

Abstract
Background
The immune thrombocytopenia (ITP) criteria were newly standardized by the International Working Group. Thus, we analyzed the natural course of childhood chronic ITP to predict the prognosis based on the revised criteria.
Methods
The medical records of children with chronic ITP from May 2000 to February 2013 in our institute were reviewed.
Results
Forty-seven children with chronic ITP who were not undergoing corticosteroid therapy were included. Their initial platelet count was 23±25×109/L, and age at diagnosis was 6.3±4.1 years. The follow-up period was 5.4±3.7 years. Among them, 44.7% (21/47) showed spontaneous remission and maintained a platelet count ≥100×109/L. And 66.0% (31/47) maintained a platelet count ≥50×109/L until the last follow-up date. The time periods required for the platelet count to be maintained ≥50×109/L and ≥100 ×109/L were 3.1±2.7 and 3.6±2.7 years. Age at diagnosis in the ≥50×109/L group (5.7±4.4 years) was significantly lower than the age at diagnosis in the <50×109/L group (7.4±3.3 years) (P=0.040). And follow-up period was the factor influencing prognosis between the ≥100×109/L group and <50×109/L group (P=0.022).
Conclusion
Approximately 45% of children with chronic ITP recovered spontaneously about 3-4 years after the diagnosis and 2/3 of patients maintained a platelet count ≥50×109/L, relatively safe state. Age at diagnosis of ITP and follow-up period were the factors influencing prognosis in this study.
Keywords: Chronic immune thrombocytopenia, Prognosis, Children
INTRODUCTION
Childhood immune thrombocytopenia (ITP) is a disorder with a favorable prognosis characterized by accelerated destruction of antibody-sensitized platelets by the reticuloendothelial system and the presence of isolated thrombocytopenia in peripheral blood [1, 2]. However, about 30% of children with ITP have a chronic persistent course [3]. In Korea, 37% of children with ITP in a multicenter study had persistent ITP ≥6 months [4] and 22.5-28.7% in single institute [5, 6].
The ITP criteria were newly standardized by the International Working Group (IWG) [7]. According to the IWG revised terminology, the term "purpura" is not appropriate due to the absence or minimal hemorrhagic symptoms in many patients with ITP. Thus, ITP (previously immune/idiopathic thrombocytopenic purpura) is now recommended to be called immune thrombocytopenia. The threshold for diagnosing ITP was established as a peripheral platelet count <100×109/L (previously, <150×109/L). The definition of "chronic" is reserved for a low platelet count persisting for ≥12 months (previously, ≥6 months). Evim et al. reported long-term follow-up data of childhood ITP in Turkey according to the newly revised ITP criteria by the IWG [8].
The percentage of spontaneous remission in childhood chronic ITP (lasting more than 6 months) is 46.9% in Korea, and maintenance therapy with a corticosteroid is one of the factors influencing recovery [9]. However, no data are available on the course of Korean childhood chronic ITP without maintenance therapy or splenectomy based on the new IWG criteria. Thus, in this study, we applied the newly standardized definition and analyzed the natural course of childhood chronic ITP after long-term follow-up.
MATERIALS AND METHODS
Inclusion and exclusion criteria
Children with chronic ITP persisting ≥12 months after diagnosis were included by reviewing the medical records at Kyungpook National University Hospital from May 2000 to February 2013. We excluded patients who had secondary causes of thrombocytopenia such as HIV infection, systemic lupus erythematosus, hepatitis, aplastic anemia, hematological malignancy, or von Willebrand disease.
