

Abstract
Chronic infection with hepatitis B virus (HBV) leads to the development of hepatocellular carcinoma and/or chronic liver failure. Despite extensive research, the immunopathogenesis is not completely understood. Viral persistence and clinical outcomes following HBV infection depend on viral factors and host factors; including genetic factors that determine a host’s immune mechanisms. The primary goal of chronic hepatitis B (CHB) treatment is to eradicate HBV or to at least maintain suppression of HBV replication. Despite recent advances in anti-viral agents for chronic HBV infection, complete eradication of the virus has been difficult to achieve. Agents for the treatment of CHB are divided mainly into two groups: immunomodulating agents and antiviral nucleos(t)ide analogues (NAs). Although NAs are safe, effective and easily administered orally, their long-term use poses the risk of drug resistance. Currently, international evidence-based guidelines have been developed to support physicians in managing CHB patients. However, treatment of patients with drug resistance is still challenging, as only a few classes of anti-HBV drugs are available and cross-resistance between drugs can occur. In addition, as the currently available genotypic test for detection of drug resistance still has limitations in identifying the different substitutions present in the same viral genome, the development of a new virologic test to overcome this limitation is necessary. Among the predictive factors associated with response to pegylated interferon (PEG-IFN) therapy, hepatitis B surface antigen quantification is considered to be a surrogate marker for monitoring response to PEG-IFN. Current practice guidelines stress the importance of profound and durable HBV viral suppression in the treatment of CHB patients. To this end, it is essential to choose a potent antiviral drug with a low risk of resistance for initial treatment of CHB to achieve sustained virological response. This review highlights recent advances in the understanding of the immunopathogenesis of HBV and currently available and developing treatment strategies against HBV infection.
Keywords: Hepatitis B virus, Chronic hepatitis B, Nucleos(t)ide analogue, Pegylated interferon, Antiviral therapy
Core tip: The primary goal of chronic hepatitis B (CHB) treatment is to eradicate hepatitis B virus (HBV) or to at least maintain suppression of HBV replication. To this end, it is essential to better understand the immunopathogenesis of CHB, although it has yet to be further elucidated. More practically, it is of great importance to choose a potent antiviral drug with a low risk of resistance for initial treatment of CHB to achieve sustained virological response. This review highlights recent advances in the understanding of the immunopathogenesis of HBV and currently available and developing treatment strategies for HBV infection.
INTRODUCTION
Hepatitis B virus (HBV), a member of the family Hepadnaviridae, has a 3.2 kb-partially double-stranded circular DNA genome comprised of 4 open reading frames (ORF) that encode Core proteins (Core and preCore), surface antigen proteins (PreS1, PreS2, and S), reverse transcriptase (Pol protein) and X protein. HBV is a non-cytopathic virus that induces liver damage via immunopathogenesis[1].
Despite the introduction of prophylactic vaccines against HBV in the early 1980s, it is estimated that there are still more than 350 million chronic HBV carriers worldwide[2], a high percentage of whom will eventually develop liver cirrhosis or hepatocellular carcinoma (HCC). The natural history of chronic HBV infection is generally divided into four phases: (1) immune tolerant phase; (2) immune clearance phase; (3) low replicative or inactive carrier stage; and (4) reactivation phase[1,3]. Recent studies have shown that progression to liver cirrhosis and HCC in patients with chronic HBV infection is significantly associated with circulating HBV-DNA levels[4,5]. Thus, antiviral therapy against HBV is critical to prevent the progression to cirrhosis or development of HCC. The primary goal of CHB treatment is to eradicate HBV or to at least maintain a suppressed state of HBV replication. However, antiviral therapy is not recommended for patients in the immune tolerant phase, which is characterized by high HBV-DNA levels with positive hepatitis B e antigen (HBeAg), but normal alanine aminotransferase (ALT) level and minimal necroinflammation. In general, antiviral therapy is considered for patients in the immune clearance phase and the reactivation phase of chronic HBV infection.
Since the introduction of interferon (IFN)-α as the first approved agent for HBV infection in the early 90’s, remarkable advances have been made in the treatment of CHB. Agents for the treatment of CHB are divided mainly into two groups according to their mechanism of action: (1) agents with immunomodulatory and antiviral effects, such as IFN or peglyated IFN (PEG-IFN); and (2) oral nucleos(t)ide analogues (NAs) such as nucleoside analogues including lamivudine (LAM), telbivudine (LdT), clevudine and entecavir (ETV) and nucleotide analogues including adefovir dipivoxil (ADV) and tenofovir dipivoxil fumarate (TDF). These NAs can be divided into sub-classes based on their structural similarities: L-nucleoside analogues (LAM, LdT and Clevudine); alkyl phosphonates (ADV and TDF); and D-cyclopentane (ETV).
The main difference between immunomodulatory agents and NAs is that PEG-IFN has the advantage of a finite duration of use, whereas the use of NA inhibitors is indefinite. The major drawback of PEG-IFN is its high frequency of adverse events. Long-term use of NAs, on the other hand, poses the risk of drug resistance. They are, however, safe, effective and easily administered orally. The number of patients having a virological response after a cycle of IFN therapy is lower compared with patients reaching the suppression of viral replication with new NAs. However, IFN therapy has higher rates of HBeAg seroconversion and hepatitis B surface antigen (HBsAg) loss than NAs. Treatment strategies with PEG-IFN or a NA are intended to achieve a sustained off-treatment virological response. A 48-wk course of PEG-IFN is mainly recommended for HBeAg-positive CHB patients with the best chance of HBeAg seroconversion. It can also be administered in HBeAg-negative CHB patients. Unlike NAs, PEG-IFN potentially offers a chance of sustained off-treatment response after a finite duration of therapy in HBeAg-negative patients. For HBeAg-positive CHB patients, NA therapy can be stopped after additional 12 mo following HBeAg seroconversion, whereas long-term use of NA is needed due to a high rate of off-therapy relapse in HBeAg-negative patients, in whom the ideal end point is HBsAg loss.
LAM, the first approved oral NA for hepatitis B treatment, had been widely used and is a safe and effective drug, however, it has been excluded from most recent international guidelines as a first-line antiviral agent against HBV due to the emergence of drug-induced mutant HBV. The frequency of the development of genotypic resistance was reported to be up to 60%-70% after 5 years of LAM therapy[6,7]. In order to achieve more curative antiviral effects, new therapeutic approaches, such as combination therapies using an antiviral and an immunomodulating agent or multiple antiviral agents used together, have been tried to address this problem, but evidence demonstrating that combination therapy is superior to monotherapy is still lacking[8,9].
The development of a new antiviral agent or optimized therapeutic approaches that can eradicate the virus and not only achieve control of viral replication, should be the focus of future work in the management of CHB. To this end, it is essential to understand the immunopathogenesis of HBV and the mechanisms of viral persistence and drug-induced resistance. The following summarizes recent advances in the understanding of the immunopathogenesis of HBV and currently available and developing optimized antiviral strategies therapies for HBV infection.
IMMUNOPATHOGENESIS
HBV infection in humans results in various clinical outcomes depending on the age of the patient at the time of infection: 90% of individuals infected via vertical or perinatal transmission develop chronically evolving hepatitis, while 90% of individuals infected via horizontal transmission during adulthood recover[1]. Viral persistence and clinical outcomes following HBV infection depend on viral factors and host factors; including genetic factors that determine a host’s immune mechanisms[10].
The innate immune response controls initial infection during the early phases of viral infection. Various components, such as natural killer (NK) cells, natural killer T (NKT) cells, dendritic cells, cytokines, chemokines and toll-like receptor (TLR) contribute to this nonspecific innate immune response[11]. Type 1 IFNs produced by infected cells also play an important role in the inhibition of viral replication early on, but do not provide long-term protective immunity against viruses[11]. Dysfunction of the innate immune response in the immune tolerant phase may be explained by previous studies which showed that HBV suppress TLR-mediated innate immune responses in murine non-parenchymal liver cells[12] and HBeAg reduces TLR2 expression on hepatocytes, Kupffer cells (KCs) and peripheral monocytes in patients with CHB[13]. On the other hand, in the immune clearance phase, NK cell activation induces tumor necrosis factor (TNF)-related apoptosis-inducing ligand (TRAIL)-mediated death of hepatocytes in CHB, leading to liver injury[14]. Interestingly, a recent study by Zhang et al[15] demonstrated that peripheral CD16+ monocytes in chronic HBV infection are selectively recruited into the liver, where they are highly activated and produce pro-inflammatory cytokines and induce Th17 cells to initiate destructive immune responses.
