

Abstract
Objective:
To apply a novel postprocessing voxel-based analysis for diffusion tensor imaging of the cervical spinal cord in multiple sclerosis (MS) in a prospective cross-sectional study.
Methods:
Fourteen patients with MS who were within 4 weeks of the onset of cervical myelitis (lesion C1-3) and 11 healthy controls underwent cervical spinal cord diffusion tensor imaging. Cervical spinal cord maps of fractional anisotropy (FA), mean diffusivity, radial diffusivity (RD), and axial diffusivity were registered and compared between patients and controls. Mean FA and RD values from significant thresholded clusters were regressed with clinical scores, after adjusting for cord area and age, to determine associations with physical disability.
Results:
Cord registrations for subjects were qualitatively assessed (scored out of 5) and those with low scores (1 or 2) were excluded from further analysis. Cord registration was considered good in 11 patients (6 females; mean age = 35.5 years) and 10 controls (6 females; mean age 44 years). Voxel-based comparisons showed patients with MS had lower FA and higher RD at C2-3 levels (left >right mainly in gray matter; p < 0.01, uncorrected). Extracted values of both FA and RD from thresholded clusters were significantly associated with greater disability measured using the Expanded Disability Status Scale and Timed 25-Foot Walk Test in patients with MS.
Conclusions:
Mapping diffusion abnormalities within the cervical spinal cord using a novel voxel-based approach can localize clinically relevant pathology.
Most studies reporting multiple sclerosis (MS)-related diffusion tensor imaging (DTI) changes in the cervical spinal cord have utilized region-of-interest or histogram-based analyses.1–3 Voxel-based analysis is technically challenging because of difficulties with registration due to the cord's small diameter and relative lack of spatial features4 but can spatially localize abnormalities in an unbiased manner and can direct region-of-interest analyses to investigate clinicopathologic correlations, effectively providing greater statistical power. Clinically, localizing pathology to specific tracts may help to predict long-term clinical motor or sensory disability and guide treatment trials. As an early step toward this goal, we present findings from a novel postprocessing DTI voxel-based analysis for people with MS-related acute cervical myelitis. We hypothesized that fractional anisotropy (FA) reductions are spatially localized in the cord and correlate with measures of disability.
METHODS
We recruited 14 patients with MS who attended the MS outpatient clinic from 2005 to 2006 at the National Hospital for Neurology and Neurosurgery, London, UK, with acute motor and sensory signs attributable to at least one cervical lesion between C1-3 on conventional MRI. The clinical and radiologic characteristics of these patients have been previously described.3 Eleven age- and sex-matched healthy controls were also recruited.
Subject assessment.
Patients underwent neurologic examination and the following measures: Expanded Disability Status Scale (EDSS), 9-Hole Peg Test, Timed 25-Foot Walk Test (TWT), and Multiple Sclerosis Walking Scale (MSWS). The inverse of the average of 2 trials for each hand for the 9-Hole Peg Test (iNHPT) and the inverse of the mean of 2 trials for the TWT (iTWT) were used for data analysis. All subjects underwent cervical spinal cord structural MRI and cardiac-gated DTI (1 × 1 × 5 mm) on a 1.5T GE scanner (see appendix e-1 on the Neurology® Web site at Neurology.org).
Data analysis.
This is described in more detail in appendix e-1. In brief, we constructed a b0 cord template for cervical levels C1-5 from both patients and controls in a 2-step procedure (figures e-1 and e-2). We then registered each native b0 image to this b0 template and applied the individual transformation matrices to register individual FA, mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD) maps into common stereotactic space (defined by the b0 template) (http://fsl.fmrib.ox.ac.uk/fsl). The registered images were smoothed (2 × 2 × 10 mm3) and entered into a voxel-based nonparametric permutation-based analysis using threshold-free cluster enhancement to assess differences between patients and healthy controls (p < 0.01, uncorrected). An uncorrected threshold was chosen because our study was exploratory in using a novel technique and sample sizes were relatively small.