Classification of children with chronic ITP based on spontaneous remission of platelet count
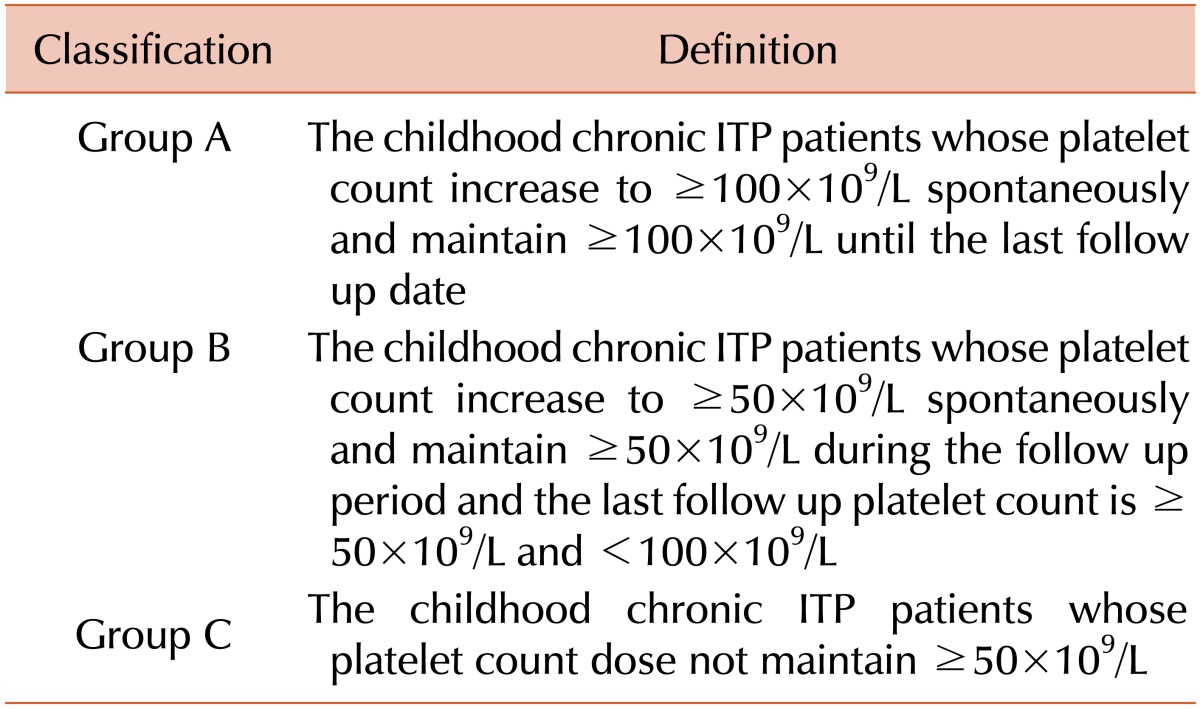
We intended to determine when the platelet count spontaneously recovered to ≥50×109/L and ≥100×109/L. The criterion of a 50×109/L platelet count followed the general consensus that patients with <50×109/L platelets may require on-demand therapy in the case of major bleeding, trauma, or for invasive procedures [7]. The criterion of a platelet count ≥100×109/L followed the revised definition of ITP by the IWG [7]. We divided the subjects into three groups according to Table 1.
Table 1.
Classification of children with chronic immune thrombocytopenia according to spontaneous increase of platelet count.
Statistical analysis
Statistical analyses were performed using SPSS ver. 21.0 software (SPSS, Inc., Chicago, IL, USA). Data are presented as means±standard deviations. The Kruskal-Wallis test and Mann-Whitney U-test with a Bonferroni adjustment were used to compare the subjects' variables between the groups. Logistic regression analysis was performed to find out the factors influencing prognosis. Linear by linear association with the chi-square test was used for the gender ratio comparison between the groups. Spearman's correlation analyses were used to define the correlation between the patients' variables and the time required for the platelet count to recover spontaneously. Absolute correlation coefficient rho values >0.3 and P values<0.05 were considered significant.
RESULTS
Subject characteristics
Forty-seven children with ITP (male:female=26:21) who were not undergoing maintenance therapy with a corticosteroid in the past three months or who did not undergo a splenectomy from May 2000 to February 2013 at our institute were included. There were 20 patients who had treated with corticosteroid. There was no pediatric patient who underwent splenectomy during study period. The initial platelet count was 23±25×109/L, and age at diagnosis was 6.3±4.1 years. The follow-up period was 5.4±3.7 years, and the last follow-up platelet count was 102±103×109/L.
Ratio of spontaneous remission
A total of 44.7% (21/47) showed spontaneous remission and maintained a platelet count ≥100×109/L (Group A). And 66.0% (31/47) maintained a platelet count ≥50×109/L until the last follow-up date and didn't need any on-demand therapy (Group A+B). All cases of spontaneous increase of platelet count were observed without any medication at least three months. The subjects' variables in accordance with the increase of platelet count are shown in Table 2.