Major histocompatibility complex (MHC) class-I restricted CD8+ T-cells and MHC class-II restricted CD4+ T-cells have been shown to play key roles in the adaptive cellular immune response against HBV. Studies have shown that individuals who demonstrated spontaneous recovery from HBV infection mount a vigorous, multi-specific T-cell response against HBV antigens. Chronic HBV carriers mount a defective T-cell response, which is characteristically weak and mono-specific, and go on to develop chronic liver diseases such as liver cirrhosis and HCC[16,17]. CD8+ T cells cause the lysis of HBV-infected hepatocytes through cytolytic and non-cytolytic mechanisms[18]. The cytolytic mechanism was demonstrated in HBV-transgenic mouse models that express HBV antigens in the liver[19,20]. These transgenic mice are tolerant of self-HBV antigens, and notable liver damage does not develop. However, when cytotoxic T-cells from one of these transgenic mice are introduced into syngenic mice, significant acute liver injury that resembles acute hepatitis B in humans occurs[21]. The lysis of HBV-infected hepatocytes occurs via perforin or Fas systems which lead to viral clearance. Non-cytolytic mechanisms are mediated by some specific cytokines, such as IFN-γ and tumor necrosis factor (TNF)-α which selectively degrade replicating genomes of HBV without killing infected cells[21,22]. Since HBV is a non-cytopathic virus, it must be able to either evade or overwhelm anti-viral immune responses. Most neonates who are infected via vertical transmission from their mothers develop chronically evolving hepatitis through neonatal tolerance. Explanations for this neonatal tolerance involve the immature immune system of neonates and the immunomodulating effects of excessively secreted HBeAg in peripheral blood. This tolerating effect of HBeAg has been well demonstrated in HBV transgenic mice[23]. In addition, studies have shown that cytotoxic T cell responses in patients with chronic HBV infection occur less vigorously than those with acute hepatitis B, even if they have a high viral load in the peripheral blood[16]. This low cytotoxic T cell response is responsible for the induction of peripheral tolerance or the exhaustion of the T cell response due to a high viral load[24]. Moreover, antigen persistence is a major factor driving the functional alteration of HBV-specific T cells, and thus antigen removal to allow T cell resting can be an essential requirement for the functional reconstitution of antiviral T cell responses[25]. The hyporesponsiveness of HBV-specific CD8+ T cells results in decreased cytotoxicity, proliferation, and production of anti-viral cytokines; including TNF-α and interleukin-2 (IL-2), which are responsible for eradicating the virus during chronic infection[26,27]. In addition to HBV-specific T cells, NK cells, NKT and macrophages can inhibit HBV replication by producing IL-12 and nitric oxide[28]. The other factors influencing HBV-specific tolerance include the immunoregulatory effects of CD4+ CD25+ FoxP3+ regulatory T cells (Tregs) and the dysfunction of dendritic cells[29]. Tregs suppress effector T cells, which impair the immune response. Thus, a change in number or function could cause a decrease in anti-viral immunity in chronic HBV carriers. Studies on the frequency of circulating Tregs in chronic HBV carriers have yielded conflicting results-both increased[30] and decreased[31] frequencies have been observed. However, depletion of Tregs increased the function of HBV specific T-cells, even though such modulation was not necessarily HBV-specific[30,31]. Hence, the role of Tregs in the immunopathogenesis of HBV should be further clarified.
Although the immunomodulatory effect of chronic HBV infection on dendritic cell function is poorly understood, recent studies suggest that dysfunction of dendritic cells may contribute to inhibition of the anti-viral immune response, leading to viral persistence and progressive liver disease in chronic HBV carriers[32]. In addition, recent studies have shown that the programmed death-1 (PD-1) inhibitory receptor is involved in the impairment of virus-specific CD8 T-cell function in chronic viral infections in mice and humans[33,34]. Little data is available on the association between PD-1 expression and HBV-specific CD8+ T cells, but a recent study has demonstrated that the increase in HBV-specific CD8+ T cell proliferation correlates with the downregulation of PD-1[35]. Based on these experiments, it can be surmised that blocking the activation of PD-1 can restore exhausted virus-specific CD8+ T cells and thus lead to a promising strategy for treating chronic HBV infection. Cytotoxic T cells play a crucial role in controlling viral replication, but selection for viral escape mutations in targeted T-cell epitopes may limit their effectiveness. However, viral escape mutants in HBV have rarely been reported, even in cases of CHB[36], with the exception of a few reports which demonstrated that viral mutations abrogate, energize or antagonize antigen recognition by virus-specific T cells[37,38]. Other possible mechanisms leading to HBV persistence include the infection of immunologically privileged sites, viral inhibition of antigen presentation and downregulation of viral gene expression[24]. The immune responses against HBV and its regulation are summarized in Figure 1.
Figure 1.
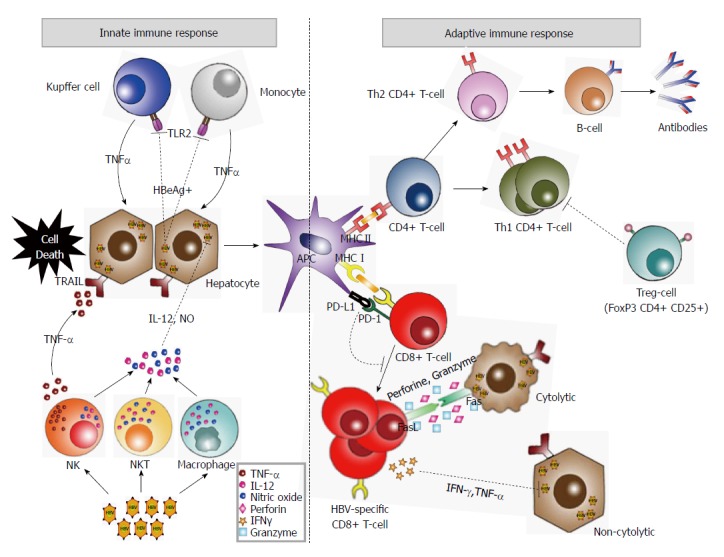
Summary of the innate immune response and cellular immune response against hepatitis B virus. Natural killer (NK) cells, natural killer T (NKT) cells, dendritic cells, cytokines, chemokines and toll-like receptor (TLR) contribute to the innate immune response against hepatitis B virus (HBV). Also, NK cells, NKT and macrophages can inhibit HBV replication by producing interleukin (IL)-12 and nitric oxide. Dysfunction of the innate immune response in the immune tolerant phase may be explained by this process. However, HBeAg reduces TLR2 expression on hepatocytes, Kupffer cells and peripheral monocytes. Moreover, NK cell activation induces TRAIL-mediated death of hepatocytes in CHB, leading to liver injury. Chronic HBV carriers mount a defective T-cell response. CD8+ T cells cause the lysis of HBV-infected hepatocytes through cytolytic and non-cytolytic mechanisms. Non-cytolytic mechanisms are mediated by some specific cytokines, such as interferon (IFN)-γ and tumor necrosis factor (TNF)-α which selectively degrade replicating genomes of HBV without killing infected cells. In CHB, Tregs suppress effector T cells, which impair the cellular immune response. The programmed death-1 (PD-1) inhibitory receptor is involved in the impairment of virus-specific CD8 T-cell function.
UPDATE ON THE TREATMENT OF CHRONIC HEPATITIS B
The ultimate goal of antiviral therapy for CHB is to prevent progression to cirrhosis or HCC via eradication of HBV or persistent viral suppression. The ideal end point of antiviral therapy is the achievement of either HBsAg seroconversion or HBsAg loss. Therefore, antiviral treatment is recommended for patients with chronic HBV infection who are at risk of developing liver failure or for those with advanced liver diseases[39,40]. Regional clinical practice guidelines for the treatment of patients with chronic HBV infection have recently been developed and updated: American Association for the Study of Liver Disease (AASLD) in 2009[40], The Asian Pacific Association for the Study of the Liver (APASL) in 2012[39] and European Association for the Study of the Liver (EASL) in 2012[41]. In deciding upon an appropriate treatment plan for patients with chronic HBV infection, careful consideration must be given to the degree of liver disease, laboratory data, including biochemical and viral levels, histological findings and patient compliance. Although recommendations for the management of chronic HBV infection are similar between regional guidelines, there are some differences regarding the levels of HBV-DNA and ALT, examination of liver biopsy prior to treatment for CHB and liver cirrhosis (Table 1). Among currently available antiviral agents including the standard IFN, PEG-IFN, LAM, ADV, LdT, ETV, TDF and clevudine, PEG-IFN-based therapy, ETV and TDF are recommended for naïve patients with CHB according to the regional guidelines. For patients with liver cirrhosis, however, AASLD guidelines recommend ETV, TDF or the combination of LAM (or LdT) and ADV, while EASL and APASL guidelines recommend ETV and TDF for decompensated liver cirrhosis, and to consider IFN-based therapy for compensated liver cirrhosis. On the other hand, antiviral therapy is not recommended for patients in the immune tolerant phase or the inactive carrier state as disease progression is rare in these phases, and treatment would induce an undue risk of developing drug resistance in such patients.
Table 1.
