

Abstract
Hairy cell leukemia (HCL) is characterized by pancytopenia and usually associated with massive splenomegaly, however the same may not be true in the clinical settings. Here we report four cases of HCL and all of them were without the classical clinical feature of splenomegaly. This is an observational study conducted between January 2013 to March 2014 where we could diagnose ten cases of HCL in Department of Hematology, All India Institute of Medical Sciences, New Delhi. Of these, four cases attracted attention because of absence of classical clinical features of HCL. Of the four cases, three presented with weakness/fatigability while fourth patient presented with recurrent respiratory tract infection. Surprising finding in these cases was absence of splenomegaly, both clinically and on imaging which demerit the suspicion of HCL clinically. All four had bi/pancytopenia and bone marrow examination coupled with immunophenotypic analysis confirmed the diagnosis of HCL. Three patients received chemotherapy with cladribine and achieved complete hematological remission. One patient did not receive chemotherapy due to poor general condition and was subsequently lost to follow up. To conclude, HCL can and do present without splenomegaly and this should not restrain one from suspecting HCL based on histomorphology which needs to be further confirmed by ancillary techniques. This finding in our series could be because these cases were picked early in their natural course of the disease. A high index of suspicion is essential for diagnosing and appropriately managing such cases.
Keywords: Hairy cell leukemia, Splenomegaly, Hypoplastic marrow, Aplastic anemia, Cladribine
Introduction
Hairy cell leukemia (HCL) is an uncommon but distinct form of chronic B cell lymphoproliferative disorder, comprising about two percent of lymphoid leukemias. Patients are predominantly middle-aged to elderly adults with a median age of 50 years and is characterized by pancytopenia, monocytopenia and splenomegaly. The major sites of disease involvement are bone marrow and spleen with rare or only a small number of leukemic cells in the peripheral blood [1].
In past, various case series have quoted the incidence of splenomegaly, which ranged from 70 to 100 % in cases of HCL [2–7]. Splenomegaly is a prominent feature in HCL with many otherwise asymptomatic patients seeking medical attention because of awareness of mass. At times the absence of splenomegaly takes away the clinical suspicion in a case of HCL and misdiagnosed as aplastic anemia as happened in one of the cases brought out in this series, delaying the diagnosis and appropriate specific management. The aim of this present communication is to highlight the importance to have high index of suspicion to consider a diagnosis of HCL based on histomorphological features even in the absence of classical clinical features. In this case series it was noticed that four out of ten (40 %) diagnosed cases of HCL during past fifteen months did not show splenomegaly both clinically and on radiological investigations. This had definitely put us in diagnostic dilemma of a morphological diagnosis of HCL till the immunophenotyping could confirm diagnosis. We present here the clinical and laboratory features, along with therapy given and their response for these four cases.
Case 1
A 69 years old diabetic male presented with one and half month history of weakness and fatigability. He also had history of renal calculus and hemorrhoids. In the past he had received packed RBCs nine times. On examination, he had pallor; however had no organomegaly or lymphadenopathy. Hemogram showed pancytopenia with Hb nine gm/dl, TLC 1240/cumm and platelet count of 53,000/cumm. His peripheral smear did not show any atypical cells. With clinical diagnosis of aplastic anemia, bone marrow examination was carried out for evaluation of pancytopenia. Bone marrow aspirate was diluted and was not contributory, however, bone marrow biopsy showed hypocellular marrow with atypical lymphoid infiltrate with the characteristic ‘fried egg’ appearance with increased reticulin fibres showing pericellular fibrosis (Figs. 1, 2). A careful reevaluation of bone marrow aspirate smears revealed few lymphoid cells with hairy projections. Subsequently Immunohistochemistry (IHC) for Annexin A1 and DBA 44 was carried out which showed positivity in this atypical lymphoid cells infiltrate confirming the diagnosis of HCL. Repeat bone marrow aspirate for IPT also confirmed the diagnosis of HCL with positivity for CD 19, CD 11c, CD 25 and CD 103. The patient subsequently received standard dose chemotherapy with cladribine (@ 0.1 mg/kg/day × 7 days) as continuous infusion and achieved hematological remission later. Presently the patient is in remission for the past eight months.
Fig. 1.
