

69-year-old woman presented to the emergency department with palpitations and dizziness of half an hour duration. The patient's history included dyslipidemia under atorvastatin. The patient was hemodynamically stable. The 12-lead surface electrocardiogram demonstrated sustained ventricular tachycardia (VT) with a left ventricular origin and north-west axis at 200 beats/min (Fig. 1A). Cardioversion with intravenous procainamide administration revealed sinus rhythm with left-axis deviation and deep T-wave inversion in the anterior leads (Fig. 1B). Two-dimensional (Fig. 1D and E), contrast (Fig. 1F), and 3-dimensional (Fig. 1G and H) echocardiography revealed mid-ventricular hypertrophy with an apical aneurysm, and an intraventricular flow velocity of 4 m/s (Fig. 1I). Coronary arteriography demonstrated normal coronary arteries, while left ventriculography (Fig. 1C) revealed mid-ventricular obliteration with an abrupt drop in intraventricular pressure from 280 mmHg to 160 mmHg, measured with the pig-tail catheter.
Fig. 1.
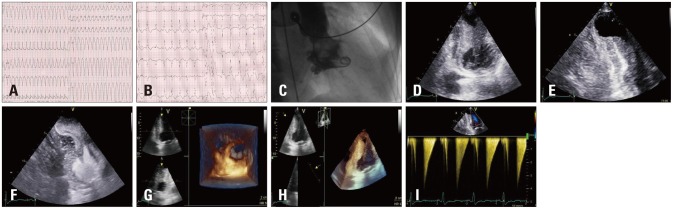
A: Presenting electrocardiogram showing ventricular tachycardia at 200 beats/min. B: Electrocardiogram revealing sinus rhythm with deep T-wave inversion in the anterior leads after intravenous procainamide administration. C: Left ventriculography demonstrating mid-ventricular obliteration. D and E: Two-dimensional echocardiography. F: Contrast echocardiography. G and H: Three-dimensional echocardiography, showing left mid-ventricular hypertrophy with an apical aneurysm. I: Intraventricular flow velocity of 4 m/s.
Mid-ventricular obstructive hypertrophy cardiomyopathy comprises a rare subtype of hypertrophic cardiomyopathies (HCM), accounting for only 1% of cases.1) It is characterized by the presence of a pressure gradient between the apical and basal chambers of the left ventricle (LV). The mid-cavity obstruction is the result of the mid-systolic muscular apposition of the septum and LV free wall producing distinct proximal and distal chambers, resembling an "hourglass" shape.2) Furthermore, LV apical aneurysms are present in up to 2% of patients with HCM, and are associated with intramural thrombus and sustained monomorphic VT.3),4)
Our patient received an implantable cardioverter-defibrillator and was discharged with explicit instructions and medication. This case demonstrates multiple complications and peculiarities of HCM.
References
- 1.Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308–1320. doi: 10.1001/jama.287.10.1308. [DOI] [PubMed] [Google Scholar]
- 2.Efthimiadis GK, Pliakos C, Pagourelias ED, Parcharidou DG, Spanos G, Paraskevaidis S, Styliadis IH, Parcharidis G. Hypertrophic cardiomyopathy with midventricular obstruction and apical aneurysm formation in a single family: case report. Cardiovasc Ultrasound. 2009;7:26. doi: 10.1186/1476-7120-7-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ. Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy. Circulation. 2008;118:1541–1549. doi: 10.1161/CIRCULATIONAHA.108.781401. [DOI] [PubMed] [Google Scholar]
- 4.Holloway CJ, Betts TR, Neubauer S, Myerson SG. Hypertrophic cardiomyopathy complicated by large apical aneurysm and thrombus, presenting as ventricular tachycardia. J Am Coll Cardiol. 2010;56:1961. doi: 10.1016/j.jacc.2010.01.078. [DOI] [PubMed] [Google Scholar]