Table 2.
Characteristics of the children with chronic immune thrombocytopenia according to spontaneous increase of platelet count.

Comparison of the subject's variables between the groups
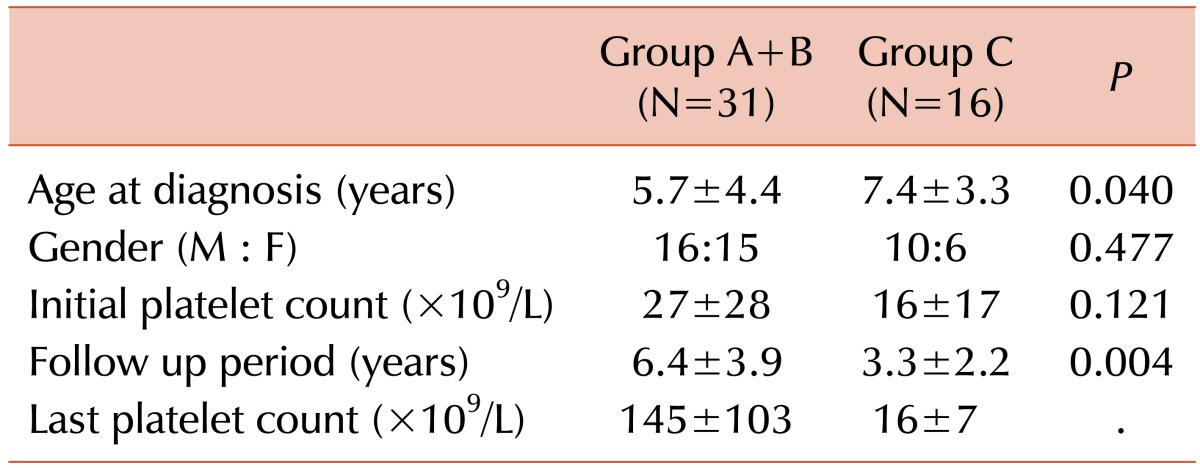
No differences in patients' age at diagnosis, gender ratio and initial platelet count were observed between the three groups. A statistically significant difference in follow-up period was observed between the three groups (P =0.028). There was difference between Group A and C (P =0.024), not between Group A/B (P =1.000) or Group B/C (P =0.291) by post hoc. By logistic regression analysis, follow-up period was the factor influencing the prognosis (P =0.022) between Group A and C. The subjects' variables and P values are shown in Table 2. When we divided the subjects into Group A + B and Group C with a 50×109/L platelet count, significant differences in patient age at diagnosis and follow-up period were observed (P =0.040 and P =0.004, respectively). No differences in gender ratio or initial platelet count were observed. The subjects' variables and P values when we divided the subjects into two groups are shown in Table 3.
Table 3.
Characteristics of children with chronic immune thrombocytopenia and P values when the patients were divided into two groups, Group A+B and Group C with a 50×109/L spontaneous increase of platelet count.
Time required for platelet count maintain ≥50×109/L and ≥100×109/L without medication
This analysis was targeted on the chronic ITP children whose initial platelet count was <50×109/L. The time periods required for platelet counts to recover to ≥50×109/L and ≥100×109/L were 3.1±2.7 years and 3.6±2.7 years, respectively in Group A patients whose initial platelet count was <50×109/L (N=17). The period between the points when platelet count reached ≥50×109/L and ≥100×109/L was 0.5±0.5 years. The progress of spontaneous remission of platelet count is shown in Fig. 1. The time for platelet count to recover to ≥50×109/L in Group B whose initial platelet count was <50×109/L (N=8) was 5.4±3.7 years.
Fig. 1.