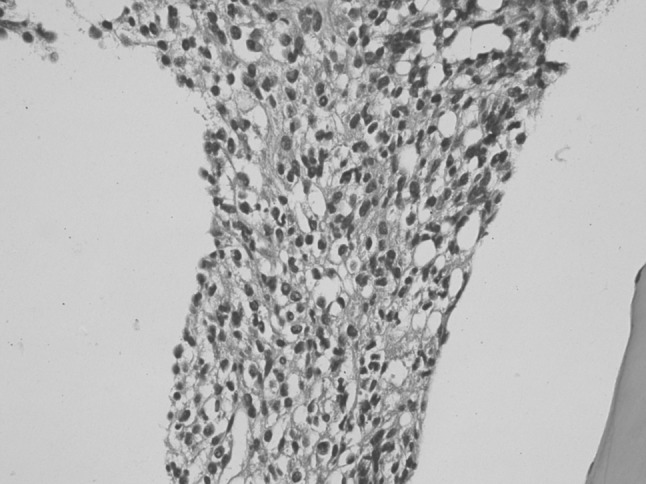
Bone marrow biopsy showing ‘fried egg’ appearance of leukemic cells with halo around the cells. (H&E stain, ×400)
Fig. 2.
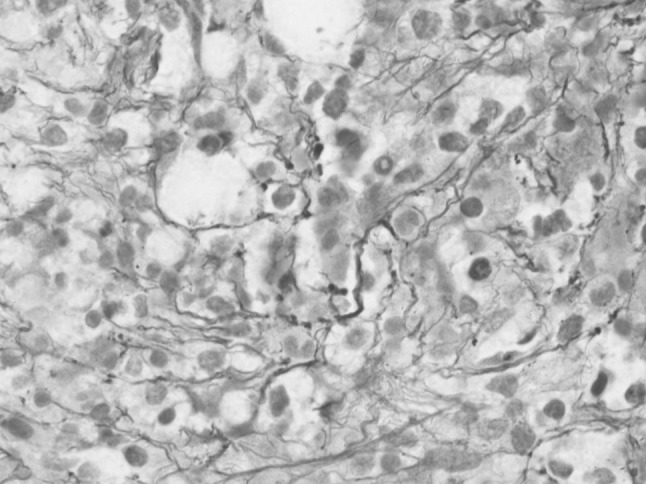
Bone marrow biopsy showing pericellular fibrosis around the leukemic hairy cells. (Reticulin stain, ×1,000)
Case 2
A 50 years old male presented with three-month history of weakness and fatigability, sweating, fever on and off with significant weight loss. On examination he did not have any lymphadenopathy or hepatosplenomegaly. Hemogram showed bicytopenia with Hb 10.3 gm/dl, TLC 2120/cumm and platelet count of 160,000/cumm. Peripheral smear examination showed atypical lymphoid cells with hairy projections (Fig. 3). With the suspicion of HCL bone marrow aspirate, biopsy, cytochemistry and immunophenotyping was carried out which confirmed the diagnosis of HCL as these cells expressed CD 19, CD 11c, CD 25 and CD 103. Subsequently the patient received chemotherapy with cladribine and achieved hematological remission. Presently the patient is in remission for the past nine months.
Fig. 3.
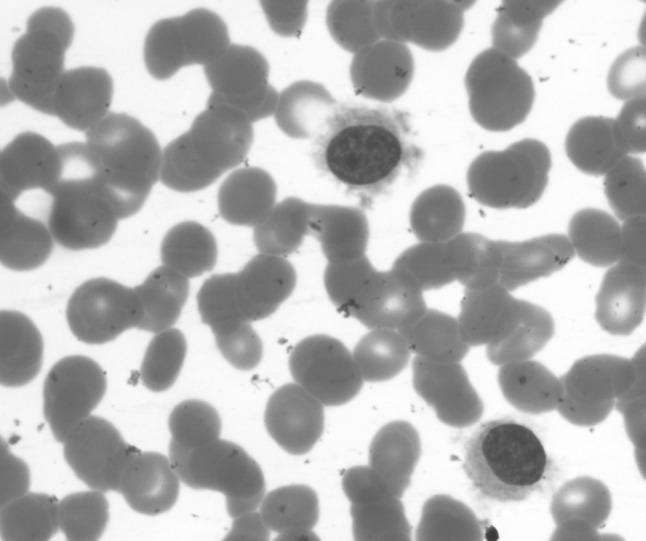
Peripheral blood—hairy cell with round nucleus, homogenous spongy chromatin with abundant pale blue cytoplasm with circumferential hair like projections. (Jenner Giemsa stain, ×1,000). (Color figure online)
Case 3
A 43 years old male patient was referred from pulmonology OPD for work-up of thrombocytopenia. He had two year history of recurrent lower respiratory tract infection. On examination, he had mild hepatomegaly, however, there was no lymphadenopathy or splenomegaly. His hemogram showed Hb of 11.4 gm/dl, TLC 4500/cumm and platelet count of 30,000/cumm. Peripheral smear did not show any hairy cells however the bone marrow aspirate showed few hairy cells which were TRAP (tartarate resistant acid phosphatase) positive (Fig. 4) and bone marrow biopsy showed the typical features of HCL with pericellular fibrosis on reticulin stain. Since the patient did not have splenomegaly, a repeat bone marrow aspirate was done for immunophenotyping which confirmed the diagnosis of HCL. Chemotherapy could not be initiated to this patient due to his poor general condition and subsequently he was lost to follow up.