Indications for treatment and recommended strategy for chronic hepatitis B
| AASLD 2009 | EASL 2012 | APASL 2012 | ||
| HBeAg positive hepatitis | Indications for treatment | HBV DNA > 20000 IU/mL and ALT > 2 × ULN | HBV DNA > 2000 IU/mL and ALT > ULN | HBV DNA > 20000 IU/mL and ALT > 2 × ULN |
| Biopsy recommended1 | HBV DNA >20000 IU/mL and ALT 1-2 × UNL especially if age > 40 yr or family history of HCC | HBV DNA > 2000 IU/mL and Age > 30 yr or family history of HCC | HBV DNA > 20000 IU/mL or high normal or minimally raised ALT and age > 40 yr | |
| Preferred drugs for naïve patients | PEG-IFN, ETV, TDF | PEG-IFN, ETV, TDF | IFN-based therapy, ETV, TDF | |
| HBeAg negative hepatitis | Indications for treatment | HBV DNA >20000 IU/mL2 and ALT > 2 × ULN | HBV DNA > 2000 IU/mL and ALT > ULN | HBV DNA > 2000 IU/mL and ALT > 2 × ULN |
| Biopsy recommended1 | HBV DNA >2000 IU/mL and ALT 1- > 2 × UNL | Unmentioned | HBV DNA > 2000 IU/mL or high normal or minimally raised ALT and age > 40 yr | |
| Preferred drugs for naïve patients | PEG-IFN, ETV, TDF | PEG-IFN, ETV, TDF | IFN-based therapy, ETV, TDF | |
| Liver cirrhosis | Indication for treatment | Compensated: HBV DNA >2000 IU/mL; consider treating HBV < 2000 IU/mL if ALT > UNL Decompensated: any detectable HBV DNA | Any detectable HBV DNA | Compensated: HBV DNA > 2000 IU/mL Decompensated: any detectable HBV DNA |
| Preferred drugs for naïve patients | Combination of LAM (or LDT) and ADV, ETV, TDF | Compensated: PEG-IFN, ETV, TDF Decompensated: ETV, TDF | ETV, TDF (consider also IFN-based therapy if compensated LC and ALT < 5 × UNL) |
Consider treatment if moderate to severe inflammation or significant fibrosis is shown on liver biopsy; noninvasive methods may be useful in EASL and APASL guidelines;
Treatment may be considered in patients with HBV DNA 2000-20000 IU/mL, particularly if they are older or have cirrhosis.AASLD: The American Association for the Study of the Liver Diseases; EASL: European Association for the Study of the Liver; APASL: The Asian Pacific Association for the Study of the Liver; ULN: Upper limit of normal; PEG-IFN: Pegylated interferon; ETV: Entecavir; TDF: Tenofovir; IFN: Interferon; LAM: Lamivudine; LDT: Telbivudine; ADV: Adefovir.
Pegylated interferon
The most important advantage of PEG-IFN use in clinical practice is finite duration of treatment. In addition, the antiviral response is more durable with higher HBeAg seroconversion and HBsAg seroconversion after treatment compared with NAs. However, frequent adverse events, low degree of compliance due to injection-related problems[41] such as flu-like symptoms, neutropenia, thrombocytopenia, decreased appetite, abdominal discomfort, rash, pruritus, alopecia, thyroiditis, injection-site reaction and depression, and high costs are considered to be some of its drawbacks. Although PEG-IFN does not result in marked DNA suppression during treatment, it has shown to induce delayed post-treatment anti-viral benefits. In two randomized clinical trials (RCT) investigating the efficacy and safety of PEG-IFN-α-2a in HBeAg positive CHB patients, the HBeAg seroconversion rate at the end-of-treatment was approximately 30% of cases. This virological response increased during the period of follow-up, reflecting post-treatment delayed immune responses[42,43]. In addition, 83% of patients who achieved seroconversion during treatment or early post-treatment had a sustained response at 12 mo post-treatment[43]. Decreasing the viral load by NA treatment prior to an immune modulator may be a rational strategy to achieve a more effective viral response given that simultaneous combination therapies have not shown a superior viral response. However, in both of the above-mentioned RCTs, simultaneous combination therapy with PEG-IFN-α-2a plus LAM was not superior to monotherapy with PEG-IFN-α-2a. Previous clinical studies on the antiviral efficacy of LAM followed by PEG-IFN therapy compared with placebo followed by PEG-IFN in HBeAg-positive CHB patients demonstrated that sequential therapy of LAM and PEG-IFN improved sustained virological response as compared with the control group[44]. However, in another sequential therapy regimen using ETV and PEG-IFN, there was no significant difference in HBeAg and HBsAg seroconversion between ETV plus PEG-IFN sequential therapy and sustained ETV monotherapy in HBeAg-positive CHB patients[45]. This hypothesis requires testing in large randomized clinical trials.
Factors that predict response to PEG-IFN therapy are an area of extensive investigation. These factors include serum HBV-DNA, ALT and HBsAg levels, HBV genotype and IL28 polymorphisms[40,41,43,46]. ALT flares (> 2-5 times the upper limit of normal) during IFN treatment reflecting enhanced host immune response[47] as well as low HBV-DNA are widely accepted as predictors for viral response to PEG-IFN therapy[40,48]. Studies have failed to find an association between HBV genotype and response after PEG-IFN therapy such as the phase III study conducted by Piratvisuth et al[43] and the NEPTUNE study by Liaw et al[49] which found no significant difference in HBeAg seroconversion between HBV genotype B and C groups 24 wk post-PEG-IFN treatment. Baseline HBsAg levels were associated with significantly different responses to PEG-IFN therapy in both studies. In addition, a recent study of HBeAg-positive CHB patients treated with PEG-IFN showed that HBsAg levels can be confidently used to guide therapy decisions and that discontinuation of PEG-IFN treatment is indicated in all patients with HBsAg levels > 20000 IU/mL after 24 wk of PEG-IFN therapy[46].
An IL28B polymorphism is associated with favorable viral response events such as HBeAg and HBsAg loss or seroconversion in HBeAg-positive CHB patients[46,50]. Furthermore, it was demonstrated that the HBsAg seroconversion rate in HBeAg-negative CHB patients was significantly higher in the IL28B CC group than in the non-CC group after a median of 11 years follow-up[51]. In contrast, no significant difference in HBeAg seroconversion rate was observed between the TT group and non-TT group of the IL28B in another study[52].
The levels of serum HBeAg may be considered as a predictive factor for response to PEG-IFN therapy. A recent study by Fried et al[53] showed that levels of HBeAg consistently decreased during treatment in patients who achieved HBeAg seroconversion and remained at their lowest level during the 24 wk of post-treatment follow-up. Taken together, lower HBV-DNA levels, higher ALT levels and lower HBsAg levels are considered strong candidate predictive markers of favorable response to PEG-IFN therapy. However, HBV genotype and IL28B polymorphisms still have limited application as useful predictive biomarkers of response to PEG-IFN therapy. Further RCTs on this issue are needed.
Nucleos(t)ide analogues
LAM: Although LAM is the first approved oral antiviral agent against HBV, the emergence of drug-resistant tyrosine-methionine-aspartate-aspartate (YMDD) mutants has been a major hindrance to long-term LAM treatment. The frequency of genotypic resistance was reported to be as high as 60%-70% after 5 years of treatment[6,7]. Therefore, it is no longer recommended as the first-line treatment for CHB patients in the current international guidelines, but it may be recommended in combination therapies with ADV or TDF for liver cirrhosis[40].
ADV: ADV is the acyclic analogue of dAMP with therapeutic efficacy against both the wild-type and YMDD mutant HBV. Two previous major phase III clinical studies showed that ADV demonstrated significant virological and biochemical responses, and histological improvement in HBeAg-positive and -negative naïve CHB patients[54,55]. ADV has also demonstrated virological improvement in patients with LAM-resistant HBV, regardless if used alone or in combination with ongoing LAM therapy[56,57]. Although ADV has been widely accepted as advantageous over LAM in terms of the development of genotypic resistance, it is not recommended as the first-line drug for HBeAg-positive and -negative CHB patients in the current international guidelines as it is less effective than other NAs such as ETV and TDF in antiviral activity[58], and possesses a significant risk of nephrotoxicity[59].
Entecavir: ETV is a deoxyguanosine nucleoside analogue which has highly potent antiviral activity and a high genetic barrier to resistance against HBV. In long-term follow-up studies of ETV for the treatment of chronic HBV infection for up to 5 years, it was very safe and well tolerated, and showed high rates of HBV-DNA suppression, ALT normalization and serological responses in both HBeAg-positive and -negative CHB patients[60,61]. Also, long-term ETV treatment showed the reversal of fibrosis or cirrhosis and continued histological improvement in patients with CHB[61]. Specifically, a post-hoc subgroup analysis in HBeAg-positive and -negative Asian CHB patients treated with ETV for up to 5 years also showed histological improvement with high rates of virological, biochemical and serological responses[62]. These results could provide evidence that ETV is beneficial in Asian CHB patients who have poor prognosis due to perinatal infection with genotype B and C in most cases. Moreover, the emergence of ETV resistance was very low, with a cumulative incidence of ETV resistance rates at year 1, 2, 3, 4, and 5 in treatment-naïve patients of 0.2%, 0.5%, 1.2%, 1.2% and 1.2%, respectively[63]. Based on the results from clinical studies, current regional guidelines have recommended ETV as a first-line therapy for the treatment of compensated and decompensated patients with chronic HBV infection.
LdT: LdT is the L-nucleoside analogue of L-deoxythymidine and displays potent antiviral activity comparable to that of ETV. HBV-DNA was undetectable (< 300 copies/mL) in 60% of HBeAg-positive CHB patients and 88% of HBeAg-negative CHB patients treated with LdT[64]. In addition, ALT normalization was found in 77% and 74%, respectively[65]. HBeAg seroconversion in HBeAg-positive CHB patients was observed in 23% and 30% at year 2 in two studies[64,65]. LdT provides higher rates of virological responses than LAM, but has also been associated with high rates of resistance due to a low genetic barrier. The rates of resistance to LdT at 1 year of treatment were 5% and 2% in HBeAg-positive and -negative CHB patients, and 25% and 11% at year 2, respectively[64,65]. Although LdT was well tolerated and safe, an asymptomatic elevation of creatinine kinase and symptomatic myopathy were occasionally reported. Taken together, LdT is not recommended as a first-line therapy for CHB patients in current international guidelines, but it is recommended as a combination therapy with ADV or TDF for liver cirrhosis[40].