Post hoc, we extracted the mean FA and RD values from voxels common to both FA and RD differences (p < 0.01) in the cord (figure 1) and compared them between patients and controls using the Mann–Whitney U test in STATA 13.0 (StataCorp, College Station, TX). AD and MD values were not extracted post hoc because differences did not survive statistical threshold (p < 0.01).
Figure 1. Differences in diffusion parameters between patients and controls.
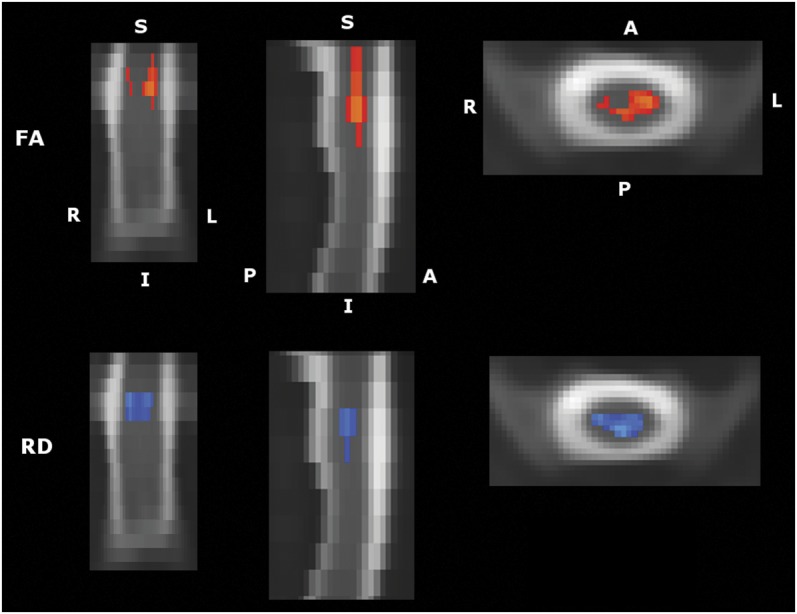
Significant differences in FA and RD between patients (n = 11; 6 females; mean age 35.5 ± 8.2 years) and healthy controls (n = 10; 6 females; mean age 44 ± 12.2 years). The cervical region with significant differences between patients and controls are shown. Clusters are shown in coronal, sagittal, and axial views, viewed from left to right, respectively. Significance is taken at p < 0.01, uncorrected. A = axial; FA = fractional anisotropy; I = inferior; L = left; P = posterior; R = right; RD = radial diffusivity; S = superior.
Associations between extracted mean FA and RD values and disability measures (iTWT, iNHPT, MSWS, EDSS) were investigated with (1) Spearman correlations, and (2) linear regression analysis, adjusting for age, sex, and cord area, for EDSS using a nonparametric bootstrapped regression.
Standard protocol approvals, registrations, and patient consents.
All subjects gave informed, written consent, and the study was approved by the local institutional research ethics board.
