

Abstract
Rhabdomyoma, a benign hamartomatous tumor of the cardiac embryonic myocyte, is the most common intrauterine cardiac tumor and accounts for 0.12% of prenatal fetal studies. Fetal cardiac rhabdomyomas increase in size during second and early third trimester and spontaneously regress postnatally. The clinical presentation is usually benign, however, compromise of the ventricular outflow tract leading to decreased cardiac output and fetal death have been reported. We present a case of large cardiac rhabdomyoma in a fetus that might have caused complete left ventricular outflow tract obstruction and development of hypoplastic left heart syndrome (HLHS) necessitating postnatal single ventricle palliation therapy. The clinical course and outcomes of prenatally diagnosed cardiac rhabdomyoma are reviewed and theories of the development of hypoplastic left heart syndrome are explored.
Keywords: Cardiac tumor, hypoplastic left heart syndrome (HLHS), rhabdomyoma
INTRODUCTION
Rhabdomyomas, benign hamartomatous tumors of cardiac myocytes, are the most common cardiac tumors diagnosed in both fetal and early postnatal life with an incidence of 0.02-0.08 percent of live born infants.[1] Cardiac rhabdomyomas (CR) account for 60-86% of primary cardiac tumors diagnosed in the fetus.[1] The natural history of CR after birth is spontaneous regression with more than half of the patients demonstrating partial or complete regression within 5 years.[1,2] In utero spontaneous regression can occur[2] , however, an increase in size, particularly during second and early third trimester due to the influence of maternal hormones, is more frequent.[2,3,4] The clinical course of CR is often benign, however, arrhythmia, compromise of the ventricular outflow tract leading to decreased cardiac output, and fetal death have been reported.[4,5,6] We present a case of large left ventricular (LV) rhabdomyoma that might have occluded the LV outflow tract during fetal life and resulted in hypoplastic left heart syndrome (HLHS). To our knowledge, this is the first case report of successful single ventricle palliation in a patient with HLHS caused by a large CR.
CASE REPORT
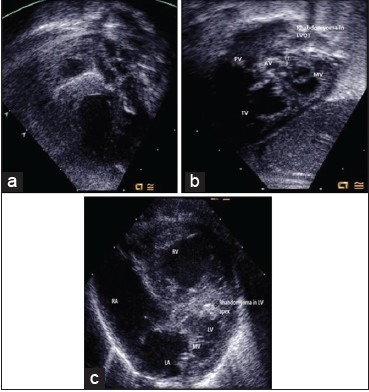
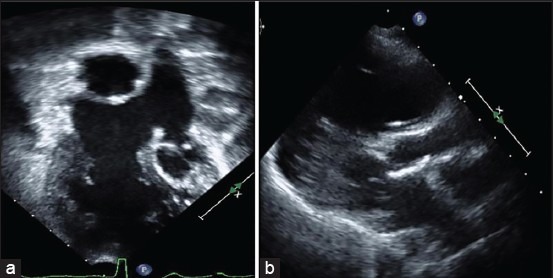
A 19-year-old gravida 1 diabetic mother with no family history of seizures or tuberous sclerosis was noted to have, on fetal echocardiogram at 25 weeks gestation, two large, homogenous, oval echogenic mass in the LV [Figure 1a]. One mass obstructed mitral valve inflow [Figure 1a and c], and there was no flow in the left ventricular outflow tract (LVOT) to the aortic valve. The additional CR was noted in the ventricular septum beneath the aortic valve (Figure 1b). Mild LV hypoplasia with moderately diminished LV systolic function was noted (Figure 1c). The tricuspid and pulmonary valves measured normal for gestational age and demonstrated normal Doppler patterns. However, the mitral and aortic valves measured small for gestational age and there was appropriate right to left shunting across the ductus arteriosus, but inappropriate retrograde filling of the ascending aorta consistent with HLHS physiology. Fetal Echo at 32 weeks gestation showed a hypoplastic LV and inappropriate left to right shunting across the foramen ovale [Figure 2]. There was no history of fetal arrhythmia or hydrops and the fetus was delivered by inducing labor at 38 weeks gestation. Prostaglandins were started for ductal patency and a postnatal Echo confirmed the diagnosis of HLHS. A large LVOT CR causing complete LVOT obstruction [Figure 3a and b] and additional small rhabdomyomas in the LV apex and free wall were noted (3c). No neuro-cutaneous markers of tuberous sclerosis were noted. On day 11 of life, he underwent a successful Norwood-Sano procedure followed by right bidirectional Glenn procedure at 5 months of age. The large LV tumor occluding the LV inflow and outflow tract had resolved by 5 months of age, however, several smaller tumors in the interventricular septum and free wall were still present. Repeat brain MRI performed a few months after Glenn palliation showed no evidence of cranial tumors. At age of 2 years, he underwent a fenestrated lateral tunnel Fontan with left pulmonary arterioplasty. Follow-up Echo showed resolution of the multiple small tumors in the interventricular septum and his most recent echocardiogram at 6-years of age shows resolution of tumors in LVOT [Figure 4a and b]. The patient did not have any evidence of tuberous sclerosis by examination or neuroimaging at his most recent follow-up.