Clevudine: Clevudine is a pyrimidine analogue with potent and sustained antiviral activity against HBV. Previous clinical studies conducted in Korea have demonstrated that clevudine showed potent antiviral activity during therapy and induced a sustained post-treatment antiviral effect for 6 mo after a 12- and 24-wk treatment period[66,67]. Moreover, a double-blind, randomized, clinical study comparing the efficacy and safety of clevudine vs LAM for 48 wk in treatment-naïve HBeAg-positive CHB patients revealed that serum HBV-DNA level was below 300 copies/mL in 73% of patients and that HBeAg seroconversion occurred in 18% of patients at week 48[68]. Although potent viral suppression and sustained antiviral activity after cessation of clevudine were observed, its efficacy has been hampered by the emergence of drug-resistant viral variants. A single mutation at rtM204I confers resistance to clevudine and the incidence of clevudine resistance at 48 wk and 2 years was 1.3%-7% and 24.4%, respectively[69,70]. Furthermore, high rates of symptomatic myopathy due to mitochondrial damage in the muscle have been reported with clevudine[71,72]. For these reasons, clevudine is not recommended as first-line therapy for CHB patients.
TDF: TDF is an acyclic nucleotide inhibitor and has been proved to be a highly powerful antiviral agent against HBV without resistance to TDF during the treatment period[58,73]. In a three-year follow-up study, levels of HBV-DNA below 400 copies/mL at week 144 was observed in 72% of HBeAg-positive and in 87% of HBeAg-negative patients treated with TDF monotherapy[74]. In addition, ALT normalization was found in 74% and 81%, respectively. In HBeAg-positive patients, rates of HBeAg and HBsAg loss were 34% and 8%, respectively. Furthermore, no genotypic resistance developed during the follow-up period. Interestingly, a recent long-term follow-up study over 5 years demonstrated that 87% of patients showed histological improvement and 51% had regression of fibrosis at week 240[75]. In addition, 74% of 96 patients with cirrhosis at baseline had no cirrhosis at year 5. Moreover, no genotypic resistance to TDF was detected. These results provided strong evidence that TDF was very safe and effective for long-term use in the treatment of CHB patients. Minor adverse events such as nephrotoxicity or decreased bone density were occasionally reported[76]. Current international guidelines recommend TDF and ETV, which are the two most effective antiviral agents, as first-line treatments for compensated and decompensated liver diseases in chronic HBV infection.
MECHANISMS AND TREATMENT OF DRUG RESISTANCE
Drug resistance is one of the most important causes of antiviral treatment failure in patients with CHB infection. The emergence of HBV mutants during antiviral treatment leads to a rapid increase in viral replication, resulting in histological deterioration with ALT flares. Therefore, it is critical to detect early HBV mutants in the treatment of CHB patients to improve long-term prognosis of the disease.
Although HBV is a DNA virus, its replication is processed by reverse transcriptase through an RNA intermediate. Because HBV-DNA polymerase lacks a proofreading mechanism, mutations can occur if NAs incompletely suppress viral replication. Under the selective pressure of NAs, newly emerging mutant strains are selected as predominant species. Subsequently, compensatory mutations in the presence of the primary mutation may emerge at other regions of the polymerase gene, resulting in increased viral replication compared to wild-type HBV[77]. There are three factors that are involved in the development of antiviral resistance; viral fitness, potency, and genetic barrier to resistance of the NAs[78].
Resistance to NAs is dependent on the structure of the NA. Eight codons in HBV polymerase are known to be involved in the development of antiviral resistance: 169, 180, 181, 184, 202, 204, 236, and 250. There are five pathways leading to antiviral resistance[79]: (1) the rtM204V/I pathway for L-nucleosides (LAM, LdT and Clevudine); (2) the rtN236T pathway for alkyl phosphonates (ADV, TDF); (3) the rtA181T/V pathway, which is shared between the L-nucleosides and alkyl phosphonates; and (4) the D-cyclopentane/ETV pathway (rtL180M + rtM204V + I169T + T184S/G/C + S202C/G/I + M250I/V).
The general principles of antiviral therapy for NA resistance include the following: (1) confirmation of the patient’s adherence to the drug; (2) detection of viral breakthrough and identification of genotypic resistance; and (3) consideration of combination therapy to prevent additional mutation caused by sequential NA therapy.
Lamivudine resistance
Although LAM is safe and tolerated in compensated and decompensated liver diseases due to HBV, it has limited clinical use in CHB patients due to a high rate of drug resistance. Previously, ADV alone or in combination with ongoing LAM therapy was used for the treatment of rtM204V/I mutant by LAM[56]. However, the rate of ADV resistance after direct switching from LAM to ADV in LAM-resistant patients was as high as 18% at year 1 and 65.6% at year 5, respectively[80,81]. On the other hand, rescue therapy switching to ETV at 1 mg daily for LAM-resistant patients was adopted, but genotypic ETV resistance and virological breakthrough developed in 51% and 43% of cases at year 5, respectively[63]. These results may be explained by cross-resistance shared by LAM and ETV. Thus, ETV monotherapy at a dose of 1 mg has not been further recommended as rescue therapy in LAM-resistant patients. TDF rescue therapy for ADV-resistant patients who were treated with ADV for 15 mo due to LAM-resistance, showed profound viral suppression of HBV-DNA below the detection limit of 400 copies/mL in 95% of cases[82]. Subsequently, a long-term study of TDF rescue monotherapy was conducted in patients with prior failure or resistance to different NA treatments[83]. Pretreatment consisted of either monotherapy with LAM, ADV, and sequential LAM-ADV therapy, or add-on combination therapy with both drugs. After a mean treatment duration of 23 mo, HBV-DNA was undetectable (< 400 copies/mL) in 79% of all patients. In addition, loss of HBeAg and HBsAg occurred in 24% and 3% of patients, respectively, suggesting that TDF monotherapy induced a potent and long-lasting antiviral response in NA-experienced patients with previous treatment failure[82]. PEG-IFN as rescue therapy for LAM-resistant patients may be considered for compensated liver disease. Current international guidelines include recommendations regarding rescue therapy for NAs-resistant patients (Table 2). For LAM-resistant patients, switching to TDF and ADV add-on therapy are commonly recommended. IFN-based therapy for those patients is only recommended in the APASL guideline.
Table 2.
Recommended treatment for drug resistance
| Resistance to | AASLD 2009 | EASL 2012 | APASL 2012 |
| LAM | Add ADV or TDF Switch to Truvada1 | Switch to TDF (add ADV if TDF is not available) | Add ADV Switch to TDF Switch to IFN-based therapy |
| LDT | Add ADV or TDF Switch to Truvada1 | Switch to or add TDF (add ADV if TDF is not available) | Add ADV Switch to TDF |
| ADV | Add LAM Switch to Truvada1 Switch to or add ETV | Switch to ETV or TDF Switch to TDF and add a nucleoside analogue if the patient has been treated with LAM | Add LAM, LDT or ETV Switch to TDF Switch to ETV plus TDF, if the patient has been treated with LAM or LDT |
| ETV | Switch to TDF or Truvada1 | Switch to or add TDF (add ADV if TDF is not available) | Add TDF or ADV |
| TDF | Unmentioned | Add ETV, LDT, LAM or emtricitabine Switch to ETV if the patient has not been treated with LAM in the past | Unmentioned |
| MDR | Unmentioned | Combination of a nucleoside and a nucleotide | Unmentioned |
Truvada is a combination pill containing emtricitabine 200 mg and tenofovir 300 mg. LAM: Lamivudine; LDT: Telbivudine; ADV: Adefovir; ETV: Entecavir; TDF:Tenofovir; MDR: Multidrug resistance; IFN: Interferon.
Adefovir resistance
ADV resistance is caused by rtN236T mutation in the D domain and rtA181T/V in the B domain of the HBV polymerase gene. A long-term follow-up study of ADV monotherapy for 48 wk in HBeAg-negative CHB showed ADV resistance in 0% at year 1 and 29% of patients at year 5[59], suggesting that long-term use of ADV could induce mutant strains. TDF has been proved to be effective in patients who were resistant to LAM and ADV. Although TDF shares partial resistance with ADV, it has been shown to have some antiviral effects in ADV resistance. In a recent study, TDF monotherapy was effective in patients with virological breakthrough or suboptimal response to ADV, but complete viral suppression was not found in patients with ADV-resistance, suggesting that a combination therapy of TDF with a NA should be considered in patients with ADV-resistance[84]. Because TDF possesses some degree of cross-resistance to ADV, the combination therapy of TDF plus LAM, LdT or ETV for patients with ADV-resistance may be more beneficial than TDF monotherapy to prevent further emergence of mutant strains. However, another study demonstrated that there was no significant difference in viral suppression between the combination of TDF plus emtricitabine and TDF alone in patients with CHB infection who had an incomplete response to ADV[85]. Further investigation is required.
