

Abstract
Autoimmune hemolysis is rare in multiple myeloma. We describe a rare case of multiple myeloma who presented with autoimmune hemolytic anemia at initial presentation.
Introduction
Multiple myeloma is a common hematological malignancy affecting commonly the older age group. Anemia commonly occurs in a patient with multiple myeloma. However, autoimmune hemolysis is an extremely rare cause of anemia in patients with multiple myeloma. We present a patient with multiple myeloma who had autoimmune hemolytic anemia at initial presentation.
Case Report
A 57-year-old Caucasian female presented with severe fatigue and tiredness. Physical examination revealed pale conjunctiva. Systemic examination was normal. Blood work showed hemoglobin of 7.5 g/dL, hematocrit 25 %, RBC 3.22 million/μL, WBC 3,900/μL, platelet count 331,000/μL, reticulocyte count of 3 %. Her LDH was 312 IU/L and haptoglobin level was undetectable. Direct Coomb’s test was positive for autoantibody. The autoantibody eluted was a warm IgG antibody. Similarly, serum protein electrophoresis and immunofixation showed monoclonal IgG kappa protein 5.15 g/dL. Serum immunoglobulins level were IgG 5,090 mg/dL, IgA 8 mg/dL, IgM 33 mg/dL. Bone marrow biopsy showed a cluster of plasma cells on hematoxylin and eosin stain (Fig. 1). The plasma cells were positive for CD 138 (Fig. 2). Although skeletal survey was negative for osteolytic lesions, she had diffuse osteoporosis.
Fig. 1.
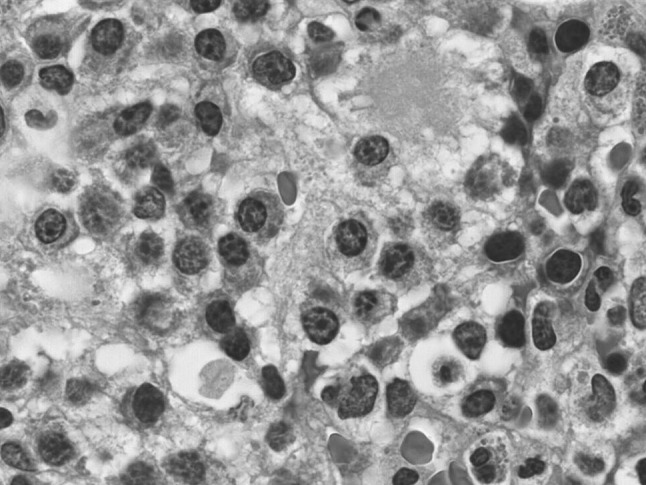
Hematoxylin and eosin stain of bone marrow biopsy showing a cluster of plasma cells
Fig. 2.
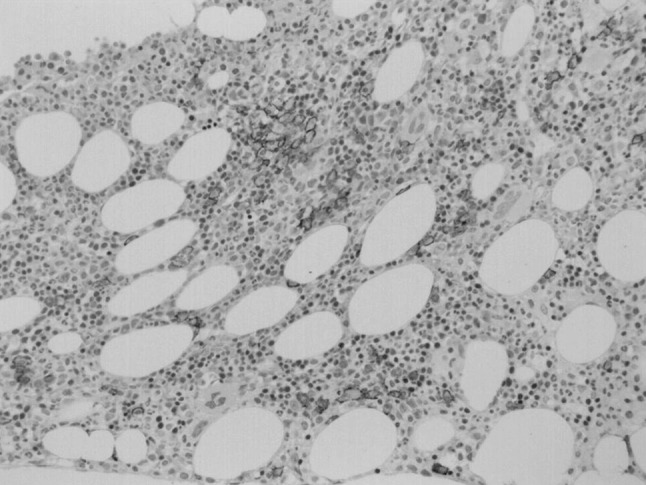
CD 138 stain positive plasma cells
Patient was treated with two units of packed red blood cells and prednisone for her autoimmune hemolytic anemia and, with bortezomib, dexamethasone and zoledronic acid for her multiple myeloma. She showed good hematological response with improvement in hemolysis. Prednisone was discontinued in 10 weeks. She continues to receive her anti-myeloma treatment.
Discussion
Multiple myeloma is a common hematologic cancer. The most common complications of multiple myeloma include anemia, hypercalcemia, pathologic fractures, renal failure and recurrent infections. More than two third of the patients with multiple myeloma have anemia [1]. One study suggested that the up-regulation of apoptogenic receptors by highly malignant myeloma cells results in the destruction of erythroid matrix resulting in normocytic normochromic anemia [2]. Other causes of anemia in multiple myeloma include anemia of chronic disease, relative erythropoietin deficiency (partly due to renal impairment) and myelosuppressive effects of chemoregimen.
Autoimmunity is a common manifestation in other hematological malignancies most importantly with chronic lymphocytic leukemia and non-Hodgkin lymphomas. Autoimmune hemolytic anemia is rare in multiple myeloma. On pubmed/medline search, we found four cases of multiple myeloma with autoimmune hemolytic anemia reported in English literature [3–6]. It is unclear whether AIHA is a result of multiple myeloma or it is just a coincidence. Yi Y et al. [6] reported IgG mediated AIHA in a patient IgA kappa multiple myeloma. AIHA was independent of multiple myeloma.
In conclusion, AIHA as presenting feature of MM is extremely rare. Although rare, autoimmunity should always be kept in mind in patient with multiple myeloma and anemia since it responds well to steroids along with the usual anti-myeloma drugs.
References
- 1.van Rhee F, Anaissie E, Angtuaco E, Bartel T, Epstein J, Nair B, Shaughnessy J, Yaccoby S, Barlogie B (2010).Chapter 109. Myeloma. In Prchal JT, Kaushansky K, Lichtman MA, Kipps TJ, Seligsohn U (eds), Williams Hematology, 8e. http://www.accessmedicine.com.proxy.heal-wa.org/content.aspx?aID=6230001. Accessed 2 January 2013
- 2.Silvestris F, Cafforio P, Tucci M, Dammacco F. Negative regulation of erythroblast maturation by Fas-L(+)/TRAIL(+) highly malignant plasma cells: a major pathogenetic mechanism of anemia in multiple myeloma. Blood. 2002;99(4):1305–1313. doi: 10.1182/blood.V99.4.1305. [DOI] [PubMed] [Google Scholar]
- 3.Wada H, Yata K, Mikami M, Suemori S, Nakanishi H, Kondo T, Tsujioka T, Suetsugu Y, Otsuki T, Sadahira Y, Yawata Y, Sugihara T. Multiple myeloma complicated by autoimmune hemolytic anemia. Intern Med. 2004;43(7):595–598. doi: 10.2169/internalmedicine.43.595. [DOI] [PubMed] [Google Scholar]
- 4.Vaiopoulos G, Kyriakou D, Papadaki H, Fessas P, Eliopoulos GD. Multiple myeloma associated with autoimmune hemolytic anemia. Haematologica. 1994;79(3):262–264. [PubMed] [Google Scholar]
- 5.Friedland M, Schaefer P. Myelomatosis and hemolytic anemia. Hemolytic anemia, a rare complication of multiple myeloma, is successfully managed by splenectomy. R I Med J. 1979;62(12):469–471. [PubMed] [Google Scholar]
- 6.Yi Y, Zhang GS, Gong FJ, Yang JJ. Multiple myeloma complicated by Evans syndrome. Intern Med J. 2009;39(6):421–422. doi: 10.1111/j.1445-5994.2009.01948.x. [DOI] [PubMed] [Google Scholar]