Figure 1.
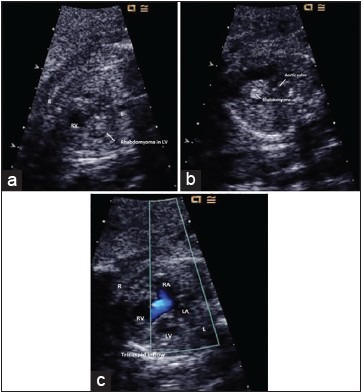
(a) shows a large rhabdomyoma in the left ventricle. (b) shows an additional small rhabdomyoma in the ventricular septum. (c) shows normal tricuspid inflow and absence of mitral inflow
Figure 2.

Abnormal red color flow across the patent foramen ovale consistent with left to right shunting seen in HLHS
Figure 3.
(a and b) show a large rhabdomyoma at birth occluding left ventricular outflow tract. Additional LV apical rhabdomyoma seen in the LV apex in 3C. (c) shows a moderately hypoplastic non apex forming LV with hypoplastic mitral valve
Figure 4.
(a) Is an apical 4 chamber view still frame showing the Fontan baffle and hypoplastic LV with resolution of LV rhabdomyoma. (b) is parasternal long axis still frame showing resolution of LV outflow tumor
DISCUSSION
Cardiac rhabdomyomas are homogenous, diffusely echogenic round or oval masses most commonly found in the interventricular septum, RV or LV free wall, and occasionally found in either atria.[1] The tumors can be single or multiple. Multiple tumors are more likely to be associated with a diagnosis of tuberous sclerosis. A large single center series reported a prevalence of tuberous sclerosis of 78% (68/87) among patients diagnosed in the fetal or neonatal period with any ventricular tumor.[2] In the largest single center study, 43% (3/7) patients with a fetal diagnosis of a single ventricular tumor had a diagnosis of tuberous sclerosis by 1-year of age, whereas, 91% (30/33) with multiple ventricular tumors had a diagnosis of tuberous sclerosis.[2] A meta-analysis of the literature reports a 78% perinatal survival rate among prenatally diagnosed CR.[7,8] Fetal MRI can be helpful in the prenatal diagnosis of tuberous sclerosis as tumors in the brain may be detected, however, a normal fetal MRI does not exclude the diagnosis of tuberous sclerosis as brain abnormalities often develop later in infancy.[3,8] Factor associated with perinatal death included hydrops, tumor size, and dysrhythmia.[7,8] Other abnormalities reported with a fetal diagnosis of CR have included intractable arrhythmia, tetralogy of Fallot, Ebstein malformation, trisomy 21, cleft palate, polycystic kidney, and club foot.[8]
The proposed mechanism of the development of HLHS is a restrictive foramen ovale in utero.[9] This case, however, suggests another intriguing hypothesis for the development of HLHS. Interference with blood flow out of the outflow tract early in gestation may have led to hypoplasia of ventricle and no outflow across the aortic valve to hypoplasia of the ascending aorta. This has been documented in an experimental model of chick embryo with the surgical placement of the nylon device in the left atrio-ventricular region.[3] Is there a causal relationship between a large occlusive LVOT rhabdomyoma and HLHS or is it a mere association? One can surmise that the lack of antegrade blood flow across the aortic valve early in gestation led to the arrest in the growth of the left heart structures in this case, however, there have been case reports of critical left ventricular outflow tract obstruction requiring surgical removal that have not led to HLHS.