Telbivudine resistance
LdT has relatively higher antiviral potency than LAM, however, prolonged treatment with LdT is limited by high rates of resistance due to a low genetic barrier. Studies reporting 1- and 2-year resistance rates to LdT were 5% and 25% in HBeAg-positive CHB patients, respectively[65]. A recent study revealed that LdT and ADV combination therapy led to significant decreases in serum HBV-DNA levels and normalization of ALT levels in patients with virological breakthrough or genotypic resistance to LdT[86]. Current international guidelines recommend add-on ADV or switching to TDF or Truvada in patients with LdT resistance.
Clevudine resistance
Clevudine is a nucleoside analogue with potent antiviral activity against HBV. Clevudine resistance in patients who have received clevudine therapy has been reported[70,87]. Although a long-term follow-up study of rescue therapy in clevudine-resistant patients has not been reported, the M204I mutation plays a key role in clevudine resistance and leads to virological breakthrough during long-term treatment. Drug susceptibility assays revealed that ADV and TDF were the most effective compounds against clevudine-resistant mutants. These results provide evidence of therapeutic options for clevudine-resistant patients. However, further clinical studies are required.
Entecavir resistance
ETV resistance occurs following a two-step mutation of HBV: (1) Pre-existing M204V and L180M by LAM; and (2) acquisition of the primary ETV resistance-encoding substitutions T184G and S202I or M250V. These mutations decrease ETV susceptibility and could give rise to virological rebound, leading to treatment failure[88]. After long-term ETV treatment in patients with LAM resistance, the rate of resistance was 51%[63]. This high resistance rate may be explained by rtM204V/I reducing the genetic barrier of ETV. Although the ETV resistance rate is not as high as other L-nucleoside analogues in naïve CHB, ETV rescue monotherapy at a dose of 1 mg for LAM-resistant patients should be considered for treatment failure due to virological rebound. Thus, add-on ADV to ETV may be beneficial in LAM-resistant patients to prevent further development of ETV resistance. Although clinical evidence regarding treatment for ETV resistance is insufficient to date, a recent study demonstrated the efficacy of TDF in ETV resistance[83]. Current international guidelines recommend add-on ADV or TDF or switching to TDF or Truvada in patients with ETV resistance.
Tenofovir resistance
TDF has been accepted as the most effective and safe antiviral nucleotide analogue for NA treatment-naïve or -failure patients to date. Recently, an open-label, long-term extension study of two previous phase III studies which confirmed no resistance to TDF after 48-wk treatment[74,75] revealed that TDF monotherapy maintains effective suppression of HBV-DNA through 288 wk (6 years) of treatment with no evidence of TDF resistance[89]. However, virological breakthrough occurred infrequently and was associated with non-adherence to study medication in the majority of cases. According to current international guidelines, TDF is recommended as an essential antiviral agent for compensated or decompensated liver diseases irrespective of any resistance to NAs.
Multidrug resistance
In general, sequential NA monotherapy against HBV can promote selection of multidrug-resistant (MDR) strains of HBV. In particular, this frequently occurs with sequential treatment using NAs with similar characteristics (e.g., LAM followed by ADV or ETV)[79]. Studies have shown that a combination therapy of TDF plus ETV in patients who had resistance to both LAM and ADV was effective[90,91]. A combination therapy of TDF plus ETV was shown to be effective in patients with MDR including LAM, ADV and ETV resistance. These results suggest that a combination therapy including TDF is better than other NA monotherapies or sequential therapy.
Currently, HBV drug-resistance mutation is mainly detected by direct sequencing and reverse hybridization. However, there are still limitations in identifying different substitutions present in the same viral variant with classic sequencing techniques[92]. Thus, it is necessary to find new tools to sequence large portions of the genome. Recently, a next generation sequencing (NGS) method has been developed to increase sequencing capacity while generating clonal sequences. The NGS method is processed through 3-step sequencing: library preparation, DNA capture and enrichment, and sequencing[93]. Newly developed virological tests may offer more optimized and tailored therapeutic strategies for treatment-naïve or -failure patients with chronic HBV infection. Current international guidelines do not recommend an appropriate treatment for MDR HBV caused by the anti-HBV NAs. However, based on pre-existing evidence, a combination of TDF and ETV is considered to be the most appropriate treatment for patients with MDR.
CONCLUSION
Although preventive vaccines and new antiviral agents against HBV have resulted in remarkable advances, chronic HBV infection is a still a difficult disease to control due to continuous viral replication from cccDNA in the nuclei of infected hepatocytes. Currently, there are two therapeutic approaches to control HBV replication: immunomodulating therapy and NAs. Despite extensive research, the exact roles of the immune response in controlling HBV infection or emerging HBV drug resistance are not completely understood. NAs therapy is considered an effective, safe and convenient therapy to control chronic HBV infection. However, the emergence of HBV mutant strains can lead to long-term treatment failure. The risk is very low or absent with ETV and TDF. Immune-based anti-viral strategies against HBV should be explored to achieve sustained viral control. International evidence-based guidelines have been developed to support physicians in managing CHB patients. However, it is difficult to initiate comprehensive therapy for MDR to NA as there is a lack of strong evidence to prove such issues. In addition, the currently available genotypic test, direct sequencing, still has limitations in identifying different substitutions present in the same viral variant. Therefore, the development of new virological tests identifying MDR may offer more optimized and tailored therapeutic strategies for treatment-naïve or -failure patients with chronic HBV infection. The factors influencing long-term treatment failure include patient compliance to drug, the emergence of HBV mutant strains, host genetic factors and the properties of each NA. It is critical to monitor viral load, serum HBsAg and ALT levels during antiviral therapy so that the therapeutic strategy can be continued or modified for patients with viral breakthrough or suboptimal response. Current practice guidelines stress the importance of profound and durable HBV viral suppression in the treatment of CHB patients. To this end, it is essential to choose a potent antiviral drug with a low risk of resistance for the initial treatment of CHB to achieve sustained virological response. TDF or ETV have a high genetic barrier and potent antiviral activity, and are widely accepted as first-line therapy for naïve patients at the present time. Furthermore, for patients with HBV mutant strains, combination therapy with NAs which have a high genetic barrier is more effective than sequential therapy of NAs with a low genetic barrier. Further studies are needed to explore the molecular mechanism of HBV mutations conferring resistance to NAs and to achieve optimal therapeutic modalities for patients with treatment failure. Finally, new anti-viral strategies that can persistently suppress HBV replication and overcome drug resistance should be investigated for the treatment of patients with chronic HBV infection.
Footnotes
P- Reviewer: Ballestri S, Bao ZJ, Liu QG S- Editor: Wen LL L- Editor: Webster JR E- Editor: Wang CH
References
- 1.Rehermann B, Nascimbeni M. Immunology of hepatitis B virus and hepatitis C virus infection. Nat Rev Immunol. 2005;5:215–229. doi: 10.1038/nri1573. [DOI] [PubMed] [Google Scholar]
- 2.Liang TJ. Hepatitis B: the virus and disease. Hepatology. 2009;49:S13–S21. doi: 10.1002/hep.22881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ganem D, Prince AM. Hepatitis B virus infection--natural history and clinical consequences. N Engl J Med. 2004;350:1118–1129. doi: 10.1056/NEJMra031087. [DOI] [PubMed] [Google Scholar]
