

Highlights
-
•
Agenesis of the pubis is a very rare clinical deformity which can be a sign of urogenital abnormalities. To report a rare condition would help clinicians to diagnose co-morbidities which may affect children remaining life.
-
•
This is a rare pattern of associated anomalies confined to a localized region of the body. Somatic mutations may responsible for developmental abnormalities of mesoderm from which the pubic bones and urogenital structures develop.
-
•
An isolated X-ray finding of ramus pubis agenesis may associate with cryptorchidism or several other urogenital malformations.
Keywords: Pubis agenesis, Acetabular dysplasia, Undescended testes, Cryptorchidism
Abstract
INTRODUCTION
Agenesis of the pubic bone, as evidenced in the world literature, is a very rare clinical and congenital abnormality. Several disorders may occur with hypoplasia of the pubis.
PRESENTATION OF CASE
Here, we report a rare longer follow-up case of the congenital unilateral agenesis of the superior ramus of pubic bone with bilateral undescended testes, osteoporosis, cranial malformations, acetabular dysplasia, unilateral shortening of the lower extremity and an abnormal gait pattern.
DISCUSSION
Somatic mutations may responsible for developmental abnormalities of the mesoderm from which the pubic bones and urogenital structures develop.
CONCLUSION
An isolated x-ray finding of ramus pubis agenesis may associate with cryptorchidism or several other urogenital malformations.
1. Introduction
The pubis is the lowest and most anterior portion of the hip bones of the pelvis. The pubis has a body, a superior ramus, and an inferior ramus. The body of the pubis contributes to the lunate surface and acetabular fossa in the acetabulum. Ossification of the pubic bone begins in the 18th to 20th gestational week. The superior pubic and ischial rami of a full-term neonate are usually ossified.1 The ischiopubic component of the pelvis starts to develop antenatal between the fifth and sixth months of fetal life from two ossification centers, an ischial (inferolateral) and a pubic (superomedial) center. At birth, the ossification is almost complete; however, the ischial and pubic segments remain separated by a cartilaginous tissue, the ischiopubic synchondrosis. Ossification and closure of the ischiopubic synchondrosis are variable, usually occurring between 4 and 12 years of age.2
Agenesis of the pubic bone, as evidenced in the world literature, is a very rare clinical and congenital abnormality. Congenital agenesis of the pubis may present itself as either an isolated anomaly or as a syndromic constituent. Several disorders may occur with hypoplasia of the pubis. Some of these are extrophy of the bladder, epispadias, hypospadias, small patella syndrome, achondrogeneses 1 and 2, rib anomalies, multipl segmenter deficits of the spine, hipochondrogenesis, camptomelic dysplasia, hypophosphatasia, undescended testes, acetabular dysplasia and congenital dislocation of the hip. This case demonstrates a rare condition of congenital unilateral agenesis of the superior ramus with bilateral undescended testes, osteoporosis, acetabular dysplasia and an abnormal gait pattern.
2. Case report
In 2002, a 5-years-old boy who was admitted to our clinic with a limp and extraversion in the right leg. His parents confirmed that he had been born in 41 weeks by normal spontaneous vaginal delivery and that he was a healthy newborn. He was taken to a hospital because of extraversion in his right leg when he was six months old. In this hospital, he received follow-up for the right hip acetabular dysplasia. A physical examination by the urologist revealed bilateral undescended testes when he was one year old. The testosterone level was <20 ng/dl, LH was 0.16 mIU/ml, FSH was 2.81 mIU/ml, inhibin B was <10 ng/l. He put on human chorionic gonadotropin (hCG/Pregnyl®) 1500 IU per day for four days to stimulate testicular descent. After the stimulation, the testosterone level was found at <20 ng/dl again and no testes were palpated in scrotum. The patient underwent inguinal and pelvic exploration by the urologist and rudimentary testes tissues were found at the superior of the bladder and the chromosomal analysis was 46 XY. Also, testosterone secretions were not found.
The boy was five years old when he was admitted to orthopedics clinic and at the physical examination, his right hip abduction was 45°, flexion was 135°, internal rotation was 50° and external rotation was 90°. Clinically, the right lower limb was 2 cm shorter. Trendelenburg test was positive and right lower limb was in slightly external rotation while he walks. There were an old incision scar in the patient's right and left inguinal regions and neither testis could be palpated in the scrotum. There was a slight contracture of the iliospoas tendon on the right side which was diagnosed with a Thomas test. The neurologic and mental examinations were within normal limits. At the antero-posterior pelvic X-ray the superior ramus of the right pubic bone was not detected. An acetabular index (AI) of 20° on the right and 16° on the left hip was recorded at the initial radiologic examination (Fig. 1). Imaging of the lumbar region was performed and no abnormality was found and no secondary structural change was noted (Fig. 2). Cranial MRI showed that a 4 cm × 5 cm arachnoid cyst in the occipital region. His T score was −5.1 in the L2–L4 region for bone mineral density and his bone age was 3.5-years-old. Compared to his peers, he was considered as osteoporotic and the treatment was begun. Genetic screening has detected no additional syndrome. Gait analyses of the patient showed that right hip extensor muscle groups were dominant, anterior pelvic tilt (Fig. 3) and right hip abduction were detected in the stance phase (Fig. 4). The iliopsoas muscle group was considered to be short according to gait analysis. The patient was followed at interval of six months and an arthrogram was performed for dynamic fluoroscopic examination of the right hip when he was six years old. In surgery AI was measured at 21° on the right side by fluoroscopic evaluation. The femoral head was well-covered with asetabular cartilage, his hip range of motion was full and spherical congruency between femoral head and acetabulum was present (Figs. 5A and B and 6).
Fig. 1.