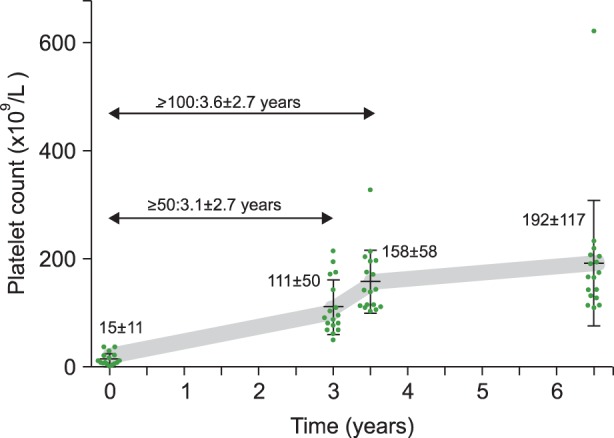
Time required for the platelet count to reach ≥50×109/L and ≥100×109/L in Group A patients whose initial platelet count was <50×109/L (N=17).
Correlation between the subject's variables and the time required for platelet count increase
This analysis was also targeted on the chronic ITP children whose initial platelet count was <50×109/L. No correlation was detected between age at diagnosis of ITP and the duration required for spontaneous increase of platelet count ≥50×109/L in Groups A and B whose initial platelet count was <50×109/L (N=25). No correlation was observed between age at diagnosis and the recovery duration to a platelet count ≥100×109/L in Group A whose initial platelet count was <50×109/L (N=17). Additionally, no correlation was observed between the initial platelet count and the duration required for a platelet count ≥50×109/L in Groups A and B whose initial platelet count was <50×109/L (N=25). No correlation was detected between initial platelet count and the recovery duration to a platelet count ≥100×109/L in Group A whose initial platelet count was <50×109/L (N=17).
DISCUSSION
Several treatment modalities have been used for children with chronic ITP in Korea including splenectomy, corticosteroid, immunoglobulin, cyclosporine, interferon, azathioprine, rituximab, vincristine, danazole, and cepharantin [10, 11, 12, 13, 14]. Although splenectomy is effective and curative for chronic ITP, it should be delayed as long as possible in children due to the possibility of overwhelming sepsis at a young age [15]. Because a certain fraction of children with chronic ITP recover spontaneously, the time when medical personnel decide to perform splenectomy for a patient is critical [15].
In this study, 44.7% of the children with chronic ITP recovered spontaneously using revised IWG criteria. There was not much difference between the result of our study and previous Korean study conducted according to the criteria before revision by the IWG - reported remission percentages of 46.9% [9]. After considering other countries' data, we suppose that approximately 40-50% of chronic ITP children will spontaneously resolve after long-term follow-up [16, 17, 18, 19]. And in this study, 66.0% maintained a platelet count ≥50×109/L, relatively safe state and didn't need on-demand therapy.
In chronic ITP children whose initial platelet count was <50×109/L , the time periods required for the platelet count to increase to ≥50×109/L and ≥100×109/L were mean 3.1 and 3.6 years after diagnosis, respectively. The duration between the time points for a platelet count to be ≥50×109/L and ≥100×109/L was mean 0.5 years in Group A. In other words, once the platelet count increase to ≥50×109/L, the platelet count will reach to ≥100×109/L relatively quickly. While, follow-up period was mean 3.3 years in Group C. This result concluded that every patient in Group C will not spontaneously recover (platelet count ≥100×109/L). Because the follow-up period was mean 6.1 years in Group B, we suggest that some patients in Group C will maintain platelet count ≥50×109/L after longer follow-up. We can consider splenectomy for a minority of patients whose platelet count maintains <50×109/L consistently.
Additionally, the time required to the platelet count to increase to ≥50×109/L was mean 5.4 years in Group B. And there was no statistical difference of follow-up period between Group A and B. This result also concluded that every patient in Group B will not spontaneously recover. We suggest that some patients with unknown underlying disease were included in Group B and C. Thus further evaluation about the underlying cause undiscovered at diagnosis is necessary for Group B or C patients.
Age at diagnosis was the factor influencing the prognosis of children with chronic ITP in this study. This was consistent with the previous study [9]. Age at diagnosis is also a known risk factor related to the development of newly diagnosed ITP to chronic ITP [1, 4].
Some limitations in this study should be discussed. Firstly, no screening for H. pylori was performed. In Korea, 65-92% of adults with chronic ITP and 19% of children with chronic ITP are positive for H. pylori, which is accompanied by H. pylori prevalence in the general population of the same age [20, 21, 22]. Although no increase in platelet count has been reported in Korean children with chronic ITP [22], eradication of H. pylori increased the remission rate of both adult and childhood chronic ITP in several reports [20, 21, 23]. Thus, we are planning an examination and eradication of H. pylori in Groups B and C of this study.