- 4.Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ, Risk Evaluation of Viral Load E, Associated Liver Disease/Cancer-In HBVSG. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678–686. doi: 10.1053/j.gastro.2005.11.016. [DOI] [PubMed] [Google Scholar]
- 5.Chen CJ, Yang HI, Su J, Jen CL, You SL, Lu SN, Huang GT, Iloeje UH, Group R-HS. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65–73. doi: 10.1001/jama.295.1.65. [DOI] [PubMed] [Google Scholar]
- 6.Yoon SK, Jang JW, Kim CW, Bae SH, Choi JY, Choi SW, Lee YS, Lee CD, Chung KW, Sun HS, et al. Long-term results of lamivudine monotherapy in Korean patients with HBeAg-positive chronic hepatitis B: response and relapse rates, and factors related to durability of HBeAg seroconversion. Intervirology. 2005;48:341–349. doi: 10.1159/000086061. [DOI] [PubMed] [Google Scholar]
- 7.Dienstag JL, Goldin RD, Heathcote EJ, Hann HW, Woessner M, Stephenson SL, Gardner S, Gray DF, Schiff ER. Histological outcome during long-term lamivudine therapy. Gastroenterology. 2003;124:105–117. doi: 10.1053/gast.2003.50013. [DOI] [PubMed] [Google Scholar]
- 8.Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin R, Lu ZM, Piratvisuth T, Germanidis G, Yurdaydin C, et al. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2004;351:1206–1217. doi: 10.1056/NEJMoa040431. [DOI] [PubMed] [Google Scholar]
- 9.Lai CL, Leung N, Teo EK, Tong M, Wong F, Hann HW, Han S, Poynard T, Myers M, Chao G, et al. A 1-year trial of telbivudine, lamivudine, and the combination in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology. 2005;129:528–536. doi: 10.1016/j.gastro.2005.05.053. [DOI] [PubMed] [Google Scholar]
- 10.Zinkernagel RM. Immunology taught by viruses. Science. 1996;271:173–178. doi: 10.1126/science.271.5246.173. [DOI] [PubMed] [Google Scholar]
- 11.Janeway CA, Medzhitov R. Innate immune recognition. Annu Rev Immunol. 2002;20:197–216. doi: 10.1146/annurev.immunol.20.083001.084359. [DOI] [PubMed] [Google Scholar]
- 12.Wu J, Meng Z, Jiang M, Pei R, Trippler M, Broering R, Bucchi A, Sowa JP, Dittmer U, Yang D, et al. Hepatitis B virus suppresses toll-like receptor-mediated innate immune responses in murine parenchymal and nonparenchymal liver cells. Hepatology. 2009;49:1132–1140. doi: 10.1002/hep.22751. [DOI] [PubMed] [Google Scholar]
- 13.Visvanathan K, Skinner NA, Thompson AJ, Riordan SM, Sozzi V, Edwards R, Rodgers S, Kurtovic J, Chang J, Lewin S, et al. Regulation of Toll-like receptor-2 expression in chronic hepatitis B by the precore protein. Hepatology. 2007;45:102–110. doi: 10.1002/hep.21482. [DOI] [PubMed] [Google Scholar]
- 14.Dunn C, Brunetto M, Reynolds G, Christophides T, Kennedy PT, Lampertico P, Das A, Lopes AR, Borrow P, Williams K, et al. Cytokines induced during chronic hepatitis B virus infection promote a pathway for NK cell-mediated liver damage. J Exp Med. 2007;204:667–680. doi: 10.1084/jem.20061287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhang JY, Zou ZS, Huang A, Zhang Z, Fu JL, Xu XS, Chen LM, Li BS, Wang FS. Hyper-activated pro-inflammatory CD16 monocytes correlate with the severity of liver injury and fibrosis in patients with chronic hepatitis B. PLoS One. 2011;6:e17484. doi: 10.1371/journal.pone.0017484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rehermann B, Fowler P, Sidney J, Person J, Redeker A, Brown M, Moss B, Sette A, Chisari FV. The cytotoxic T lymphocyte response to multiple hepatitis B virus polymerase epitopes during and after acute viral hepatitis. J Exp Med. 1995;181:1047–1058. doi: 10.1084/jem.181.3.1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rehermann B, Lau D, Hoofnagle JH, Chisari FV. Cytotoxic T lymphocyte responsiveness after resolution of chronic hepatitis B virus infection. J Clin Invest. 1996;97:1655–1665. doi: 10.1172/JCI118592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Guidotti LG, Chisari FV. To kill or to cure: options in host defense against viral infection. Curr Opin Immunol. 1996;8:478–483. doi: 10.1016/s0952-7915(96)80034-3. [DOI] [PubMed] [Google Scholar]
- 19.Chisari FV, Ferrari C. Hepatitis B virus immunopathogenesis. Annu Rev Immunol. 1995;13:29–60. doi: 10.1146/annurev.iy.13.040195.000333. [DOI] [PubMed] [Google Scholar]
- 20.Chisari FV. Hepatitis B virus transgenic mice: models of viral immunobiology and pathogenesis. Curr Top Microbiol Immunol. 1996;206:149–173. doi: 10.1007/978-3-642-85208-4_9. [DOI] [PubMed] [Google Scholar]
- 21.Guidotti LG, Ishikawa T, Hobbs MV, Matzke B, Schreiber R, Chisari FV. Intracellular inactivation of the hepatitis B virus by cytotoxic T lymphocytes. Immunity. 1996;4:25–36. doi: 10.1016/s1074-7613(00)80295-2. [DOI] [PubMed] [Google Scholar]
- 22.Cavanaugh VJ, Guidotti LG, Chisari FV. Inhibition of hepatitis B virus replication during adenovirus and cytomegalovirus infections in transgenic mice. J Virol. 1998;72:2630–2637. doi: 10.1128/jvi.72.4.2630-2637.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chen MT, Billaud JN, Sällberg M, Guidotti LG, Chisari FV, Jones J, Hughes J, Milich DR. A function of the hepatitis B virus precore protein is to regulate the immune response to the core antigen. Proc Natl Acad Sci USA. 2004;101:14913–14918. doi: 10.1073/pnas.0406282101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chisari FV. Rous-Whipple Award Lecture. Viruses, immunity, and cancer: lessons from hepatitis B. Am J Pathol. 2000;156:1117–1132. doi: 10.1016/s0002-9440(10)64980-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bertoletti A, Ferrari C. Innate and adaptive immune responses in chronic hepatitis B virus infections: towards restoration of immune control of viral infection. Gut. 2012;61:1754–1764. doi: 10.1136/gutjnl-2011-301073. [DOI] [PubMed] [Google Scholar]
- 26.Gruener NH, Lechner F, Jung MC, Diepolder H, Gerlach T, Lauer G, Walker B, Sullivan J, Phillips R, Pape GR, et al. Sustained dysfunction of antiviral CD8+ T lymphocytes after infection with hepatitis C virus. J Virol. 2001;75:5550–5558. doi: 10.1128/JVI.75.12.5550-5558.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Michel ML, Deng Q, Mancini-Bourgine M. Therapeutic vaccines and immune-based therapies for the treatment of chronic hepatitis B: perspectives and challenges. J Hepatol. 2011;54:1286–1296. doi: 10.1016/j.jhep.2010.12.031. [DOI] [PubMed] [Google Scholar]
- 28.Kakimi K, Guidotti LG, Koezuka Y, Chisari FV. Natural killer T cell activation inhibits hepatitis B virus replication in vivo. J Exp Med. 2000;192:921–930. doi: 10.1084/jem.192.7.921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pol S, Lampertico P. First-line treatment of chronic hepatitis B with entecavir or tenofovir in ‘real-life’ settings: from clinical trials to clinical practice. J Viral Hepat. 2012;19:377–386. doi: 10.1111/j.1365-2893.2012.01602.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Franzese O, Kennedy PT, Gehring AJ, Gotto J, Williams R, Maini MK, Bertoletti A. Modulation of the CD8+-T-cell response by CD4+ CD25+ regulatory T cells in patients with hepatitis B virus infection. J Virol. 2005;79:3322–3328. doi: 10.1128/JVI.79.6.3322-3328.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Stoop JN, van der Molen RG, Baan CC, van der Laan LJ, Kuipers EJ, Kusters JG, Janssen HL. Regulatory T cells contribute to the impaired immune response in patients with chronic hepatitis B virus infection. Hepatology. 2005;41:771–778. doi: 10.1002/hep.20649. [DOI] [PubMed] [Google Scholar]
- 32.van der Molen RG, Sprengers D, Binda RS, de Jong EC, Niesters HG, Kusters JG, Kwekkeboom J, Janssen HL. Functional impairment of myeloid and plasmacytoid dendritic cells of patients with chronic hepatitis B. Hepatology. 2004;40:738–746. doi: 10.1002/hep.20366. [DOI] [PubMed] [Google Scholar]
- 33.Barber DL, Wherry EJ, Masopust D, Zhu B, Allison JP, Sharpe AH, Freeman GJ, Ahmed R. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature. 2006;439:682–687. doi: 10.1038/nature04444. [DOI] [PubMed] [Google Scholar]
