

Abstract
If the patient has antibody to low incidence antigen providing compatible blood for transfusion is not a problem. It is however necessary to identify such antibodies to assess their potential to cause hemolytic transfusion reaction and hemolytic disease of newborn. We identified anti Cw in patient’s serum while investigating the cause of incompatible cross match in a female thalassemia patient. Anti Cw is an antibody against Cw (Rh8) antigen, which is a low incidence antigen of Rh system. This case also prompted us to study frequency of Cw antigen in our donor population as the frequency of Cw antigens in our population is not reported. Frequency of Cw antigens in north Indian donors was found to be 1.2 %.
Keywords: Rh–Hr blood group system, Rh immunization, Pregnancy complications
Introduction
During compatibility testing if patient’s serum is found incompatible with only one donor unit, the possible causes could be ABO incompatible/DAT positive/polyagglutinable donor red cells or antibody to low incidence antigen in patient’s serum [1]. If the patient has antibody to low incidence antigen providing compatible blood for transfusion is not a problem. It is however necessary to identify such antibodies to assess their potential to cause hemolytic transfusion reaction (HTR) and hemolytic disease of newborn (HDN). Also in multitransfused patients these antibodies may complicate the identification of other clinically significant antibodies. It is also of academic interest to identify such antibodies and antigens as many of the new low incidence antigens are discovered in this manner.
We identified anti Cw in patient’s serum while investigating the cause of incompatible crossmatch in a female thalassemia patient. Anti Cw is an antibody against Cw (Rh8) antigen, which is a low incidence antigen of Rh system [2]. This case, also prompted us to study frequency of Cw antigen in our donor population as the frequency of Cw antigens in our population is not reported. We also reviewed literature with regards to its potential to cause HDN as the patient was a young female of child bearing age group.
Case Report with Results
Two units of packed red cells were crossmatched for B positive 18 years old female thalassemia major patient by AHG gel technique at our institution. One unit these was found incompatible (3+), however second unit was fully compatible. Cross match was compatible by saline technique at room temperature. Five another B+ units crossmatched for the patient were also found to be compatible. Two units of compatible blood were issued for the patient and incompatible crossmatch was further worked up.
On further investigations incompatible blood donor unit red cells were found to be Direct antiglobulin test negative (AHG gel column agglutination test: Diamed GmbH, Cressier, Switzerland), B positive on repeat blood grouping (ABO compatible) and not agglutinated by sera of group AB donors (polyagglutination negative).
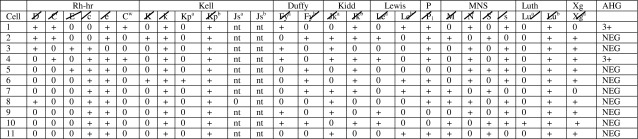
Results of antibody screening and antibody identification done on patient’s serum using ID Diacell I-II-II and ID-Diapanel (Diamed GmbH, Cressier, Switzerland) by AHG gel technique are shown in Table 1 and 2. Anti CW was identified in the patient’s serum. It also reacted with Cw positive cells from another lot of ID-Diapanel prepared from different set of donors and donor red cells identified as Cw positive at our center on typing of 163 donors for this study. Anti Cw titer in patient’s serum was found to be 16. As this is a rare antibody aliquots of plasma from all subsequent blood samples sent for pretransfusion testing were preserved frozen.
Table 1.
Results of testing patient’s serum with reagent red cell panel for antibody screening

The crossed out antigens are ruled out and probability of antibody specificity being either anti C, anti Cw or anti Lu a remains
Superscript letter a and b denote the alleles of antigen
Table 2.
Results of testing patients serum with reagent red cell panel for antibody identification
Anti Cw is the only probable antibody as the rest have been crossed out
Superscript letter a and b denote the alleles of antigen
The incompatible donor unit was found to be CW antigen positive by commercially available anti CW anti sera (Diamed GmbH, Cressier, Switzerland). Aliquots from CW positive donor red cell unit were preserved using 40 % glycerol at −80 °C. The donor of incompatible blood unit was from Eastern India, whereas our center is located in central India.
Patient’s red cells were found to be negative for CW antigen. This patient has been regularly transfused since the age of 6 months and has received >300 transfusions so far mostly at other centers. She was registered at our center recently and had been found to be negative for red cell alloantibodies nine months ago on screening. In frequently transfused patients the red cell antigen phenotype may not represent the true phenotype of the patient due to presence of transfused donor red cells more so if the last transfusion has been within 2–3 weeks and molecular typing is confirmatory. However last transfusion in this patient had been 6 weeks ago. The Rh antigen phenotype of patient, incompatible unit and compatible unit was found to be CcDee, CcCWDee and CCDee respectively.
To find CW antigen frequency in north Indian donor population we typed 163 donors for CW antigen using commercially available anti Cw antisera from (Diamed GmbH, Cressier, Switzerland); two out of 163 (1.2 %) of these were found to be Cw antigen positive.