Fig. 4.
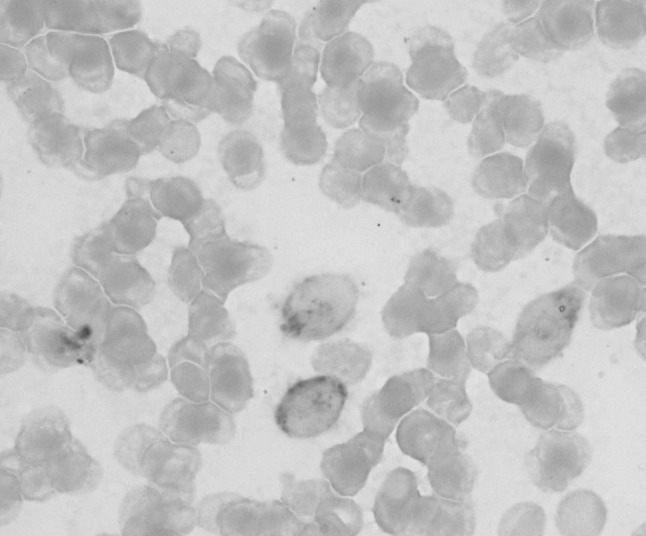
Peripheral blood—TRAP stain of HCL showing bright red granular cytoplasmic positivity in the leukemic cells. (tartrate-treated acid phosphatase stain, ×1,000). (Color figure online)
Case 4
A 67 years old retired doctor underwent coronary angioplasty five months ago and later developed weakness and easy fatigability. Routine hemogram revealed pancytopenia and the patient underwent bone marrow examination at an outside hospital and was suspected to have aplastic anemia in view of a hypocellular bone marrow biopsy. Patient has received multiple packed red cells and platelet transfusions for the past three months. Patient reported to our hematology OPD for second opinion; however he could not produce the previous bone marrow slides for review. With the clinical suspicion of MDS/Aplastic anemia, bone marrow examination was repeated. His hemogram showed Hb of 7.6 gm/dl, TLC 2000/cumm and platelet count of 70,000/cumm. Bone marrow aspirate was diluted and biopsy revealed a patchily cellular bone marrow with focal areas of residual hematopoiesis while some other foci showed monomorphic lymphoid cells infiltrate with ‘fried egg’ appearance and increased pericellular reticulin fibrosis. Careful reexamination of bone marrow aspirate revealed few lymphoid cells with hairy projections which were TRAP positive. With a strong suspicion of HCL even though clinically the diagnosis was not considered, IHC was carried out for Annexin A1 and DBA 44 which were non contributory on two occasions. A month had gone by and in his subsequent visit to OPD, the follow up peripheral smear examination revealed 10 % hairy cells which were immunophenotyped and confirmed as HCL with expression of CD 19, CD 11c, CD 25 and CD 103 as the patient was not willing for another bone marrow examination. The patient was treated with cladribine and is on regular follow up for past two month. His latest hemogram showed hemoglobin of 11.6 gm/dl, TLC 8050/cumm and platelets 1,50,000/cumm. Patient is not transfusion dependant at present.
Discussion
HCL is a unique chronic lymphoproliferative disorder that can mimic or coexist with other clonal hematologic disorders. It can present with pancytopenia or variable cytopenias, associated with splenomegaly and inaspirable bone marrow resulting from fibrosis. Unusual manifestations can be seen. HCL should be entertained as an alternative diagnosis in patients being considered for the diagnosis of aplastic anemia, hypoplastic myelodysplastic syndrome, atypical chronic lymphocytic leukemia, B-Prolymphocytic Leukemia, and idiopathic myelofibrosis [8].