- 34.Petrovas C, Casazza JP, Brenchley JM, Price DA, Gostick E, Adams WC, Precopio ML, Schacker T, Roederer M, Douek DC, et al. PD-1 is a regulator of virus-specific CD8+ T cell survival in HIV infection. J Exp Med. 2006;203:2281–2292. doi: 10.1084/jem.20061496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Boettler T, Panther E, Bengsch B, Nazarova N, Spangenberg HC, Blum HE, Thimme R. Expression of the interleukin-7 receptor alpha chain (CD127) on virus-specific CD8+ T cells identifies functionally and phenotypically defined memory T cells during acute resolving hepatitis B virus infection. J Virol. 2006;80:3532–3540. doi: 10.1128/JVI.80.7.3532-3540.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Rehermann B, Pasquinelli C, Mosier SM, Chisari FV. Hepatitis B virus (HBV) sequence variation of cytotoxic T lymphocyte epitopes is not common in patients with chronic HBV infection. J Clin Invest. 1995;96:1527–1534. doi: 10.1172/JCI118191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bertoletti A, Costanzo A, Chisari FV, Levrero M, Artini M, Sette A, Penna A, Giuberti T, Fiaccadori F, Ferrari C. Cytotoxic T lymphocyte response to a wild type hepatitis B virus epitope in patients chronically infected by variant viruses carrying substitutions within the epitope. J Exp Med. 1994;180:933–943. doi: 10.1084/jem.180.3.933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bertoletti A, Sette A, Chisari FV, Penna A, Levrero M, De Carli M, Fiaccadori F, Ferrari C. Natural variants of cytotoxic epitopes are T-cell receptor antagonists for antiviral cytotoxic T cells. Nature. 1994;369:407–410. doi: 10.1038/369407a0. [DOI] [PubMed] [Google Scholar]
- 39.Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, Guan R, Lau GK, Locarnini S, Chronic Hepatitis BGWPotA-PAftSotL. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2:263–283. doi: 10.1007/s12072-008-9080-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–662. doi: 10.1002/hep.23190. [DOI] [PubMed] [Google Scholar]
- 41.European Association For The Study Of The L. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol. 2012;57:167–185. doi: 10.1016/j.jhep.2012.02.010. [DOI] [PubMed] [Google Scholar]
- 42.Lau GK, Piratvisuth T, Luo KX, Marcellin P, Thongsawat S, Cooksley G, Gane E, Fried MW, Chow WC, Paik SW, et al. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med. 2005;352:2682–2695. doi: 10.1056/NEJMoa043470. [DOI] [PubMed] [Google Scholar]
- 43.Piratvisuth T, Lau G, Chao YC, Jin R, Chutaputti A, Zhang QB, Tanwandee T, Button P, Popescu M. Sustained response to peginterferon alfa-2a (40 kD) with or without lamivudine in Asian patients with HBeAg-positive and HBeAg-negative chronic hepatitis B. Hepatol Int. 2008;2:102–110. doi: 10.1007/s12072-007-9022-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sarin SK, Sood A, Kumar M, Arora A, Amrapurkar D, Sharma BC, Konar A, Chawla YK, Jain RK, Nanda V, Kumar A, Hissar S, Lavate P, Lahoti D, National Collaborative Group on Hepatitis B I. Effect of lowering HBV DNA levels by initial antiviral therapy before adding immunomodulator on treatment of chronic hepatitis B. Am J Gastroenterol. 2007;102:96–104. doi: 10.1111/j.1572-0241.2006.01006.x. [DOI] [PubMed] [Google Scholar]
- 45.Chen CC, Wang PC, Chang HW, Chen CF. Safety and efficacy of two-step peginterferon α-2a treatment in patients of chronic hepatitis B with acute exacerbation. J Viral Hepat. 2012;19:161–172. doi: 10.1111/j.1365-2893.2011.01469.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sonneveld MJ, Hansen BE, Piratvisuth T, Jia JD, Zeuzem S, Gane E, Liaw YF, Xie Q, Heathcote EJ, Chan HL, et al. Response-guided peginterferon therapy in hepatitis B e antigen-positive chronic hepatitis B using serum hepatitis B surface antigen levels. Hepatology. 2013;58:872–880. doi: 10.1002/hep.26436. [DOI] [PubMed] [Google Scholar]
- 47.Perrillo RP. Acute flares in chronic hepatitis B: the natural and unnatural history of an immunologically mediated liver disease. Gastroenterology. 2001;120:1009–1022. doi: 10.1053/gast.2001.22461. [DOI] [PubMed] [Google Scholar]
- 48.Flink HJ, Sprengers D, Hansen BE, van Zonneveld M, de Man RA, Schalm SW, Janssen HL, Group HBVS. Flares in chronic hepatitis B patients induced by the host or the virus? Relation to treatment response during Peg-interferon {alpha}-2b therapy. Gut. 2005;54:1604–1609. doi: 10.1136/gut.2004.062208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Liaw YF, Jia JD, Chan HL, Han KH, Tanwandee T, Chuang WL, Tan DM, Chen XY, Gane E, Piratvisuth T, et al. Shorter durations and lower doses of peginterferon alfa-2a are associated with inferior hepatitis B e antigen seroconversion rates in hepatitis B virus genotypes B or C. Hepatology. 2011;54:1591–1599. doi: 10.1002/hep.24555. [DOI] [PubMed] [Google Scholar]
- 50.Wu X, Xin Z, Zhu X, Pan L, Li Z, Li H, Liu Y. Evaluation of susceptibility locus for response to interferon-α based therapy in chronic hepatitis B patients in Chinese. Antiviral Res. 2012;93:297–300. doi: 10.1016/j.antiviral.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 51.Lampertico P, Viganò M, Cheroni C, Facchetti F, Invernizzi F, Valveri V, Soffredini R, Abrignani S, De Francesco R, Colombo M. IL28B polymorphisms predict interferon-related hepatitis B surface antigen seroclearance in genotype D hepatitis B e antigen-negative patients with chronic hepatitis B. Hepatology. 2013;57:890–896. doi: 10.1002/hep.25749. [DOI] [PubMed] [Google Scholar]
- 52.Tseng TC, Yu ML, Liu CJ, Lin CL, Huang YW, Hsu CS, Liu CH, Kuo SF, Pan CJ, Yang SS, et al. Effect of host and viral factors on hepatitis B e antigen-positive chronic hepatitis B patients receiving pegylated interferon-α-2a therapy. Antivir Ther. 2011;16:629–637. doi: 10.3851/IMP1841. [DOI] [PubMed] [Google Scholar]
- 53.Fried MW, Piratvisuth T, Lau GK, Marcellin P, Chow WC, Cooksley G, Luo KX, Paik SW, Liaw YF, Button P, et al. HBeAg and hepatitis B virus DNA as outcome predictors during therapy with peginterferon alfa-2a for HBeAg-positive chronic hepatitis B. Hepatology. 2008;47:428–434. doi: 10.1002/hep.22065. [DOI] [PubMed] [Google Scholar]
- 54.Marcellin P, Chang TT, Lim SG, Tong MJ, Sievert W, Shiffman ML, Jeffers L, Goodman Z, Wulfsohn MS, Xiong S, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med. 2003;348:808–816. doi: 10.1056/NEJMoa020681. [DOI] [PubMed] [Google Scholar]
- 55.Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, Marcellin P, Lim SG, Goodman Z, Wulfsohn MS, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-negative chronic hepatitis B. N Engl J Med. 2003;348:800–807. doi: 10.1056/NEJMoa021812. [DOI] [PubMed] [Google Scholar]
- 56.Peters MG, Hann Hw Hw, Martin P, Heathcote EJ, Buggisch P, Rubin R, Bourliere M, Kowdley K, Trepo C, Gray Df Df, et al. Adefovir dipivoxil alone or in combination with lamivudine in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology. 2004;126:91–101. doi: 10.1053/j.gastro.2003.10.051. [DOI] [PubMed] [Google Scholar]
- 57.Perrillo R, Hann HW, Mutimer D, Willems B, Leung N, Lee WM, Moorat A, Gardner S, Woessner M, Bourne E, et al. Adefovir dipivoxil added to ongoing lamivudine in chronic hepatitis B with YMDD mutant hepatitis B virus. Gastroenterology. 2004;126:81–90. doi: 10.1053/j.gastro.2003.10.050. [DOI] [PubMed] [Google Scholar]
- 58.Marcellin P, Heathcote EJ, Buti M, Gane E, de Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med. 2008;359:2442–2455. doi: 10.1056/NEJMoa0802878. [DOI] [PubMed] [Google Scholar]
- 59.Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, Marcellin P, Lim SG, Goodman Z, Ma J, et al. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B for up to 5 years. Gastroenterology. 2006;131:1743–1751. doi: 10.1053/j.gastro.2006.09.020. [DOI] [PubMed] [Google Scholar]
- 60.Chang TT, Lai CL, Kew Yoon S, Lee SS, Coelho HS, Carrilho FJ, Poordad F, Halota W, Horsmans Y, Tsai N, et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology. 2010;51:422–430. doi: 10.1002/hep.23327. [DOI] [PubMed] [Google Scholar]
- 61.Chang TT, Liaw YF, Wu SS, Schiff E, Han KH, Lai CL, Safadi R, Lee SS, Halota W, Goodman Z, et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology. 2010;52:886–893. doi: 10.1002/hep.23785. [DOI] [PubMed] [Google Scholar]
- 62.Tong MJ, Kowdley KV, Pan C, Hu KQ, Chang TT, Han KH, Yoon SK, Goodman ZD, Beebe S, Iloeje U, et al. Improvement in liver histology among Asian patients with chronic hepatitis B after long-term treatment with entecavir. Liver Int. 2013;33:650–651. doi: 10.1111/liv.12121. [DOI] [PubMed] [Google Scholar]
- 63.Tenney DJ, Rose RE, Baldick CJ, Pokornowski KA, Eggers BJ, Fang J, Wichroski MJ, Xu D, Yang J, Wilber RB, et al. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naïve patients is rare through 5 years of therapy. Hepatology. 2009;49:1503–1514. doi: 10.1002/hep.22841. [DOI] [PubMed] [Google Scholar]
- 64.Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, Chen Y, Heathcote EJ, Rasenack J, Bzowej N, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med. 2007;357:2576–2588. doi: 10.1056/NEJMoa066422. [DOI] [PubMed] [Google Scholar]
