

Abstract
Hemiballism-hemichorea (HB-HC) is a hyperkinetic disorder characterized by continuous involuntary movements of the extremities. It could be associated with non-insulin dependent diabetes mellitus. A very few cases of bilateral HB-HC have been reported until today. We describe here the case of a Taiwanese woman (85 years old) presenting with bilateral HB-HC and diabetes mellitus.
Key words: hemiballism-hemichorea, diabetes mellitus, Taiwan
Introduction
Hemiballism-hemichorea (HB-HC) is characterized by the continuous and involuntary movements of both the distal and proximal part of the extremities.1,2 Most of cases are associated with diabetes mellitus with poor control and presented in the elderly women.2-5 Typical brain magnetic resonance imaging (MRI) presentation shows unilateral hyper-intensity signal over the striatum region, contra-lateral to the symptom side. Nonetheless, bilateral HB-HC is seldom reported. Here, we report a case of bilateral HB-HC associated with diabetes mellitus. Brain MRI are also carefully evaluated.
Case Report
A 85-year-old Taiwanese woman with poor controlled non-insulin dependent diabetes mellitus (NIDDM) noted four limbs involuntary movements one week prior to medical attention. She was consciousness, clear and oriented to person, place and time. A neurological consultation was made and it revealed she had bilateral HB-HC (first with left sided extremities, which was then ensued with right sided extremities). After admission, contrasted cerebral MRI was performed; it showed the evidence of T1 weighted imaging with hyperintensity signal in bilateral putamen regions (Figure 1). The routine laboratory work-up showed that her fasting blood sugar was up to 500 mg/dL and hemoglobin A1C was 16.2%. During the two-week hospitalization, hyperglycemia was corrected with aggressive insulin therapy. In addition, she was treated with haloperidol 1 mg twice a day. Her bilateral HB-HC was greatly subsided. After she discharged from the ward, her bilateral HB-HC remained silent. The second MRI was taken four months after her initial involuntary episode and showed complete resolution of the previously-reported brain lesions.
Figure 1.
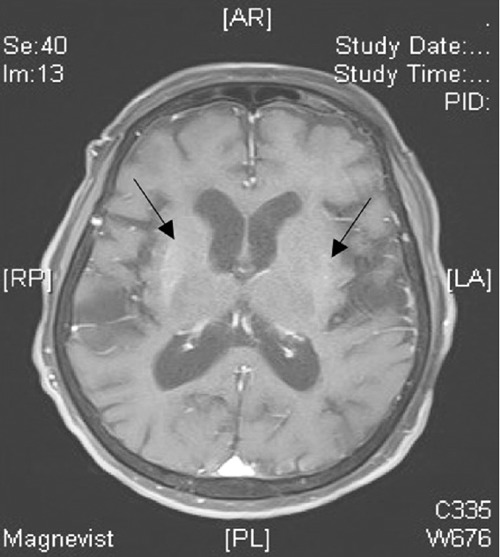
Gadolinium-enhanced brain magnetic resonance imaging shows hyper-intensity signal over bilateral putamen regions in T1 weighted imaging.
Discussion and Conclusions
We report the case of a patient with initial HBHC over the left side extremities. The right sided extremities ensued the same phenomena three days later. The symmetrical focal abnormalities over bilateral striatum of her brain MRI taken during the hospitalization correspond to her clinical manifestations.
The clinical symptom could be alleviated with intensive correction of hyperglycemia state and administration of low doses of haloperidol.1,4 The follow-up brain MRI, which showed intact cerebral parenchyma, also echoes the satisfactory treatment. On literature review, the likely etiologies of HB-HC cases vary. However, most of reported cases are associated with poor controlled type 2 diabetes mellitus in either hypoglycemic or hyperglycemic state as the initial manifestation.6,7 The other etiologies are ischemic change contra-lateral to the lesion side, infection,1,4,5 or tumor metastasis.3 It is speculated by some scholars inflammation process plays a pivotal role in this malady owing to increased level of IgG in cerebrospinal fluid examination.2 However, the definite cause of HB-HC is still uncertain and required advanced studies.
In addition, most of the involuntary movement occurs unilaterally. Few cases have been documented with bilateral HB-HC, and whose efficacy of treatment and neuro-imaging studies are compatible with one another.
References
- 1.Mugundhan K, Maski A, Elanchezhian JA, et al. Mixed movement disorder as the presenting manifestation of non-ketotic hyperglycemia. J Assoc Physicians India 2010;58: 387-8 [PubMed] [Google Scholar]
- 2.Wang JH, Wu T, Deng BQ, et al. Hemichoreahemiballismus associated with nonketotic hyperglycemia: a possible role of inflammation. J Neurol Sci 2009;284:198-202 [DOI] [PubMed] [Google Scholar]
- 3.Moore FG.Bilateral hemichorea-hemiballism caused by metastatic lung cancer. Mov Disord 2009;24:1405-6 [DOI] [PubMed] [Google Scholar]
- 4.Ohmori H, Hirashima K, Ishihara D, et al. Two cases of hemiballism-hemichorea with T1-weighted MR image hyperintensities. Intern Med 2005;44:1280-5 [DOI] [PubMed] [Google Scholar]
- 5.Oh SH, Lee KY, Im JH, Lee MS.Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci 2002;200:57-62 [DOI] [PubMed] [Google Scholar]
- 6.Guerrero WR, Okun MS, McFarland NR.Encephalopathy, hypoglycemia, and flailing extremities: a case of bilateral chorea-ballism associated with diabetic ketoacidosis. Tremor Other Hyperkinet Mov (N Y) 2012;2:pii:tre-02-58-235-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ogawa K, Suzuki Y, Kamei S, Mizutani T.Choreic involuntary movement that occurred during therapy for diabetes mellitus. Nihon Ronen Igakkai Zasshi 2008;45:225-30 [Article in Japanese] [DOI] [PubMed] [Google Scholar]