RESULTS
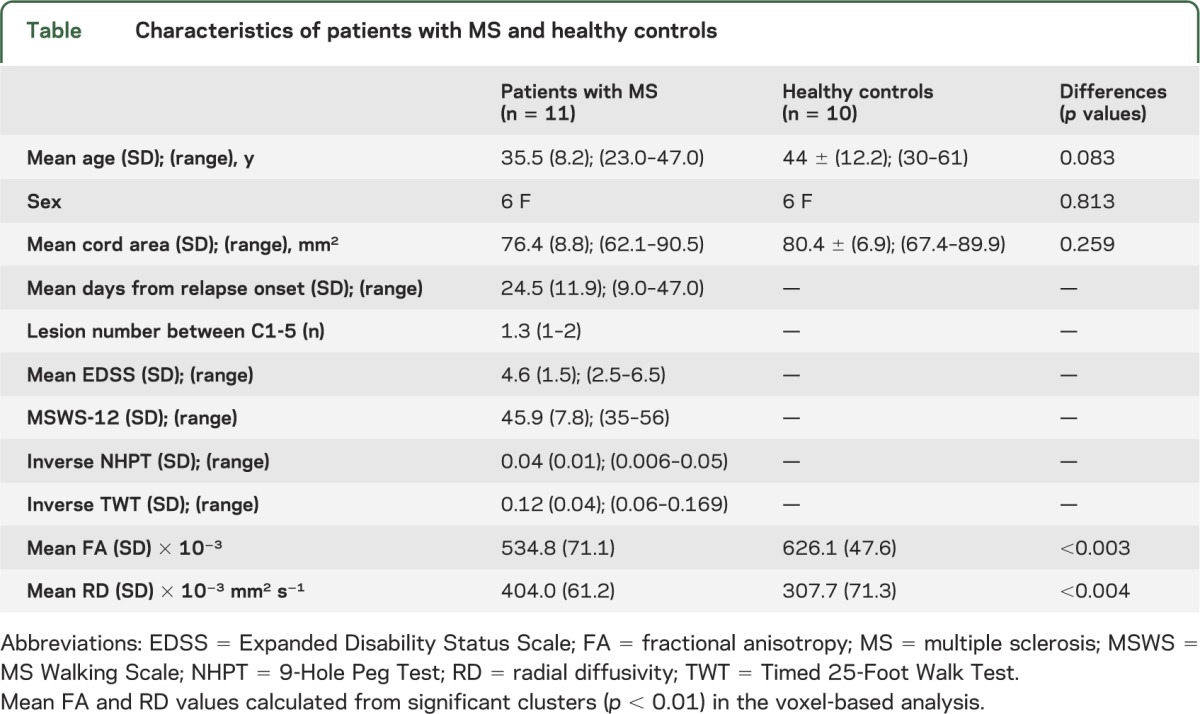
Eleven patients with MS (6 females; mean age 35.5 years) and 10 healthy subjects (6 females; mean age 44 years) were analyzed after cord registration (3/14 MS and 1/11 healthy subjects could not be registered accurately and were excluded). Subject characteristics are detailed in the table.
Table.
Characteristics of patients with MS and healthy controls
Differences between patients and controls.
After voxel-based analysis, patients showed lower FA at C2-3 than controls, predominantly in the left hemicord, extending across to the right (p < 0.01, uncorrected). These changes in FA were driven by higher RD in patients with MS than controls, which was detected at the same level, mainly in the central cord (figure 1). AD was not significantly different between groups. Voxel-based analysis also revealed higher MD in patients with MS at the same level (figure e-3), but with lower significance (p < 0.05, uncorrected); hence, MD values were not extracted for the post hoc analysis of clinical associations. It is likely that these changes seen for FA, RD, and MD resulted from the presence of lesions causing the acute relapse at the same levels.
Patients' mean RD values extracted from the overlapping thresholded clusters were significantly higher than controls' (404 vs 308 × 10−3 mm2 s−1, p < 0.005). This was likely to explain the lower mean extracted FA found in patients with MS (table [535 vs 626, p < 0.005]).
Associations between extracted DTI metrics and disability.
Spearman correlations showed that lower FA and higher RD were significantly associated with greater disability, measured using EDSS and iTWT (RD vs iTWT showed borderline significance at p = 0.054) (figure 2).
Figure 2. Significant correlations between diffusion and clinical metrics.

(A) Relation between FA and EDSS (R = −0.605; p = 0.049). (B) FA and iTWT (R = 0.721; p = 0.019). (C) Relation between RD and EDSS (R = 0.744; p = 0.009). (D) RD and iTWT (R = −0.624; p = 0.054). EDSS = Expanded Disability Status Scale; FA = fractional anisotropy; iTWT = inverse of Timed 25-Foot Walk Test; RD = radial diffusivity.