- 65.Liaw YF, Gane E, Leung N, Zeuzem S, Wang Y, Lai CL, Heathcote EJ, Manns M, Bzowej N, Niu J, Han SH, Hwang SG, Cakaloglu Y, Tong MJ, Papatheodoridis G, Chen Y, Brown NA, Albanis E, Galil K, Naoumov NV, Group GS. 2-Year GLOBE trial results: telbivudine Is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology. 2009;136:486–495. doi: 10.1053/j.gastro.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 66.Lee HS, Chung YH, Lee K, Byun KS, Paik SW, Han JY, Yoo K, Yoo HW, Lee JH, Yoo BC. A 12-week clevudine therapy showed potent and durable antiviral activity in HBeAg-positive chronic hepatitis B. Hepatology. 2006;43:982–988. doi: 10.1002/hep.21166. [DOI] [PubMed] [Google Scholar]
- 67.Yoo BC, Kim JH, Chung YH, Lee KS, Paik SW, Ryu SH, Han BH, Han JY, Byun KS, Cho M, et al. Twenty-four-week clevudine therapy showed potent and sustained antiviral activity in HBeAg-positive chronic hepatitis B. Hepatology. 2007;45:1172–1178. doi: 10.1002/hep.21629. [DOI] [PubMed] [Google Scholar]
- 68.Lau GK, Leung N. Forty-eight weeks treatment with clevudine 30 mg qd versus lamivudine 100 mg qd for chronic hepatitis B infection: a double-blind randomized study. Korean J Hepatol. 2010;16:315–320. doi: 10.3350/kjhep.2010.16.3.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Ko SY, Kwon SY, Choe WH, Kim BK, Kim KH, Lee CH. Clinical and virological responses to clevudine therapy in chronic hepatitis B patients: results at 1 year of an open-labelled prospective study. Antivir Ther. 2009;14:585–590. [PubMed] [Google Scholar]
- 70.Jang JH, Kim JW, Jeong SH, Myung HJ, Kim HS, Park YS, Lee SH, Hwang JH, Kim N, Lee DH. Clevudine for chronic hepatitis B: antiviral response, predictors of response, and development of myopathy. J Viral Hepat. 2011;18:84–90. doi: 10.1111/j.1365-2893.2010.01281.x. [DOI] [PubMed] [Google Scholar]
- 71.Tak WY, Park SY, Cho CM, Jung MK, Jeon SW, Kweon YO, Park JY, Sohn YK. Clinical, biochemical, and pathological characteristics of clevudine-associated myopathy. J Hepatol. 2010;53:261–266. doi: 10.1016/j.jhep.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 72.Lee HJ, Eun JR, Lee CH, Hwang JS, Suh JI, Kim BS, Jang BK. [Long-term clevudine therapy in nucleos(t)ide-naïve and lamivudine-experienced patients with hepatitis B virus-related chronic liver diseases] Korean J Hepatol. 2009;15:179–192. doi: 10.3350/kjhep.2009.15.2.179. [DOI] [PubMed] [Google Scholar]
- 73.Woo G, Tomlinson G, Nishikawa Y, Kowgier M, Sherman M, Wong DK, Pham B, Ungar WJ, Einarson TR, Heathcote EJ, et al. Tenofovir and entecavir are the most effective antiviral agents for chronic hepatitis B: a systematic review and Bayesian meta-analyses. Gastroenterology. 2010;139:1218–1229. doi: 10.1053/j.gastro.2010.06.042. [DOI] [PubMed] [Google Scholar]
- 74.Heathcote EJ, Marcellin P, Buti M, Gane E, De Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, et al. Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology. 2011;140:132–143. doi: 10.1053/j.gastro.2010.10.011. [DOI] [PubMed] [Google Scholar]
- 75.Marcellin P, Gane E, Buti M, Afdhal N, Sievert W, Jacobson IM, Washington MK, Germanidis G, Flaherty JF, Schall RA, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381:468–475. doi: 10.1016/S0140-6736(12)61425-1. [DOI] [PubMed] [Google Scholar]
- 76.Gish RG, Clark MD, Kane SD, Shaw RE, Mangahas MF, Baqai S. Similar risk of renal events among patients treated with tenofovir or entecavir for chronic hepatitis B. Clin Gastroenterol Hepatol. 2012;10:941–946; quiz e968. doi: 10.1016/j.cgh.2012.04.008. [DOI] [PubMed] [Google Scholar]
- 77.Melegari M, Scaglioni PP, Wands JR. Hepatitis B virus mutants associated with 3TC and famciclovir administration are replication defective. Hepatology. 1998;27:628–633. doi: 10.1002/hep.510270243. [DOI] [PubMed] [Google Scholar]
- 78.Richman DD. The impact of drug resistance on the effectiveness of chemotherapy for chronic hepatitis B. Hepatology. 2000;32:866–867. doi: 10.1053/jhep.2000.18194. [DOI] [PubMed] [Google Scholar]
- 79.Zoulim F, Locarnini S. Hepatitis B virus resistance to nucleos(t)ide analogues. Gastroenterology. 2009;137:1593–1608.e1-e2. doi: 10.1053/j.gastro.2009.08.063. [DOI] [PubMed] [Google Scholar]
- 80.Lee YS, Suh DJ, Lim YS, Jung SW, Kim KM, Lee HC, Chung YH, Lee YS, Yoo W, Kim SO. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology. 2006;43:1385–1391. doi: 10.1002/hep.21189. [DOI] [PubMed] [Google Scholar]
- 81.Lee JM, Park JY, Kim do Y, Nguyen T, Hong SP, Kim SO, Chon CY, Han KH, Ahn SH. Long-term adefovir dipivoxil monotherapy for up to 5 years in lamivudine-resistant chronic hepatitis B. Antivir Ther. 2010;15:235–241. doi: 10.3851/IMP1510. [DOI] [PubMed] [Google Scholar]
- 82.van Bömmel F, Zöllner B, Sarrazin C, Spengler U, Hüppe D, Möller B, Feucht HH, Wiedenmann B, Berg T. Tenofovir for patients with lamivudine-resistant hepatitis B virus (HBV) infection and high HBV DNA level during adefovir therapy. Hepatology. 2006;44:318–325. doi: 10.1002/hep.21253. [DOI] [PubMed] [Google Scholar]
- 83.van Bömmel F, de Man RA, Wedemeyer H, Deterding K, Petersen J, Buggisch P, Erhardt A, Hüppe D, Stein K, Trojan J, et al. Long-term efficacy of tenofovir monotherapy for hepatitis B virus-monoinfected patients after failure of nucleoside/nucleotide analogues. Hepatology. 2010;51:73–80. doi: 10.1002/hep.23246. [DOI] [PubMed] [Google Scholar]
- 84.Tan J, Degertekin B, Wong SN, Husain M, Oberhelman K, Lok AS. Tenofovir monotherapy is effective in hepatitis B patients with antiviral treatment failure to adefovir in the absence of adefovir-resistant mutations. J Hepatol. 2008;48:391–398. doi: 10.1016/j.jhep.2007.09.020. [DOI] [PubMed] [Google Scholar]
- 85.Berg T, Marcellin P, Zoulim F, Moller B, Trinh H, Chan S, Suarez E, Lavocat F, Snow-Lampart A, Frederick D, et al. Tenofovir is effective alone or with emtricitabine in adefovir-treated patients with chronic-hepatitis B virus infection. Gastroenterology. 2010;139:1207–1217. doi: 10.1053/j.gastro.2010.06.053. [DOI] [PubMed] [Google Scholar]
- 86.Zhang Y, Lian JQ, Li Y, Wang JP, Huang CX, Bai XF, Wang JP. Telbivudine plus adefovir therapy for chronic hepatitis B patients with virological breakthrough or genotypic resistance to telbivudine. Eur J Gastroenterol Hepatol. 2013;25:814–819. doi: 10.1097/MEG.0b013e32835ee516. [DOI] [PubMed] [Google Scholar]
- 87.Kim YS, Kim GH, Hwang YJ, Kwon OS, Choi DJ, Kim JH. Early development of clevudine resistance during clevudine therapy in a patient with chronic hepatitis B who received prior lamivudine therapy. Liver Int. 2009;29:950–951. doi: 10.1111/j.1478-3231.2008.01967.x. [DOI] [PubMed] [Google Scholar]
- 88.Tenney DJ, Levine SM, Rose RE, Walsh AW, Weinheimer SP, Discotto L, Plym M, Pokornowski K, Yu CF, Angus P, et al. Clinical emergence of entecavir-resistant hepatitis B virus requires additional substitutions in virus already resistant to Lamivudine. Antimicrob Agents Chemother. 2004;48:3498–3507. doi: 10.1128/AAC.48.9.3498-3507.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Kitrinos KM, Corsa A, Liu Y, Flaherty J, Snow-Lampart A, Marcellin P, Borroto-Esoda K, Miller MD. No detectable resistance to tenofovir disoproxil fumarate after 6 years of therapy in patients with chronic hepatitis B. Hepatology. 2014;59:434–442. doi: 10.1002/hep.26686. [DOI] [PubMed] [Google Scholar]
- 90.Lok AS, Zoulim F, Locarnini S, Bartholomeusz A, Ghany MG, Pawlotsky JM, Liaw YF, Mizokami M, Kuiken C, Hepatitis BVDRWG. Antiviral drug-resistant HBV: standardization of nomenclature and assays and recommendations for management. Hepatology. 2007;46:254–265. doi: 10.1002/hep.21698. [DOI] [PubMed] [Google Scholar]
- 91.Petersen J, Ratziu V, Buti M, Janssen HL, Brown A, Lampertico P, Schollmeyer J, Zoulim F, Wedemeyer H, Sterneck M, et al. Entecavir plus tenofovir combination as rescue therapy in pre-treated chronic hepatitis B patients: an international multicenter cohort study. J Hepatol. 2012;56:520–526. doi: 10.1016/j.jhep.2011.09.018. [DOI] [PubMed] [Google Scholar]
- 92.Chevaliez S, Rodriguez C, Pawlotsky JM. New virologic tools for management of chronic hepatitis B and C. Gastroenterology. 2012;142:1303–1313.e1301. doi: 10.1053/j.gastro.2012.02.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Metzker ML. Sequencing technologies - the next generation. Nat Rev Genet. 2010;11:31–46. doi: 10.1038/nrg2626. [DOI] [PubMed] [Google Scholar]