Splenomegaly is by far the most constant physical finding in HCL and HCL is typically included in the differential diagnosis of splenic enlargement. Hence a case of hairy cell leukemia presenting without splenomegaly puts both the clinician and pathologist in diagnostic dilemma many a times, as these cases show only a small percentage of abnormal mononuclear cells in the peripheral blood as well as in the bone marrow aspirate because bone marrow is usually fibrosed in these cases. Hence bone marrow biopsy is the only morphologic tool available for diagnosis of HCL highlighting the high index of suspicion that a morphologist should have in such cases, as HCL cases without splenomegaly most often have a hypocellular bone marrow [9] and these cases may be erroneously diagnosed as aplastic anemia which happened in one of our cases brought out in this series. The incidence of HCL without splenomegaly in various series ranged from 0 to 30 % as brought out in Table 1 and the present series shows the incidence to 40 % even though the sample size is small. In nearly seven percent of HCL cases the bone marrow cellularity is reduced [10] and these patients frequently do not have splenomegaly, suggesting that these patients may have an early disease [11]. Some series report bone marrow hypocellularity to the tune of 18 % [7].
Table 1.
Absence of splenomegaly in cases of hairy cell leukemia: literature review
| Incidence of absence of splenomegaly | ||
|---|---|---|
| Author reference | Number of patients | Absence of splenomegaly in percentage (%) |
| Burke JS et al. 1974 [2] | 21 | 0 |
| Bouroncle et al. 1979 [3] | 82 | 7 |
| Chatterjee et al. 2008 [4] | 15 | 0 |
| Bhargava et al. 2010 [5] | 20 | 15 |
| Galani et al. 2012 [6] | 28 | 4 |
| Gaman AM et al. 2013 [7] | 39 | 30 |
| Present study | 10 | 40 |
It can be said with reasonable confidence that the incidence of such cases of ‘hypoplastic variant’ of HCL will increase in near future due to more and more bone marrow examination being done nowadays for otherwise asymptomatic patients presenting with unicytopenia/bicytopenia or pancytopenia as regular health check ups are carried out even in developing nations, once again highlighting the awareness and high index of suspicion a pathologist should have to diagnose these cases. It is not necessary to reiterate the fact that early diagnosis of HCL is important to ensure that patients obtain maximum benefit from new therapeutic agents such as purine nucleoside analogues and monoclonal antibodies that have greatly improved the prognosis in this rare disorder as the patients after achieving remission can lead a normal life as against their age and sex matched population with regular follow up where as prior to the development of these treatments the median survival of HCL patients was four years [9].
Hairy cell leukemia can present without splenomegaly and so far there are individual case reports of HCL without splenomegaly [12–18]. This series is a first of its kind in reporting a series of HCL cases without splenomegaly and highlighting the importance of diagnosing this condition even in the absence of one of its classical clinical feature namely splenomegaly. Some of the case reports of HCL without splenomegaly presented with lytic bony lesions [15, 17], however none of the cases brought out in present series had any lytic bone lesions. The comparison provided in Table 1 shows the incidence of absence of splenomegaly in HCL cases. The present series shows 40 % of cases to be without splenomegaly even though the case number is small, this finding may predict the recent trend of this disease and as brought out, this finding may not be infrequent in near future.
Conclusion
The purpose of this case series is to create awareness of this uncommon presentation of HCL and to emphasize that absence of splenomegaly does not exclude the diagnosis of hairy-cell leukemia. Careful attention to morphological detail is important especially while interpreting bone marrow biopsies in such cases for early diagnosis, especially when low percentages of “hairy” cells are present in the peripheral blood and bone marrow. Early diagnosis is important to ensure that patients obtain maximum benefit from the newer therapeutic agents that have greatly improved the prognosis in this rare disorder.
Contributor Information
S. Venkatesan, Email: ltcolsvenkatesan@gmail.com
Abhishek Purohit, Email: purohitabhi80@gmail.com.
Mukul Aggarwal, Email: mukulmamc@gmail.com.
Prabhu Manivannan, Email: drprabhumanivannan@gmail.com.
Seema Tyagi, Email: drseematyagi@hotmail.com.
Manoranjan Mahapatra, Email: mrmahapatra@hotmail.com.
Hara P. Pati, Email: harappati@yahoo.com
Renu Saxena, Email: renusaxena@outlook.com.