Regression modeling adjusting for age, sex, and cord area showed that lower FA was associated with greater disability measured using EDSS (p < 0.05, bootstrap) and iTWT (p = 0.034). Higher RD showed a borderline significant association with iTWT (p = 0.087). RD's association with EDSS became nonsignificant because of confounding by age (p > 0.05, bootstrap). No significant associations were found for iNHPT or MSWS and FA/RD.
DISCUSSION
We localized lower FA and higher RD in MS-related myelitis to specific regions of the cervical spinal cord. Extracted FA and RD were associated with greater disability (higher EDSS and lower iTWT scores), confirming the clinical relevance of our results. Spatially localizing diffusion differences in the cord with voxel-based analyses permits one to focus on pathologically relevant areas (without an a priori hypothesis) thereby improving the ability to detect clinically relevant associations. This technique can provide clinical and pathophysiologic insights into mechanisms of disability in MS and can be applied to other neurologic conditions with cord involvement. It may also lead to more accurate imaging biomarkers to monitor therapeutic treatments and help to predict clinical outcomes in future studies.
Associations between DTI metrics and spinal cord pathology have been reported by previous studies using region-of-interest analyses in MS and other conditions.2,3,5,6 Lower FA and higher RD are associated with pathologic alterations of tissue microstructure7,8 and correspond with greater motor impairment in vivo.2,3,6 Our study supplements these findings by spatially localizing these changes without relying on an a priori hypothesis.
Cervical spinal cord registration is challenging. The cord possesses smooth cylindrical morphology thus does not have as much information content as the brain, which has richer features associated with sulcal, gyral, and CSF spaces, making it less amenable to robust registration. Partial volume effects and cardiac/CSF-related inhomogeneities may also impair registration accuracy. Previous spinal cord voxel-based analyses have relied on sagittal-based registration.9 Axial imaging can provide higher cross-sectional resolution than sagittal imaging for anisotropic voxel dimensions. We defined upper and lower limits of C1 and C5 individually to maintain some degree of longitudinal anatomical correspondence.
The effect of smoothing should be considered. Smoothing can lead to less precise spatial inferences because of spatial blurring and this may be a particular issue at the gray matter–white matter interface. However, this should be balanced against the advantages that it provides. Registration is rarely 100% accurate, and there are likely to be small differences between subjects. Smoothing compensates for this. It also helps to increase signal to noise and, in parametric analyses, normalizes the data structure. Overall, it is likely that the advantages outweigh the loss in spatial resolving ability. In spinal cord DTI, the degree of smoothing required is not clear but must be chosen to balance the factors above. Anisotropic (vs isotropic) spatial filtering may be more sensitive and specific at detecting significant effects in DTI while preserving white matter boundaries.10
With further advances in image registration, voxel-based analyses should improve and complement a priori region-of-interest techniques in assessing spinal cord pathology.
Supplementary Material
GLOSSARY
- AD
axial diffusivity
- DTI
diffusion tensor imaging
- EDSS
Expanded Disability Status Scale
- FA
fractional anisotropy
- iNHPT
inverse of 9-Hole Peg Test
- iTWT
inverse of Timed 25-Foot Walk Test
- MD
mean diffusivity
- MS
multiple sclerosis
- MSWS
Multiple Sclerosis Walking Scale
- RD
radial diffusivity
- TWT
Timed 25-Foot Walk Test
Footnotes
Editorial, page 1306
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
Ahmed T. Toosy and Nancy Kou helped to draft and revise the manuscript, contributed to data and statistical analyses, and made intellectual contributions to the study. Daniel Altmann helped to revise the manuscript and contributed to statistical analyses. Claudia A.M. Wheeler-Kingshott helped to revise the manuscript and design the magnetic resonance sequences, and made intellectual contributions to the study. Alan J. Thompson helped to revise the manuscript and made intellectual contributions to the study. Olga Ciccarelli helped to revise the manuscript, acquired the data, contributed to data and statistical analyses, and made intellectual contributions to the study.