Discussion
The anti Cw identified in this case is most likely transfusion induced. Since in this case anti Cw was detected in a female patient of child bearing age group it was necessary to evaluate the antibody’s potential to cause HDN and advise accordingly although for transfusion purposes crossmatch compatible blood could have been be issued. This antibody may have been present in patient’s serum earlier also but as she was never screened for alloantibodies it remained undetected. It is essential that alloantibody screening should be done at scheduled intervals in frequently transfused patients in the Institution’s policy is to issue blood AHG compatible blood without antibody screening.
On literature search few case reports of mild to severe HDN caused by anti Cw were found. Table 3 summarizes the findings of reported studies. Anti Cw was first described in 1946 by Callender and race in a DCe/DCe multitransfused patient with systemic lupus erythematosus who had been transfused DCe/DCe Cw + red cells [2]. In 1947, Lawler and Loghem reported first anti CW associated HDN [3]. Since then there have been infrequent case reports on anti Cw associated moderate to severe HDN requiring intervention as summarized in Table 3 [3–12], demonstrating that pregnancies affected by anti Cw merit closer scrutiny.
Table 3.
Summary of outcome in reported pregnancies with anti Cw
| Reference | No of cases | Clinical outcome |
|---|---|---|
| Lawler and Loghem [3] | 1 | HDN |
| Anderson et al. [4] | 9 pregnancies in a anti Cw positive woman | First child normal, Cw positive |
| Second and third child (twins) had jaundice, Cw positive, required transfusion | ||
| Fourth child normal, Cw negative | ||
| Next four pregnancy miscarriage | ||
| Fifth child had jaundice, Cw positive, no transfusion required | ||
| Hughes et al. [5] | NM | Severe HDF, treated with phototherapy and exchange transfusion |
| Bowman et al. [6] | 14 pregnancies with acquired anti Cw (In 1 in 1,100 women treated during 36 years) | Three babies who were Cw negative- normal |
| 11 babies were Cw positive- DAT+had HDN | ||
| (Five no treatment required, two required phototherapy and four required exchange transfusion) | ||
| Reiner et al. [7] | 1 | Required phototherapy and exchange transfusion |
| Kollamparambil et al. [8] | NM | Severe HDF, fetus had hydrops. |
| Byers et al. [9] | 1 | Severe fetal anemia requiring intrauterine transfusion |
| May-Wewers et al. [10] | 1 | Severe neonatal anemia |
| Chu et al. [11] | NM | History of previous IUD and bad obstetrics history. Presenting pregnancy had HDN and neonate required exchange transfusion |
| Malik [12] | 1 (Primi) | Normal baby |
| 1 (4th gravida) | Normal baby | |
| 1 (Primi) | NM |
DAT direct ant globulin test, NM not mentioned, IUD intra uterine transfusion, HDF hemolytic disease of fetus, HDN hemolytic disease of newborn
Table 4 shows the Cw antigen frequency in this study in comparison to that reported from other parts of world. As seen in Table 4 the frequency of Cw antigen is reported to be 1–3 % in most of the populations with exception of Finns, Lapps and Latvians where the frequency is reported to be higher. The reported frequency of Cw antigen among Caucasians and blacks is reported to be 2 and 1 % respectively [13]. It is more frequent in Latvians (7 %) and Finns (4 %) [14].
Table 4.
Cw antigen frequency in different populations
| Reference | Population | Antigenic frequency of Cw (%) |
|---|---|---|
| Reid [13] | Caucasians | 2 |
| Reid [13] | Black | 1 |
| Race [14] | Latvians | 9 |
| Race [14] | Finns | 4 |
| Race [15] | English | 2.6 |
| Simic [16] | Serbian | 3.5 |
| Sarentopolous et al. [17] | Greek | 1.48 |
| Kornstad [18] | Oslo | 2.98 |
| Frequency of CW antigen | Blood donors in Northern Central India | 1.25 |
In view of clinical significance of anti Cw antibody the patient was provided an antibody card for reference. It was also decided to issue crossmatch compatible blood for further transfusions and monitor antibody titre. Since patient was of child bearing age group she and her parents were counseled regarding anti Cw antibody’s potential to cause HDN and HTR and their prevention.
In certain countries however, it is reported that a Cw positive cell is typically not included in a set of screening cells and thus anti Cw may be missed on antibody screening although Cw positive cell is included on antibody identification panel from most manufacturers [19].
Conclusion
We suggest that Cw antigen positive antibody screening cells should be used for antibody screening in pregnant women as these antibodies may not be as infrequent as they are thought to be and can result in clinically significant HDN. Also if these antibodies are identified, titer in maternal serum and assessment of fetal well being should be done aggressively.
This case illustrates that work of a transfusion service does not end with providing compatible blood as work up of incompatible cross match led us to detection of antibody to low frequency antigen in the patient’s serum and prompted us to study the antigen frequency in our region. This approach may have far reaching consequences for the patient and growth of science.