Secondly, no genetic evaluation was concerned. A genetic study is recommended in cases of a family history, treatment failure, persistent moderate thrombocytopenia (≥20×109/L), long-term stable thrombocytopenia, or nonhematological manifestations [24]. Thus, detailed history taking and a genetic evaluation are under consideration for Groups B and C.
Lastly, the correlation between the response to treatment and prognosis of chronic ITP was not evaluated. Because of the various immunoglobulin doses and different treatment modalities for children with chronic ITP at our institute from 2000-2013, quantification of the data was difficult. In this sense, a multicenter prospective study of Korean children with chronic ITP is necessary.
In conclusion, approximately 45% of children with chronic ITP recovered spontaneously about 3-4 years after the diagnosis and 2/3 of patients maintained a platelet count ≥50×109/L after long-term follow-up. Age at diagnosis of ITP and follow-up period were the factors influencing prognosis in this study. We think this study is valuable because it is the first attempt to adopt the new standardized terminology and definition by the IWG for childhood chronic ITP in Korea.
Footnotes
This research was supported by the Kyungpook National University Research Fund, 2012.
No potential conflicts of interest relevant to this article were reported.
References
- 1.Kuhne T, Buchanan GR, Zimmerman S, et al. A prospective comparative study of 2540 infants and children with newly diagnosed idiopathic thrombocytopenic purpura (ITP) from the Intercontinental Childhood ITP Study Group. J Pediatr. 2003;143:605–608. doi: 10.1067/s0022-3476(03)00535-3. [DOI] [PubMed] [Google Scholar]
- 2.Geddis AE, Balduini CL. Diagnosis of immune thrombocytopenic purpura in children. Curr Opin Hematol. 2007;14:520–525. doi: 10.1097/MOH.0b013e3282ab98f2. [DOI] [PubMed] [Google Scholar]
- 3.Kuhne T, Imbach P, Bolton-Maggs PH, Berchtold W, Blanchette V, Buchanan GR. Newly diagnosed idiopathic thrombocytopenic purpura in childhood: an observational study. Lancet. 2001;358:2122–2125. doi: 10.1016/S0140-6736(01)07219-1. [DOI] [PubMed] [Google Scholar]
- 4.Choi EJ, Lee SM, Lee KS, et al. Childhood acute immune thrombocytopenic purpura in Korea - multicenter study of Korean Society of Pediatric Hematology/Oncology. Korean J Pediatr Hematol Oncol. 2003;10:14–21. [Google Scholar]
- 5.Cho YK, Baek HJ, Lim HK, Kook H, Ma JS, Hwang TJ. A clinico-epidemiological study of childhood acute and chronic idiopathic thrombocytopenic purpura. Korean J Pediatr Hematol Oncol. 2005;12:1–10. [Google Scholar]
- 6.Kim UH, Lee SI, Lee KS. Early prediction of chronic childhood immune thrombocytopenic purpura according to the response of immunoglobulin treatment. Clin Pediatr Hematol Oncol. 2013;20:79–85. [Google Scholar]
- 7.Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113:2386–2393. doi: 10.1182/blood-2008-07-162503. [DOI] [PubMed] [Google Scholar]
- 8.Evim MS, Baytan B, Gunes AM. Childhood immune thrombocytopenia: Long-term follow-up data evaluated by the criteria of the International Working Group on Immune Thrombocytopenic Purpura. Turk J Haematol. 2014;31:32–39. doi: 10.4274/Tjh.2012.0049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jung TW, Kwon DH, Jeong DC, Koh DG. Analysis for spontaneous remission of chronic immune thrombocytopenic purpura in children. Clin Pediatr Hematol Oncol. 2011;18:81–85. [Google Scholar]