Superior ramus of the right pubic bone was not detected at initial orthopedic admission.
Fig. 2.

Lumbosakral imaging showed no abnormality.
Fig. 3.

Anterior pelvic tilt in sagittal plane.
Fig. 4.
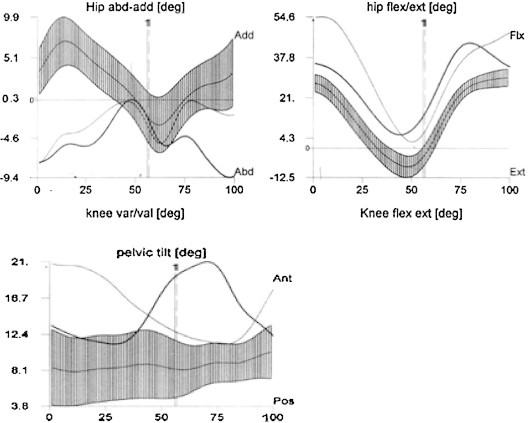
Gait analyses of the patient shows right hip flexor muscles were dominant, anterior pelvic tilt and right hip abduction was detected in the stance phase.
Fig. 5.
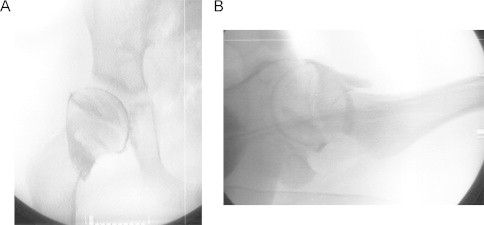
(A and B) Arthrogram shows well covered femoral head and spherical congruency.
Fig. 6.

