual health screening following the roll-out of the National Chlamydia Screening Programme, and improvements in reporting and surveillance. However, the rise in incident infection reported in the UK mirrors the global trend; the World Health Organization (WHO) estimates gonorrhoea to represent 106.1 million of the 498.9 million new cases of curable sexually transmitted infections (syphilis, chlamydia, gonorrhoea and trichomoniasis) worldwide [2].
N. gonorrhoeae are intracellular gram-negative bacteria transmitted via sexual contact. They primarily infect the mucous membranes of the urethra, endocervix, rectum, pharynx and conjunctiva. Infection of the genital tract causes local inflammation that can result in dysuria, discharge, genital discomfort and pain. Infection in women may spread to the fallopian tubes and ovaries causing pelvic inflammatory disease (PID). Complications include infertility, chronic pelvic pain and ectopic pregnancy and can result in considerable physical and emotional morbidity in addition to a significant financial burden on health-care services [3,4]. An estimate of the average lifetime costs for women who develop complications is $6,350 for chronic pelvic pain, $6,840 for ectopic pregnancy and $1,270 for infertility [4].
Gonorrhoea has consistently been identified as a risk factor for incident HIV infection in both heterosexual and MSM populations [5-7]. This is thought to result from increased HIV viral shedding in genital secretions [8,9] and from an increased concentration of target cells for HIV in the locally inflamed mucosa found in individuals with gonorrhoea [10]. Ensuring effective gonorrhoea testing and treatment is therefore important to both reduce the global incidence of curable sexually transmitted infections and control the spread of HIV.
Testing guidance advocates the use of NAATs to detect gonorrhoea [11-14]. These tests benefit from high sensitivity and specificity, quick turnaround times, ability to use non-invasive specimens from patients and permitting dual screening for chlamydia and gonorrhoea at extra-genital sites. However, to allow antibiotic susceptibility testing, a sample for culture is also required. In vitro susceptibility testing is used to guide individual patient management in addition to providing data for surveillance programmes. Antibiotic resistance in N. gonorrhoeae is a continuing problem, and surveillance of antibiotic resistance with a change in empirical treatment when resistance occurs in >5% of isolates is recommended [15]. This is of particular importance in resource-limited settings where testing for N. gonorrhoeae is difficult and individuals are typically treated using syndrome-based algorithms.
A high level of resistance in N. gonorrhoeae has developed against penicillins, sulphonamides, tetracyclines and fluoroquinolones, which are now no longer recommended for use. Current guidelines recommend a single dose of intramuscular ceftriaxone with or without the addition of a single oral dose of azithromycin for the treatment of uncomplicated gonorrhoea infection [12,14,16,17]. The European Centre for Disease Prevention and Control (ECDC) has proposed a working case definition for confirmed treatment failure that includes both clinical and laboratory criteria [18]. The precise resistance breakpoint for cephalosporin antibiotics is unknown, but surveillance data from the gonococcal isolate surveillance projects in both the UK and US have reported an upward drift in the mean inhibitory concentration (MIC) of ceftriaxone (UK: 13% with MIC over 0.03 mg/l in 2010 cf. 1% in 2007 [19]; US: 0.05% with MIC over 0.125 mcg/ml in 2006 cf. 0.5% in 2010 [20]). Clinical failure of cephalosporins has now been reported in Japan and Europe [21-23].
The mechanism of resistance to cephalosporin antibiotics is not fully understood. Plasmid-mediated resistance has not been observed, but a number of chromosomal mechanisms, including the presence of mosaic penA genes and mutations in penA, penB, mtrR promoter and mtrR genes, have been reported. Mosaicism of the penA gene that encodes penicillin-binding protein 2 (PBP2) is thought to be the predominant mechanism causing cephalosporin resistance. Penicillin-binding proteins are involved in the synthesis of peptidoglycan, a major component of bacterial cell walls. Mosaic sequences of PBP2, resulting from recombination events involving penA gene sequences from other Neisseria species, have been identified in clinical isolates that demonstrate reduced susceptibility to cefixime and ceftriaxone [24-26]. Options to treat gonorrhoea if cephalosporins become ineffective are severely limited.