References
- 1.Swedlow SH, Campo E, Harris NL, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008. [Google Scholar]
- 2.Burke JS, Byrne G, Appaport H. Hairy cell leukemia (leukemic reticuloendotheliosis). A clinical pathologic study of 21 patients. Cancer. 1974;33:1394–1410. doi: 10.1002/1097-0142(197405)33:5<1399::AID-CNCR2820330526>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 3.Bouroncle B. Leukemic reticuloendotheliosis (hairy cell leukemia) Blood. 1979;53:412–436. [PubMed] [Google Scholar]
- 4.Chatterjee T, Panigrahi I, Mahapatra M, Pati HP, Kumar R, Naithani R, et al. Hairy cell leukemia: clinical, pathological and ultrastructural findings in Asian-Indians. Indian J Cancer. 2008;45:41–44. doi: 10.4103/0019-509X.41768. [DOI] [PubMed] [Google Scholar]
- 5.Bhargava R, Kar R, Mahapatra M, Saxena R. The clinico-hematological profile of hairy cell leukaemia: a single centre experience. Hematology. 2010;15:162–164. doi: 10.1179/102453309X12583347113816. [DOI] [PubMed] [Google Scholar]
- 6.Galani KS, Subramanian PG, Gadage VS, Rahman K, AshokKumar MS, Shinde S, et al. Clinico-pathological profile of Hairy cell leukemia: critical insights gained at a tertiary care cancer hospital. Indian J Pathol Microbiol. 2012;55:61–65. doi: 10.4103/0377-4929.94858. [DOI] [PubMed] [Google Scholar]
- 7.Gaman AM. Hairy cell leukemia–a rare type of leukemia. A retrospective study on 39 patients. Rom J Morphol Embryol. 2013;54(3):575–579. [PubMed] [Google Scholar]
- 8.Wanko SO, et al. Hairy cell leukemia: an elusive but treatable disease. Oncologist. 2006;11:780–789. doi: 10.1634/theoncologist.11-7-780. [DOI] [PubMed] [Google Scholar]
- 9.Johnston JB, Grever MR. Hairy cell leukemia. In: Greer JP, List AF, editors. Wintrobe’s clinical hematology. 13. Philadelphia: Lippincott Williams & Wilkins; 2014. pp. 1929–1950. [Google Scholar]
- 10.Yam LT, Phyliky RL, Li CY. Benign and neoplastic disorders simulating hairy cell leukemia. Semin Oncol. 1984;11:353–361. [PubMed] [Google Scholar]
- 11.Westbrook CA, Golde DW. Clinical problems in hairy cell leukemia: diagnosis and management. Semin Oncol. 1984;11:514–522. [PubMed] [Google Scholar]
- 12.Muta T, Okamura T, Oshima K, Kikuchi M, Niho Y. European-American-type hairy cell leukemia without splenomegaly, treated successfully with deoxycoformycin. Rinsho Ketsueki. 2001;42(5):426–431. [PubMed] [Google Scholar]
- 13.Zoldan MC, Ponzoni M, Ricci D, Camba L, Faravelli A. Hairy cell leukemia without splenomegaly nor myelofibrosis in a patient with gastric adenocarcinoma: early phase of the disease or a variant? Pathologica. 1995;87(1):97–99. [PubMed] [Google Scholar]
- 14.Josephine FP, Nissapatorn V. Hairy-cell leukemia: a rare blood disorder in Asia. Southeast Asian J Trop Med Public Health. 2006;37(Suppl 3):190–194. [PubMed] [Google Scholar]
- 15.Gray MT, et al. Hairy-cell leukemia presenting as lytic bone lesions. J Clin Oncol. 2013;31(25):e410–e412. doi: 10.1200/JCO.2012.47.5301. [DOI] [PubMed] [Google Scholar]
- 16.Mirrakhimov AE, Ali AM, Barbaryan A, et al. Pancytopenia in a 70-year-old african-american male: an unusual presentation of a rare disease. Case Rep Hematol. 2014 doi: 10.1155/2014/354810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Spedini P, Tajana M, Bergonzi C. Unusual presentation of hairy cell leukemia. Haematologica. 2000;85(5):548. [PubMed] [Google Scholar]
- 18.Karmali R, Farhat M, Leslie W, McIntire MG, Gregory S. Localized bone disease as a presentation of hairy cell leukemia. Clin Adv Hematol Oncol. 2008;6(4):290–294. [PubMed] [Google Scholar]