AP pelvis X-ray when he was 7-years-old.
At 14 years old, the boy was fully ambulatory, with 2 cm right lower extremity shortening, a slight Trendelenburg gait and had no sign of pain. He is currently being followed by pediatric endocrinology for testicular regression syndrome. His T score was improved to −3.2 in the L2–L4 region with bisphosphonate and vitamin D treatment. His bone age was 13 years old, testosterone level was <20 ng/dl and he was still on testosterone replacement therapy. His AI was improved to 18° on the right and 15° on the left hip. His central edge angle (CEA) was 24° on the right and 26° on the left hip (Fig. 7A and B). No additional surgery was needed.
Fig. 7.
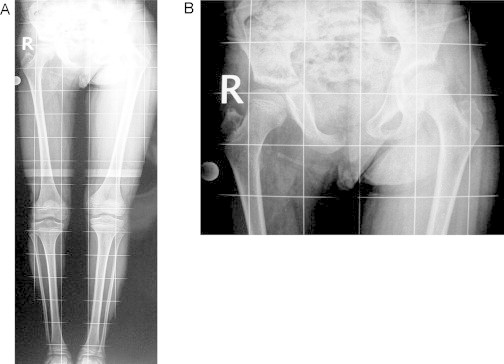
(A and B) Last follow up X-rays shows 2 cm right lower extremity shortening, pelvic obliquity, acetabular dysplasia with a horizontal sourcil.
3. Discussion
The abnormality of our patient was congenital unilateral agenesis of the superior ramus of the pubic bone with bilateral undescended testes, osteoporosis, cranium malformations, acetabular dysplasia and an abnormal gait pattern.
Recognition of the agenesis of pubic bones is of clinical importance, because bone abnormalities can be seen in conjunction with other musculoskeletal and urogenital abnormalities such as teratologic hip dislocation, patellar hypoplasia, undescended testes, and hypospadias.3,4 Sarban et al.4 found that the absence of the pubic bone may be a cause of acetabular dysplasia. Their case was presented with teratogenic left hip dislocation, undescended left testes, hypospadias and left pubic bone aplasia. They were performed open reduction with capsular plication when the infant was eighteen months old. The AI was within the normal range and the infant were fully ambulatory at the last follow-up. Sponseller et al.5 compared computerized tomography scans of the pelvis of the 24 patients who had exstrophy of the bladder with scans of age-matched controls. They found 30% shortening of the pubic rami, and progressive diastasis of the symphysis pubis. In the literature such as this urologic abnormalities were reported to be together with the agenesis of pelvic structures. Like our study, Yildiz et al. showed a rare entity that undescended testes with agenesis of pubic rami.6
In conclusion, we suggest that this is a rare pattern of associated anomalies confined to a localized region of the body. Somatic mutations may responsible for developmental abnormalities of the mesoderm from which the pubic bones and urogenital structures develop. An isolated X-ray finding of ramus pubis agenesis may associate with cryptorchidism or several other urogenital malformations.
Conflict of interest
Each author certifies that he or she has no commercial associations that might pose a conflict of interest in connection with the submitted article.
Funding
This study has not been published elsewhere before. It is not accepted for publication and under consideration by another publication. There is no commercial association that might pose the manuscript and the data.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author contributions
Yavuz Saglam M.D. contributed in the study design, data collections, data analysis and writing the manuscript. Murat Dursun M.D. contributed in the study design, data analysis, and in writing. Goksel Dikmen M.D. contributed in data collections and data analysis. Suleyman Bora Goksan M.D. contributed in data analysis and writing.
Key learning points.
-
•
Agenesis of pubis is a very rare clinical deformity which can be a sign of urogenital abnormalities.
-
•
Pubic bones and urogenital structures develop from mesoderm.
-
•
Somatic mutations may be responsible for developmental abnormalities of mesoderm.
-
•
An isolated X-ray finding of ramus pubis agenesis may be associated with cryptorchidism.
Contributor Information
Yavuz Saglam, Email: yavuz_saglam@hotmail.com, nazifegamzeusta@gmail.com.
Murat Dursun, Email: mrt_drs@hotmail.com.
Goksel Dikmen, Email: gdkmen@yahoo.com.
Suleyman Bora Goksan, Email: sboragoksan@istanbul.edu.tr.
References
- 1.Francis C.C. Appearances of centers of ossification in the human pelvis before birth. Am J Roentgenol Radium Ther Nucl Med. 1951;65:778–783. [PubMed] [Google Scholar]
- 2.Sandomenico C., Tamburrini O. Bilateral accessory ossification center of the ischio-pubic synchondrosis in a female infant. Pediatr Radiol. 1981;10:233–236. doi: 10.1007/BF01001589. [DOI] [PubMed] [Google Scholar]
- 3.Sferopoulos N.K., Tsitouridis I. Ischiopubic hypoplasia: a rare constituent of congenital syndromes. Acta Orthop Belg. 2003;69:29–34. [PubMed] [Google Scholar]
- 4.Sarban S., Ozturk A., Iskan U.E. Aplasia of the pubic bone in conjunction with hip dislocation. J Pediatr Orthop B. 2005;14:266–268. doi: 10.1097/01202412-200507000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Sponseller P.D., Bisson L.J., Gearhart J.P., Jeffs R.D., Magid D., Fishman E. The anatomy of the pelvis in the exstrophy complex. J Bone Joint Surg Am. 1995;77A:177–189. doi: 10.2106/00004623-199502000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Yildiz C., Yurttas Y., Oto M., Kocaoglu M. Congenital agenesis of pubic bones: a case report. J Pediatr Orthop B. 2008;17(6):299–300. doi: 10.1097/BPB.0b013e328311d3e9. [DOI] [PubMed] [Google Scholar]