Gentamicin, an aminoglycoside antibiotic, is known to be clinically effective in the treatment of gram-negative infections, exerting both a bacteriostatic and bactericidal effect. It is an inexpensive antibiotic and has been used successfully to treat genital gonorrhoea infections in resource-limited settings. Studies in Malawi have shown high susceptibility of gonococcal isolates to gentamicin in vivo and clinical cure rates of approximately 95% when used in combination with doxycycline [27,28]. Whilst it is not included in current UK or European gonorrhoea treatment guidelines, an evaluation of gentamicin susceptibility of gonorrhoea isolates across 17 European countries was performed in 2009 in response to the emergence of decreased susceptibility to third-generation, extended-spectrum cephalosporins. The majority of MICs for genital and rectal isolates fell within a narrow range: 95% of isolates within 4–8 mg/l and 79% of isolates demonstrating an MIC of 8 mg/l [29]. Cephalosporin-resistant gonococci are unlikely to exhibit cross-resistance to gentamicin given its bacteriostatic action via the bacterial ribosome in contrast to the action of cephalosporins on bacterial cell wall synthesis. Administration of gentamicin is limited to either the intravenous or intramuscular routes, and the optimal dose for uncomplicated genital infections is not known. However, a single intramuscular injection of antibiotic lends itself to outpatient management and may reduce the risk of vestibular and renal toxicity that is seen with extended high trough drug concentrations.
In view of concerns about decreasing sensitivity of N. gonorrhoeae to current first-line agents, there is a clear need to identify treatment options. This systematic review assesses the clinical effectiveness and safety of gentamicin for the treatment of N. gonorrhoeae.
Methods
The review protocol was registered with PROSPERO (CRD42012002490) [30].
Criteria for considering studies for the review
Types of study
Randomised controlled trials, quasi-randomised trials and prospective studies with concurrent controls and consistent treatment assignment were eligible for inclusion. Studies with historical controls, before and after studies, case series and case reports were excluded.
Types of participants
Studies recruiting men and women aged 16 years or over receiving their first antibiotics as an inpatient or outpatient for a microbiological diagnosis of gonorrhoea at any anatomical site were included. Gonorrhoea was diagnosed by microscopy, culture or nucleic acid amplification tests.
Types of intervention
Studies in which gentamicin was given at any single dose intramuscularly or intravenously were eligible for inclusion. To enable assessment of gentamicin efficacy, studies in which gentamicin was given as part of a combined antibiotic regimen were excluded. Comparators included no treatment, placebo or any alternative antibiotic given either orally or parenterally.
Types of outcome
Primary outcome
The primary outcome is microbiological cure of N. gonorrhoeae (negative microscopy, culture or nucleic acid amplification test).
Secondary outcomes
The secondary outcomes are the following:
• Clinical resolution of symptoms (dysuria, genital discharge, genital pain or abdominal pain).
• Need for additional antibiotic therapy.
• Adverse events (rash, allergy, injection site discomfort, renal dysfunction, hearing loss, vestibular dysfunction, other reported adverse events attributed to antibiotic).
• Hospital attendance (admission to hospital, unscheduled clinic attendance).
Search strategy for identification of studies
Electronic searches
A search strategy was developed and used to identify relevant studies (Additional file 1). Databases were searched on 11th May 2012 and 27th July 2012 and updated on 2nd June 2014 as follows: MEDLINE from PubMed 1950 to present, Embase 1980 to present, CINAHL 1981 to present, CAB Abstracts, EThOS and the Cochrane Central Register of Controlled Trials. Searches were repeated of http://www.clinicaltrials.gov and http://www.who.int/trialsearch to identify ongoing trials. Papers published in peer-reviewed journals, theses, conference abstracts and reports were included. No language restriction was placed on the search strategy.
Searching other resources
Searches were repeated in grey literature to identify any unpublished and ongoing research (Additional file 1). References from included studies were reviewed for further relevant studies.
Data collection and analysis
Study selection
Two reviewers (DD and EH) independently screened titles and abstracts against the inclusion criteria to identify eligible citations. Disagreements were resolved by discussion. Full-text copies were obtained if insufficient information was available and of all studies meeting inclusion criteria.
Data extraction
A standardised data extraction form was developed and utilised. Data were independently extracted from the studies, and discrepancies were resolved by discussion and consultation with a third reviewer if necessary.
Assessment of risk of bias
Risk of bias in studies was assessed using the risk of bias tool described in the Cochrane Handbook for Systematic Reviews of Interventions [31]. A bias judgement (low risk of bias, high risk of bias or unclear risk of bias) was allocated to each of six domains (sequence generation, allocation of sequence concealment, blinding, incomplete outcome data, selective reporting bias and other bias) within the tool. The tool was developed for assessment of randomised trials, and the Good Research for Comparative Effectiveness (GRACE) checklist, which has been utilised to rate the quality of observational studies of comparative effectiveness, was used to assess non-randomised studies included for data analysis [32].