Conflict of Interest
The authors declare no conflict of interest. Consent of patient and Institutional ethics committee approval for anonymous publication taken.
References
- 1.Walker PS. Identification of antibodies to red cell antigens. In: Roback JD, Grossman BJ, Harris T, Hillyer CD, editors. Technical manual . 17. Maryland: AABB Bethesda; 2011. p. 487. [Google Scholar]
- 2.Callender ST, Race RR. A serological and genetical study of multiple antibodies formed in response to blood transfusion by a patient with lupus erythematosus diffusus. Ann Eugen. 1946;13:102. doi: 10.1111/j.1469-1809.1946.tb02346.x. [DOI] [PubMed] [Google Scholar]
- 3.Lawler SD, Van Loghem JJ., Jr The rhesus antigen CW causing haemolytic disease of the newborn. Lancet. 1947;2:545. doi: 10.1016/S0140-6736(47)90587-4. [DOI] [PubMed] [Google Scholar]
- 4.Anderson GH, Fenton E. A case of anti-Cw sensitization resulting in hemolytic disease of the newborn. Can Med Assoc J. 1963;89:28. [PMC free article] [PubMed] [Google Scholar]
- 5.Hughes W, Pussell P, Klarkowski D. Haemolytic disease of the newborn associated with anti Cw. Aust N Z J Obstet Gynaecol. 1982;22:161–162. doi: 10.1111/j.1479-828X.1982.tb01433.x. [DOI] [PubMed] [Google Scholar]
- 6.Bowman JM, Pollock J. Maternal Cw Alloimmunization. Vox Sang. 1993;64:226–230. doi: 10.1111/j.1423-0410.1993.tb03060.x. [DOI] [PubMed] [Google Scholar]
- 7.Reiner AP, Teramura G, Aramaki KM. Use of PCR based assay for fetal Cw antigen genotyping in a patient with history of moderately severe hemolytic disease of newborn. Am J Perinatol. 1999;16:277–281. doi: 10.1055/s-2007-993872. [DOI] [PubMed] [Google Scholar]
- 8.Kollamparambil TG, Jani BR, Aldouri M, Soe A, Ducker DA. Anti-C(w) alloimmunization presenting as hydrops fetalis. Acta Paediatr. 2005;94:499–501. doi: 10.1111/j.1651-2227.2005.tb01924.x. [DOI] [PubMed] [Google Scholar]
- 9.Byers BD, Gordon MC, Higby K. Severe hemolytic disease of the newborn due to anti-Cw. Obstet Gynecol. 2005;106:1180–1182. doi: 10.1097/01.AOG.0000164060.89842.a9. [DOI] [PubMed] [Google Scholar]
- 10.May-Wewers J, Kaiser JR, Moore EK, Blackall DP. Severe neonatal hemolysis due to maternal antibody to low frequency Rh antigen C(w) Am J Perinatol. 2006;23:213–217. doi: 10.1055/s-2006-934098. [DOI] [PubMed] [Google Scholar]
- 11.Chu H-P, Kanagalingam D, Chan DK-L. Severe intrauterine hemolysis due to anti-Cw. Am J Perinatol. 2007;24:623–626. doi: 10.1055/s-2007-992176. [DOI] [PubMed] [Google Scholar]
- 12.Malik S, Moiz B. Clinical significance of maternal anti-Cw antibodies: a review of three cases and literature. J Pak Med Assoc. 2012;62:620–621. [PubMed] [Google Scholar]
- 13.Reid ME, Lomas-Francis C. The blood group antigen: facts book. San Diego: Academic Press; 2004. The blood group system and antigen; pp. 111–112. [Google Scholar]
- 14.Race RR, Sanger R. Blood Groups in Man. Oxford: Blackwell Scientific Publications; 1975. [Google Scholar]
- 15.Race RR, Mourant AE, Lawler SD, Sanger R. The Rh chromosome frequencies in England. Blood. 1948;3:689–695. [PubMed] [Google Scholar]
- 16.Simic S (1975) Frequency of Cw antigens. Bilt Hematol Transfuz 3:73–76 [PubMed]
- 17.Sarantopolous AA, Gavalaki M, Kotsi P, Adraktas T et al (2014). Detection of CW antigen of the Rhesus blood system in Greek blood donors with a novel method for simultaneous typing of ABO, D, Rhesus subgroups and K (MDmulticard). Available at http://www.medion-diagnostics.ch/images/pev_20080604_2.pdf. Accessed 05 Feb 2014
- 18.Kornstad Leif. The frequency of the Rh Antigen Cw in 2750 Oslo blood donors. Vox Sang. 1959;4:225–230. doi: 10.1111/j.1423-0410.1959.tb05131.x. [DOI] [PubMed] [Google Scholar]
- 19.Antibody identification-anti Cw case study. Available at http://www.api-pt.com/Reference/Specialtopics/11A-EDU-01_BBank.pdf. Accessed on 05 Feb 2014