STUDY FUNDING
A.T.T. is supported by the Higher Education Funding Council for England. This research study was funded by the Wellcome Trust, grant 074618/Z/04, the Engineering and Physical Sciences Research Council, grant EP/I027084/1, and the International Research Spinal Trust, grant NRB104, and was supported by the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
DISCLOSURE
A. Toosy has received honoraria from Serono Symposia International Foundation and Bayer. N. Kou reports no disclosures relevant to the manuscript. D. Altmann has received an honorarium from Merck & Co., Inc., and gave expert testimony in the case of Mylan v. Yeda. C.A.M. Wheeler-Kingshott receives research funding from drug companies for clinical trials (Biogen Idec, Novartis) and in the past has received honoraria from Biogen Idec and Philips Healthcare for lectures and consultancies. She is on the editorial board of Functional Neurology. A. Thompson has received honoraria and support for travel for consultancy from Genzyme and Teva; honorarium for consultancy from BTG International; honorarium to UCL for board membership from Eisai; honoraria and support for travel for lecturing from Serono Symposia International Foundation, Teva, Novartis, and Remedica. Alan Thompson is a board member for Imanova, chair of the MSIF International Medical and Scientific Board, member of the NMSS Research Programs Advisory Committee, editor-in-chief for Multiple Sclerosis Journal (for which he receives an honorarium), and a member of the editorial board for The Lancet Neurology (for which he receives a free subscription). O. Ciccarelli is on the editorial board of Neurology® and Multiple Sclerosis Journal; she serves as consultant for Biogen, General Electric, and Novartis; and she receives research support from UK MS Society, UCL/UCLH NIHR BRC, and EPSRC. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Agosta F, Absinta M, Sormani MP, et al. In vivo assessment of cervical cord damage in MS patients: a longitudinal diffusion tensor MRI study. Brain 2007;130:2211–2219 [DOI] [PubMed] [Google Scholar]
- 2.Freund P, Wheeler-Kingshott C, Jackson J, Miller D, Thompson A, Ciccarelli O. Recovery after spinal cord relapse in multiple sclerosis is predicted by radial diffusivity. Mult Scler 2010;16:1193–1202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ciccarelli O, Wheeler-Kingshott CA, McLean MA, et al. Spinal cord spectroscopy and diffusion-based tractography to assess acute disability in multiple sclerosis. Brain 2007;130:2220–2231 [DOI] [PubMed] [Google Scholar]
- 4.Mohammadi S, Freund P, Feiweier T, Curt A, Weiskopf N. The impact of post-processing on spinal cord diffusion tensor imaging. Neuroimage 2013;70:377–385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Freund P, Schneider T, Nagy Z, et al. Degeneration of the injured cervical cord is associated with remote changes in corticospinal tract integrity and upper limb impairment. PLoS One 2012;7:e51729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Naismith RT, Xu J, Klawiter EC, et al. Spinal cord tract diffusion tensor imaging reveals disability substrate in demyelinating disease. Neurology 2013;80:2201–2209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kim JH, Budde MD, Liang HF, et al. Detecting axon damage in spinal cord from a mouse model of multiple sclerosis. Neurobiol Dis 2006;21:626–632 [DOI] [PubMed] [Google Scholar]
- 8.Klawiter EC, Schmidt RE, Trinkaus K, et al. Radial diffusivity predicts demyelination in ex vivo multiple sclerosis spinal cords. Neuroimage 2011;55:1454–1460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rocca MA, Valsasina P, Damjanovic D, et al. Voxel-wise mapping of cervical cord damage in multiple sclerosis patients with different clinical phenotypes. J Neurol Neurosurg Psychiatry 2013;84:35–41 [DOI] [PubMed] [Google Scholar]
- 10.Van Hecke W, Leemans A, De Backer S, Jeurissen B, Parizel PM, Sijbers J. Comparing isotropic and anisotropic smoothing for voxel-based DTI analyses: a simulation study. Hum Brain Mapp 2010;31:98–114 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.