Data synthesis
Characteristics, main findings and risk of bias assessment were tabulated for each study. Levels of attrition were noted for included studies. If data were adequate for meta-analysis, we planned that results be presented as a summary risk ratio with 95% confidence intervals, on an intention-to-treat basis.
Reviewing the studies identified a high level of clinical heterogeneity. The dose of gentamicin varied from 160 to 280 mg, and the primary assessment of cure was based on symptoms, microscopy and culture or was not reported. The definition and assessment of risk of re-infection was not reported in some studies [33-35], and those with potential re-exposure were excluded in one study [36]. Meta-analysis was considered to be inappropriate due to these methodological differences and the results summarised in a tabular format.
Results
Eight hundred and thirty-nine studies were identified by the search strategy (Figure 1). Two reviewers independently screened all titles and available abstracts. Nineteen studies were discussed due to disagreement, of which 17 were excluded, as they did not meet pre-specified inclusion criteria. Seventeen full-text articles were retrieved and 12 were excluded after further review.
Figure 1.

Review profile.
Five studies with a total of 1,063 participants were included in the review: three randomised trials [28,33,34], one quasi-randomised trial [36] and one non-randomised study with a comparator arm [35].
Description of studies
Table 1 summarises the characteristics of the included studies. All five studies included men with uncomplicated gonococcal urethritis diagnosed by culture [34], identification of gram-negative diplococci on urethral smear [36] or a combination of Gram-stained urethral smear and culture [28,34,36]. Five hundred and twenty-nine men received intramuscular gentamicin in a single dose—160 mg (n = 20), 240 mg (n = 207) or 280 mg (n = 302). No study compared gentamicin to placebo and comparator antibiotics included an alternative aminoglycoside (kanamycin and spectinomycin) or antibiotic used in the syndromic management of male urethritis.
Table 1.
Characteristics of included studies
| Author | Methods | Participants |
Intervention |
Primary outcome | Evaluation of re-infection | |
|---|---|---|---|---|---|---|
| Gentamicin | Comparator | |||||
| Hira et al. (1984) [36] |
Quasi-random (treatment assigned to alternate consecutive patients) |
Men with uncomplicated gonorrhoea infection (gram-negative diplococci on urethral smear), Lusaka, Zambia |
Single-dose gentamicin 280 mg intramuscular injection (n = 302) |
Single-dose kanamycin 2 g intramuscular injection (n = 113) |
Cure |
All patients advised to abstain from sexual activity for 2 weeks after therapy. |
| Patients in whom N. gonorrhoea persisted or re-appeared (as determined by a positive result of a smear or culture) in the absence of sexual activity during the follow-up period were considered to be treatment failure |
Patients excluded if reported sexual activity during 2 weeks follow-up period with or without persistent or re-appearing gonorrhoea on culture |
|||||
| Iskandar et al. (1978) [33] |
RCT (randomly allocated to 3 groups of 30 patients) |
Men with acute gonorrhoea infection (gonorrhoea on Gram stain of urethral smears), Egypt |
Single-dose gentamicin 240 mg intramuscular injection (n = 30) |
Co-trimoxazole (Bactrim, Roche) 8 tablets daily divided into 2 doses for 2 days (n = 30). Trimethoprim-sulphametrol (Lidaprim, Ciba) 8 tablets divided into 2 doses for 2 days (n = 30) |
Cure |
One case of re-infection reported in which there was a history of re-exposure. |
| Cases with negative smears plus resolution of discharge on day 7 were considered cured |
Safe sex advice and assessment of re-infection not described |
|||||
| Pareek and Chowdhury (1981) [35] |
Non-randomised, comparator study |
Men with urethral gonorrhoea infection (culture positive and beta lactamase detected), Riyadh, Saudi Arabia |
Single-dose gentamicin 160 mg intramuscular injection (n = 20) |
Single-dose spectinomycin 2 g intramuscular injection (n = 20) |
Cure |
Safe sex advice, definition and assessment of re-infection not described |
| Patients in whom culture on days 3, 7 and 14 post treatment were negative were considered cured | ||||||
| Yoon et al. (1988) [34] |
RCT (random numbered tickets used to divide patients into 2 groups) |
Men with uncomplicated gonococcal urethritis (Gram stain and ‘bacteriological test of urethral secretions’), Seoul, Korea |
Single-dose gentamicin 240 mg intramuscular injection (n = 137) |