[10] Irrespective of the causal relationship, this case report highlights the importance to recognize and evaluate for HLHS in the presence of a large occlusive LVOT rhabdomyoma, for appropriate management of the patient in the immediate postnatal period. Several case reports have suggested that location, rather than size is the critical factor in prognosis for cardiac rhabdomyoma.[3,10] This case report highlights the importance of the location of cardiac rhabdomyoma and the associated potentially lethal complications. Delivery of the fetus and surgical excision should be considered in fetus with a large inflow or outflow tract CR, and single ventricle palliation may be considered as an option, particularly when not associated with tuberous sclerosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Fesslova V, Villa L, Rizzuti T, Mastrangelo M, Mosca F. Natural history and long-term outcome of cardiac rhabdomyomas detected prenatally. Prenat Diag. 2004;24:241–8. doi: 10.1002/pd.825. [DOI] [PubMed] [Google Scholar]
- 2.Tworetzky W, McElhinney DB, Margossian R. Association between cardiac tumors and tuberous sclerosis in the fetus and neonate. Am J Cardiol. 2003;92:487–9. doi: 10.1016/s0002-9149(03)00677-5. [DOI] [PubMed] [Google Scholar]
- 3.Watanabe T, Hojo Y, Kozaki T, Nagshima M, Ando M. Hypoplastic left heart syndrome with rhabdomyoma of the left ventricle. Pediatr Cardiology. 1991;12:121–2. doi: 10.1007/BF02238418. [DOI] [PubMed] [Google Scholar]
- 4.Nir A, Ekstein S, Nadjari M, Raas-Rothschild A, Rein AJ. Rhabdomyoma in the fetus: Illustration of tumor growth during the second half of gestation. Pediatr Cardiol. 2001;22:515–8. doi: 10.1007/s002460010287. [DOI] [PubMed] [Google Scholar]
- 5.Ibrahim CP, Thankker P, Miller PA, Barron D. Cardiac rhabdomyomas presenting as left ventricular outflow tract obstruction in a neonate. Interact Cardiovasc Thorac Surg. 2003;2:572–4. doi: 10.1016/S1569-9293(03)00150-6. [DOI] [PubMed] [Google Scholar]
- 6.Sharma J, Inglis S, Cavalieri R, Udom-Rice I. Fetal demise secondary to massive rhabdomyoma in the early second trimester of pregnancy. Pediatr Cardiol. 2011;32:243–4. doi: 10.1007/s00246-010-9874-7. [DOI] [PubMed] [Google Scholar]
- 7.Jozwiak S, Kotulska K. Are all prenatally diagnosed multiple cardiac rhabdomyomas a sign of tuberous sclerosis? Prenat Diag. 2006;26:866–77. doi: 10.1002/pd.1506. [DOI] [PubMed] [Google Scholar]
- 8.Chao AS, Chao A, Wang TH, Chang YC, Chang YL, Hsieh CC, et al. Outcome of antenatally diagnosed cardiac rhabdomyoma: Case series and a meta-analysis. Ultrasound Obstet Gynecol. 2008;31:289–95. doi: 10.1002/uog.5264. [DOI] [PubMed] [Google Scholar]
- 9.Nowlen TT, Ayres NA, Kearney DL, Nihill MR, Grifka RG. Premature closure of the foramen ovale associated with aortic stenosis, left ventricular dilation with thrombus, and early mortality. Am J Cardiol. 2000;85:1159–61, A9. doi: 10.1016/s0002-9149(00)00718-9. [DOI] [PubMed] [Google Scholar]
- 10.Ikemba CM, Eidem BW, Dimas VV, O’Day MP, Fraser CD. Fetal rhabdomyoma causing postnatal critical left ventricular outflow tract obstruction. Ann Thorac Surg. 2005;80:1529. doi: 10.1016/j.athoracsur.2003.10.095. [DOI] [PubMed] [Google Scholar]