- 10.Jang GC, Lee YK, Park SH, Lyu CJ, Yang CH, Kim KY. Long-term outcome of chronic childhood idiopathic thrombocytopenic purpura according to therapeutic methods. Korean J Pediatr Hematol Oncol. 2000;7:32–41. [Google Scholar]
- 11.Han HJ, Lee IS, Shin HY, Park ES, Choi HS, Ahn HS. Treatment of chronic idiopathic thrombocytopenic purpura in children with Cepharanthin. Korean J Pediatr Hematol Oncol. 2004;11:26–31. [Google Scholar]
- 12.Hong CH, Park JK, Lee SY. Vincristine effect for the treatment of idiopathic thrombocytopenic purpura in childhood. Clin Pediatr Hematol Oncol. 2007;14:151–158. [Google Scholar]
- 13.Kim MJ, Kim HS, Kwon SY, et al. Role of cyclosporine A in pediatric patients with refractory chronic idiopathic thrombocytopenic purpura. Clin Pediatr Hematol Oncol. 2009;16:1–8. [Google Scholar]
- 14.Kim DJ, Chung JH. Long-term results of laparoscopic splenectomy in pediatric chronic immune thrombocytopenic purpura. Ann Surg Treat Res. 2014;86:314–318. doi: 10.4174/astr.2014.86.6.314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schifferli A, Kuhne T. Chronic immune thrombocytopenia in children: who needs splenectomy? Semin Hematol. 2013;50(Suppl 1):S58–S62. doi: 10.1053/j.seminhematol.2013.03.010. [DOI] [PubMed] [Google Scholar]
- 16.Jayabose S, Levendoglu-Tugal O, Ozkaynkak MF, Visintainer P, Sandoval C. Long-term outcome of chronic idiopathic thrombocytopenic purpura in children. J Pediatr Hematol Oncol. 2004;26:724–726. doi: 10.1097/00043426-200411000-00007. [DOI] [PubMed] [Google Scholar]
- 17.Kubota M, Adachi S, Usami I, et al. Characterization of chronic idiopathic thrombocytopenic purpura in Japanese children: a retrospective multi-center study. Int J Hematol. 2010;91:252–257. doi: 10.1007/s12185-009-0484-1. [DOI] [PubMed] [Google Scholar]
- 18.Kato M, Koh K, Kikuchi A, Hanada R. Spontaneous improvement of chronic immune thrombocytopenia in children: experience of 56 patients at a single institute. Int J Hematol. 2012;96:729–732. doi: 10.1007/s12185-012-1211-x. [DOI] [PubMed] [Google Scholar]
- 19.Rosthoj S, Rajantie J, Treutiger I, Zeller B, Tedgard U, Henter JI. Duration and morbidity of chronic immune thrombocytopenic purpura in children: five-year follow-up of a Nordic cohort. Acta Paediatr. 2012;101:761–766. doi: 10.1111/j.1651-2227.2012.02671.x. [DOI] [PubMed] [Google Scholar]
- 20.Kim BS, Nam SH, Bang SM, et al. The clinical efficacy of Helicobacter pylori eradication in patients with Helicobacter pylori-positive chronic thrombocytopenic purpura. Korean J Hematol. 2005;40:23–27. [Google Scholar]
- 21.Tag HS, Lee HS, Jung SH, et al. Effects of Helicobacter pylori eradication in patients with immune thrombocytopenic purpura. Korean J Hematol. 2010;45:127–132. doi: 10.5045/kjh.2010.45.2.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Park SJ, Baek HJ, Lee SU, et al. Helicobacter pylori infection in children with chronic idiopathic thrombocytopenic purpura. Clin Pediatr Hematol Oncol. 2008;15:83–91. doi: 10.1097/MPH.0b013e3181615600. [DOI] [PubMed] [Google Scholar]
- 23.Russo G, Miraglia V, Branciforte F, et al. Effect of eradication of Helicobacter pylori in children with chronic immune thrombocytopenia: a prospective, controlled, multicenter study. Pediatr Blood Cancer. 2011;56:273–278. doi: 10.1002/pbc.22770. [DOI] [PubMed] [Google Scholar]
- 24.Del Vecchio GC, De Santis A, Accettura L, De Mattia D, Giordano P. Chronic immune thrombocytopenia in childhood. Blood Coagul Fibrinolysis. 2014;25:297–299. doi: 10.1097/MBC.0000000000000043. [DOI] [PubMed] [Google Scholar]