Single-dose kanamycin 2 g intramuscular injection (n = 137) |
Cure |
All patients advised to avoid sexual intercourse during the period of treatment. Definition and assessment of re-infection not described |
| Cases with negative Gram stain and bacteriological test (undefined) of urethral secretions | ||||||
| Lule et al. (1994) [28] | RCT (computerised randomisation) | Men presenting with urethral discharge +/-dysuria and gram-negative intracellular diplococci on urethral smear and/or positive culture, Malawi | Single-dose gentamicin 240 mg intramuscular injection (n = 40) | Amoxicillin 3 gm, probenecid 1 gm, and clavulanate 125 mg by mouth once (n = 60) |
To determine the relative contribution of gonorrhoea and chlamydia to urethritis in Malawi |
Safe sex advice not described |
| Amoxicillin 3 gm, probenecid 1 gm, and clavulanate 125 mg, by mouth once and doxycycline 100 mg BD for 7 days (n = 56) |
To evaluate the effectiveness of five antibiotic therapies for urethritis |
6/48 (12.5%) patients with persistent gonococcal infection at follow-up reported having sex between initial and follow-up visits compared to 21 of 249 (8.4%) men for whom gonococcal infection was not detected at follow-up (p = 0.4) | ||||
| Ciprofloxacin 250 mg by mouth once (n = 59) |
Cure not defined. An assessment of symptoms and signs, urethral Gram stain and culture were obtained at 8–10 days post treatment | |||||
| Co-trimoxazole (trimethoprim 320 mg/sulphamethoxazole 1,600 mg) by mouth for 2 days (n = 29) | ||||||
RCT randomised control trial, mg milligrams, g grams, BD twice daily.
Assessment of risk of bias
The included studies were assessed for risk of bias using either the Cochrane risk of bias tool (randomised studies) or the GRACE checklist (observational studies). Study methodology was poorly reported, so that consistently assessing methodological quality and risk of bias in each individual study was difficult. Insufficient detail was often included in the publication to distinguish accurately what was done in contrast to what was reported. As such, risk of bias within and across individual studies was unclear or judged by reviewers to be high (Additional file 2).
Effectiveness of gentamicin
All five studies reported cure, as defined in Table 1, as a primary outcome (Table 2). Fixed effects meta-analysis was not performed for any of the defined outcomes due to the high level of clinical heterogeneity between studies and the high risk of bias within individual studies (Additional file 2). Whilst cure, presented as a percentage rate, was reported in each of the included studies, they differed significantly in definition of cure (clinical cure or negative microscopy and/or culture), timing of cure and their assessment of re-infection (Additional file 3).Figure 2 summarises the efficacy of gentamicin in the treatment of uncomplicated gonorrhoea infection. The probability of cure was comparable between gentamicin and comparator antibiotics.
Table 2.
Outcome data of included studies
| Outcome | Hira et al. [36] | Iskandar et al. [33] | Pareek and Chowdhury [35] | Yoon et al. [34] | Lule et al. [28] |
|---|---|---|---|---|---|
|
Cure |
Gentamicin: 98% (216/220) |
Gentamicin: 27/30 (90%) |
Gentamicin: 19/20 (95%) |
Gentamicin: 78/125 (62.4%) |
Gentamicin: 38/40 (95%) |
| Kanamycin: 95% (85/89) |
Co-trimoxazole: 29/30 (96.6%) |
Spectinomycin: 16/20 (80%) |
Kanamycin: 86/126 (68.3%) |
Ciprofloxacin: 55/59 (93%) |
|
| Lidaprim: 29/30 (96.6%) |
23 patients did not attend follow-up and were excluded |
APC: 40/60 (67%) |
|||
| Adjusted to include only those attending on day 7: |
APC-D: 52/56 (93%) |
||||
| Gentamicin: 19/22 (86.4%) |
Co-trimoxazole: 14/29 (48%) |
||||
| Bactrim: 15/16 (93.7%) | |||||
| Lidaprim: 20/21(95.2%) | |||||
|
Need for additional treatment |
No data |
No data |
No data |
No data |
No data |
|
Adverse event |
‘No serious toxicity or other adverse reactions were noticed in either group of men. Serum creatinine values were normal in the 52 patients given gentamicin and the 28 kanamycin whose blood samples were tested’ |
‘No adverse side effects were observed in any of the patients’ |
‘There were no obvious side effects with either of these drugs. The blood urea and creatinine values remained within normal limits’ |
‘There was no side effect of using kanamycin and gentamicin’ |
No data |
| Hospital attendance | No data | No data | No data | No data | No data |
APC amoxicillin, probenecid and clavulanate, APC-D amoxicillin, probenecid, clavulanate and doxycycline, TMPSMX trimethoprim/sulphamethoxazole.
Figure 2.
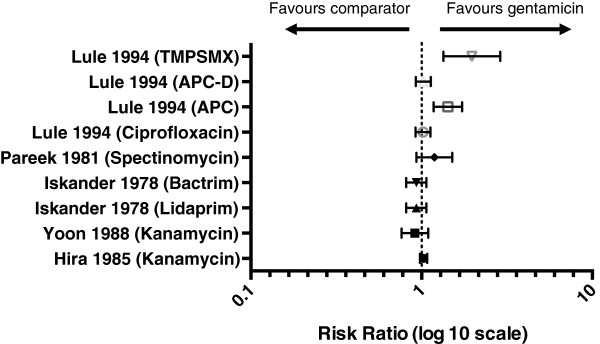
Efficacy of gentamicin. The probability of cure following treatment with gentamicin compared to cure with a comparator antibiotic. The probability of cure was comparable between gentamicin and comparator antibiotics. TMPSMX trimethoprim/sulphamethoxazole, APC amoxicillin, probenecid and clavunate, APC-D amoxicillin, probenecid, clavunate and doxycycline. Risk ratios: Lule (TMPSMX) 1.9679 (95% CI 1.3412-2.8873); Lule (APC-D) 1.0231 (95%CI 0.924201.1325); Lule (APC) 1.4250 (95% CI 1.1754-1.7275); Lule (ciprofloxacin) 1.0191 (95% CI 0.9231-1.1251); Pareek (specinomycin) 1.1875 (95% CI 0.9331-1.5113); Iskander (Bactrim) 0.9310 (95% CI 0.8122-1.0672); Iskander (Lidaprim) 0.9310 (95% CI 0.8122-1.0672); Yoon (kanamycin) 0.9142 (95% CI 0.7630-1.0954); Hira (kanamycin) 1.0280 (95% CI 0.979301.0791).
Discussion
Our systematic review found insufficient data to support or refute the role of gentamicin in the treatment of gonorrhoea infections. Five studies of single-dose intramuscular gentamicin for the treatment of uncomplicated gonococcal urethritis in men met inclusion criteria and reported cure rates of 62% to 98%. The probability of cure was comparable between gentamicin and comparator antibiotics.
A separate systematic review assessing the effectiveness of gentamicin for uncomplicated urogenital gonorrhoea infection has recently been published [37] and reported a pooled percentage with negative culture after single-dose gentamicin of 91.5% (95% CI 88% to 94%). It included three studies of which only two met our inclusion criteria due to methodological differences [36]. Firstly, Dowell and Kirkcaldy included studies with historical controls and single-arm case series. Secondly, they included studies in which gentamicin was given as part of a treatment regimen in combination with other antibiotics. Thirdly, their definition of gonorrhoea was limited to participants with uncomplicated urogenital infection and diagnosis was restricted to urethral or cervical culture at the time of treatment and follow-up.
Our data supports the conclusion that gentamicin may not achieve the 95% cure rate recommended by the World Health Organization for empirical therapy. However, the risk of bias within available studies limits any firm conclusions being drawn and a potential role for gentamicin as an alternative or adjunctive agent remains and merits evaluation in randomised trials. Preliminary data from an American study examining the effectiveness of gentamicin with azithromycin recently suggested high efficacy (202/202 negative culture at 10–17 days post treatment) but poor tolerability of this regimen (27.7% reporting nausea and 47% any gastrointestinal disturbance) [38]. Also, this study did not determine the efficacy of the individual antibiotics, or efficacy of gentamicin for extra-genital infections, and further randomised control trials incorporating currently recommended antibiotic regimens, comparing different gentamicin doses and correlating in vitro gentamicin susceptibilities to clinical response are needed.
A comprehensive review of the literature was performed with all relevant identified articles obtained and translated. Few studies met the inclusion criteria with limited numbers of patients receiving single-dose intramuscular gentamicin. The five studies included for data extraction were performed in Malawi, Zambia, Egypt, Korea and Saudi Arabia, and their findings may not be applicable to other settings where first-line treatment regimens and gentamicin susceptibility may differ. No studies of genital infection in women or non-genital gonorrhoea infection were identified by the search strategy, and the findings cannot be extrapolated to these groups.
Quality of included studies
Two of the identified studies were very small with 20 [35] and 30 [33] patients receiving gentamicin. The comparator antibiotic varied across the included studies, and all were suboptimal when compared to current UK management guidelines. Two studies were described as randomised control trials, but none adequately described their method of generating a random allocation sequence, method of concealment or blinding to the allocation schedule. In addition, differences in definition of gonococcal infection, gentamicin dosing, comparator antibiotic, evaluation of re-infection and definition and timing of cure meant that it was inappropriate to pool data for meta-analysis.
Conclusions
Based on current evidence, there are insufficient data to support or reject a recommendation for inclusion of single-dose gentamicin as a first-line agent in the treatment of uncomplicated gonorrhoea infection. Further high-quality RCTs incorporating currently recommended antibiotic regimens with laboratory measurement of gentamicin MIC are needed to inform a change in clinical practice.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
EH and DD conducted the review and writing of the manuscript. LD reviewed the protocol, gave statistical advice and reviewed the manuscript. JDCR contributed to the initial concept and reviewed and revised the manuscript. All authors read and approved the final manuscript.
Supplementary Material
Search strategy. Search strategy used to identify studies for inclusion in the review.
Risk of bias assessment. Summary of the risk of bias in each included study.
PRISMA statement. Checklist against PRISMA guidelines for the reporting of systematic reviews.
Contributor Information
Emma Hathorn, Email: emma.hathorn@nhs.net.
Divya Dhasmana, Email: divya.dhasmana@uhb.nhs.uk.
Lelia Duley, Email: lelia.duley@nottingham.ac.uk.
Jonathan DC Ross, Email: jonathan.ross@uhb.nhs.uk.
References
- Health Protection England. Sexually transmitted infections and chlamydia screening in England 2012. Health Prot Rep. 2013;7(23):8–21. [Google Scholar]
- World Health Organization. Global incidence and prevalence of selected curable sexually transmitted infections, 2008. [ http://www.who.int/reproductivehealth/publications/rtis/stisestimates/en/]
- Aghaizu A, Adams EJ, Turner K, Kerry S, Hay P, Simms I, Oakeshott P. What is the cost of pelvic inflammatory disease and how much could be prevented by screening for Chlamydia trachomatis? Cost analysis of the Prevention of Pelvic Infection (POPI) trial. Sex Transm Infect. 2011;87(4):312–317. doi: 10.1136/sti.2010.048694. [DOI] [PubMed] [Google Scholar]
- Yeh JM, Hook EW, Goldie SJ. A refined estimate of the average lifetime cost of pelvic inflammatory disease. Sex Transm Dis. 2003;30(5):369–378. doi: 10.1097/00007435-200305000-00001. [DOI] [PubMed] [Google Scholar]
- Venkatesh KK, van der Straten A, Cheng H, Cheng H, Montgomery ET, Lurie MN, Chipato T, Ramjee G, Blanchard K, Padian NS, Mayer KH, de Bruyn G. The relative contribution of viral and bacterial sexually transmitted infections on HIV acquisition in southern African women in the methods for improving reproductive health in Africa study. Int J STD AIDS. 2011;22(4):218–224. doi: 10.1258/ijsa.2010.010385. [DOI] [PubMed] [Google Scholar]
- Watson-Jones D, Baisley K, Weiss HA, Tanton C, Changalucha J, Everett D, Chirwa T, Ross D, Clayton T, Hayes R. Risk factors for HIV incidence in women participating in an HSV suppressive treatment trial in Tanzania. AIDS. 2009;23(3):415–422. doi: 10.1097/QAD.0b013e32831ef523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pathela P, Braunstein S, Blank S, Schillinger J. HIV incidence and time to diagnosis among men with bacterial rectal infections, New York City. Sex Transm Infect. 2011;87(Suppl 1):A184. [Google Scholar]
- Cohen MS, Hoffman IF, Royce RA, Kazembe P, Dyer JR, Daly CC, Zimba D, Vernazza PL, Maida M, Fiscus SA, Eron JJ Jr. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1: AIDSCAP Malawi Research Group. Lancet. 1997;349(9069):1868–1873. doi: 10.1016/S0140-6736(97)02190-9. [DOI] [PubMed] [Google Scholar]
- Ghys PD, Fransen K, Diallo MO, Ettiègne-Traoré V, Coulibaly IM, Yeboué KM, Kalish ML, Maurice C, Whitaker JP, Greenberg AE, Laga M. The associations between cervicovaginal HIV shedding, sexually transmitted diseases and immunosuppression in female sex workers in Abidjan. Cote d’Ivoire AIDS. 1997;11(12):F85–F93. doi: 10.1097/00002030-199712000-00001. [DOI] [PubMed] [Google Scholar]
- Levine WC, Pope V, Bhoomkar A, Tambe P, Lewis JS, Zaidi AA, Farshy CE, Mitchell S, Talkington DF. Increase in endocervical CD4 lymphocytes among women with nonulcerative sexually transmitted diseases. J Infect Dis. 1998;177(1):167–174. doi: 10.1086/513820. [DOI] [PubMed] [Google Scholar]
- HPA Guidance for gonorrhoea testing in England and Wales, 2010. [ http://www.bashh.org/BASHH/Guidelines/Guidelines/BASHH/Guidelines/Guidelines.aspx]
- Bignell C. European (IUSTI/WHO) guideline on the diagnosis and treatment of gonorrhoea in adults. Int J STD AIDS. 2009;20(7):453–457. doi: 10.1258/ijsa.2009.009160. [DOI] [PubMed] [Google Scholar]
- Smith DW, Tapsall JW, Lum J. Guidelines for the use and interpretation of nucleic acid detection tests for Neisseria gonorrhoea in Australia: a position paper on behalf of the Public Health Laboratory Network. [ http://www.health.gov.au/internet/main/publishing.nsf/Content/cda-cdi2904-pdf-cnt.htm/$FILE/cdi2904b.pdf] [DOI] [PubMed]
- CDC Sexually Transmitted Diseases Guidelines, 2010: gonococcal infections. [ http://www.cdc.gov/std/treatment/2010/gonococcal-infections.htm]
- World Health Organization. Guidelines for the management of sexually transmitted diseases. [ http://www.who.int/hiv/pub/sti/en/STIGuidelines2003.pdf]
- Bignell C, FitxGerald M. UK national guideline for the management of gonorrhoea in adults, 2011. [ http://www.bashh.org/BASHH/Guidelines/Guidelines/BASHH/Guidelines/Guidelines.aspx] [DOI] [PubMed]
- Government of South Australia, Communicable Disease Control Branch. Revision of treatment guidelines for uncomplicated gonorrhoea. [ http://www.health.wa.gov.au/diseasewatch/vol17_issue3/gonorrhoeae-treatment.cfm]
- European Centre for Disease Prevention and Control. Response plan to control and manage the threat of multi-drug resistant gonorrhoea in Europe. [ http://www.ecdc.europa.eu/en/publications/Publications/1206-ECDC-MDR-gonorrhoea-response-plan.pdf]
- HPA GRASP 2010 Report. [ http://webarchive.nationalarchives.gov.uk/20140714084352/http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1316016752917]
- CDC 2010 STD Surveillance Report: Gonorrhoea. [ http://www.cdc.gov/std/stats10/gonorrhea.htm]
- Ohnishi M, Golparian D, Shimuta K, Saika T, Hoshina S, Iwasaku K, Nakayama S, Kitawaki J, Unemo M. Is Neisseria gonorrhoeae initiating a future era of untreatable gonorrhea?: detailed characterization of the first strain with high-level resistance to ceftriaxone. Antimicrob Agents Chemother. 2011;55(7):3538–3545. doi: 10.1128/AAC.00325-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Unemo M, Golparian D, Nicholas R, Ohnishi M, Gallay A, Sednaoui P. High-level cefixime- and ceftriaxone-resistant Neisseria gonorrhoeae in Europe (France): novel penA mosaic allele in a successful international clone causes treatment failure. Antimicrob Agents Chemother. 2012;56(3):1273–1280. doi: 10.1128/AAC.05760-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carnicer-Pont D, Smithson A, Fina-Homar E, Bastida MT. First cases of Neisseria gonorrhoeae resistant to ceftriaxone in Catalonia, Spain, May 2011. Enferm Infecc Microbiol Clin. 2012;30(4):218–219. doi: 10.1016/j.eimc.2011.11.010. [DOI] [PubMed] [Google Scholar]
- Ameyama S, Onodera S, Takahata M, Minami S, Maki N, Endo K, Goto H, Suzuki H, Oishi Y. Mosaic-like structure of penicillin-binding protein 2 gene (penA) in clinical isolates of Neisseria gonorrhoeae with reduced susceptibility to cefixime. Antimicrob Agents Chemother. 2002;46(12):3744–3749. doi: 10.1128/AAC.46.12.3744-3749.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ito M, Deguchi T, Mizutani KS, Yasuda M, Yokoi S, Ito S, Takahashi Y, Ishihara S, Kawamura Y, Ezaki T. Emergence and spread of Neisseria gonorrhoeae clinical isolates harboring mosaic-like structure of penicillin-binding protein 2 in Central Japan. Antimicrob Agents Chemother. 2005;49(1):137–143. doi: 10.1128/AAC.49.1.137-143.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanaka M, Nakayama H, Huruya K, Konomi I, Irie S, Kanayama A, Saika T, Kobayashi I. Analysis of mutations within multiple genes associated with resistance in a clinical isolate of Neisseria gonorrhoeae with reduced ceftriaxone susceptibility that shows a multidrug-resistant phenotype. Int J Antimicrob Agents. 2006;27(1):20–26. doi: 10.1016/j.ijantimicag.2005.08.021. [DOI] [PubMed] [Google Scholar]
- Brown LB, Krysiak R, Kamanga G, Mapanje C, Kanyamula H, Banda B, Mhango C, Hoffman M, Kamwendo D, Hobbs M, Hosseinipour MC, Martinson F, Cohen MS, Hoffman IF. Neisseria gonorrhoeae antimicrobial susceptibility in Lilongwe, Malawi, 2007. Sex Transm Dis. 2010;37:169–172. doi: 10.1097/OLQ.0b013e3181bf575c. [DOI] [PubMed] [Google Scholar]
- Lule G, Behets FM, Hoffman IF, Dallabetta G, Hamilton HA, Moeng S, Liomba G, Cohen MS. STD/HIV control in Malawi and the search for affordable and effective urethritis therapy: a first field evaluation. Genitourin Med. 1994;70(6):384–388. doi: 10.1136/sti.70.6.384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chisholm SA, Quaye N, Cole MJ, Fredlund H, Hoffmann S, Jensen JS, van de Laar MJ, Unemo M, Ison CA. An evaluation of gentamicin susceptibility of Neisseria gonorrhoeae isolates in Europe. J Antimicrob Chemother. 2011;66(3):592–595. doi: 10.1093/jac/dkq476. [DOI] [PubMed] [Google Scholar]
- Hathorn E, Dhasmana D, Dule L, Ross J, Harding J. The effectiveness of gentamicin in the treatment of Neisseria gonorrhoeae: a systematic review. PROSPERO: International Prospective Register of Systematic Reviews. 2012: CRD42012002490. [ http://www.crd.york.ac.uk/NIHR_PROSPERO/] [DOI] [PMC free article] [PubMed]
- The Cochrane Collaboration. Chapter 8: Assessing risk of bias included studies. [ http://handbook.cochrane.org/]
- Dreyer NA, Velentgas P, Westrich K, Dubois R. The GRACE checklist for rating the quality of observational studies of comparative effectiveness: a tale of hope and caution. JMCP. 2014;20(3):301–308. doi: 10.18553/jmcp.2014.20.3.301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iskandar IO, Nahuib F, Gabry L EL. A comparative study of gentamicin, co-trimoxazole and trimethoprim-sulphametrol in acute gonococcal urethritis. J Egypt Med Assoc. 1978;61:489–495. [PubMed] [Google Scholar]
- Yoon JY, Kim YT, Kim JH. Treatment of uncomplicated male gonococcal urethritis: kanamycin vs. gentamicin. Korean J Dermatol. 1988;26(2):184–188. [Google Scholar]
- Pareek SS, Chowdhury MNH. Comparative study between gentamicin and spectinomycin in the treatment of infections to penicillin-resistant gonococci. Curr Ther Res. 1981;30(2):177–180. [Google Scholar]
- Hira SK, Attili VR, Kamanga J, Mkandawire O, Patel JS, Patel MI. Efficacy of gentamicin and kanamycin in the treatment of uncomplicated gonococcl urethritis in Zambia. Sex Transm Dis. 1985;12(1):52–54. doi: 10.1097/00007435-198501000-00011. [DOI] [PubMed] [Google Scholar]
- Dowell D, Kirkcaldy RD. Effectiveness of gentamicin for gonorrhoea treatment: systematic review and meta-analysis. Sex Transm Inf. 2012;88:589–594. doi: 10.1136/sextrans-2012-050604. [DOI] [PubMed] [Google Scholar]
- Kirkcaldy RD. Treatment of gonorrhoea in an era of emerging cephalosporin resistance and results of a randomised trial of new potential treatment options. Sex Transm Infect. 2013;89:A14–A15. doi:10.1136/sextrans-2013-051184.0043. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy. Search strategy used to identify studies for inclusion in the review.
Risk of bias assessment. Summary of the risk of bias in each included study.
PRISMA statement. Checklist against PRISMA guidelines for the reporting of systematic reviews.