

Abstract
Background
Neonatal septicaemia diagnosis based on clinical features alone is non-specific leading to the initiation of unnecessary antibiotic treatment posing a danger of increased antibiotic resistance. In the present study the utility of serial qualitative C-reactive protein (CRP) assay and white blood cells count (WBC) in the diagnosis of neonatal septicaemia was investigated using blood culture as gold standard.
Methods
A total of 305 neonates admitted at Bugando Medical Centre (BMC) neonatal units between September 2013 and April 2014 were enrolled. Demographic and clinical data were collected using standardized data collection tool. Blood specimens were collected for blood culture, WBC count and qualitative CRP assay.
Results
Of 305 neonates; 224 (73.4%) were ≤ 72 hrs of age and 91(29.8%) had low birth weight. The positive CRP assay was observed in 67 (22.0%), 80 (26.2%) and 88 (28.9%) of neonates on day 1, 2 and 3 respectively; with any CRP positive occurred in 104 (34.1%) of neonates. The sensitivities of CRP assay in the diagnosis of septicaemia using culture as gold standard on day 1, 2, 3 and any positive were 40.4%, 53.2%, 54.8% and 62.9% respectively. While specificities were 82.7%, 80.7%, 77.8% and 73.3% respectively. Higher sensitivity of 75% was observed when CRP was used to diagnose gram negative septicaemia compared to 50% that was observed in the diagnosis of gram positive septicaemia. WBC count of ≥13 × 109 /L had sensitivity and specificity of 64.5% and 66.7% respectively with area under the curve of 0.694. When the any positive CRP and WBC of ≥13 × 109 /L were used the sensitivity increased to 90.3% with specificity of 50%. Neonates with septicaemia due to gram negative bacteria were significantly found to have higher rates of positive CRP than neonates with gram positive septicaemia and with negative culture (p < 0.001, OR 8.2, 95 CI; 2.9-26).
Conclusion
In place where blood culture is limited neonates having clinical features of neonatal sepsis with positive qualitative CRP assay and increased WBC should urgently be initiated on appropriate sepsis management in order to reduce morbidity and mortality associated with neonatal sepsis.
Keywords: C-reactive protein, Neonatal sepsis, WBC
Background
Neonatal deaths account for about 40% of all deaths among underfives. Out of all neonatal deaths in developing countries, 50% occur during the first 24 hours of life and 75% during the first week of life [1]. Globally, deaths occurring in the first month of life have increased from 36% in 1990 to 43% in 2011. Most of deaths have been due to neonatal septicaemia and prematurity [2]. In 2010 at the Bugando medical center (BMC) prevalence of neonatal septicaemia was 39% with mortality rate of 19% [3]. Delayed diagnosis and inappropriate treatment of neonatal septicaemia has been associated with neurological complication with increased mortality [4].
Though blood culture is the gold standard in the diagnosis of neonatal septicaemia, it takes more than 3 days for the final results to be available and the technique is not available in many settings in developing countries [5]. This necessitates the use of antibiotics with no supporting microbiological results; hence leading to unnecessary cost and risk of increased resistance development. In developing countries, there are no suitable clinical or laboratory parameters available to guide the duration of the antibiotic treatment. At BMC and in many other centres in developing countries, full antibiotics courses are prescribed in all neonates suspected with septicaemia regardless of culture results. This practice at BMC does not reduce the mortality due to neonatal septicaemia however it has been found to add to the problem of antibiotic resistance, as evidenced by the fact that all Klebsiella pneumoniae isolated in the neonatal unit were resistant to gentamicin and being more than 50% resistant to third generation cephalosporin [6].
Early diagnosis followed by appropriate treatment of all newborns with clinical suspicion of septicaemia has been found to be an important strategy in preventing life threatening complications [7]. Most of the time, initial diagnosis of neonatal septicaemia is based on clinical features which are non-specific; resulting in initiation of unnecessary empirical antibiotic treatment posing to a danger of increased antibiotic resistance [8].
Therefore; in order to guide the empiric antibiotic treatment it is important to evaluate cheap and inexpensive CRP assay as a rapid test to justify the use and duration of antibiotics treatment in many settings in developing countries. C-reactive protein is an acute-phase reactant protein synthesized by the liver within six hours after the onset of infectious process [9, 10]. There is variation in the performance of CRP in the diagnosis of septicaemia depending on the etiology of septicaemia and the setting. Therefore this study aimed at evaluating the use of serial qualitative CRP assay as a rapid test to accurately predict neonatal septicaemia so as to avoid unnecessary use of antibiotics and to guide the duration of antibiotic therapy.
Methods
Study design and study area
This was a hospital based analytical cross sectional study conducted from October 2013 to April 2014. This study was conducted at BMC, Mwanza, Tanzania which is a tertiary teaching hospital serving about 14 million population.
Inclusion criteria and exclusion criteria
All neonates with clinical suspicion of neonatal sepsis according to WHO criteria [11] admitted at NICU and premature Unit were enrolled. Neonates with history of use of antibiotics before enrolment for more than 72 hours and those with body weight less than 1 kilogram were excluded from the study.
Sample size and sampling procedure
Sample size was estimated using Buderer formula [12]; using anticipated sensitivity and specificity of 95% and neonatal sepsis prevalence of 40% [3]. The minimum sample size obtained was 305 neonates. All neonates admitted to the neonatal wards with clinical sepsis were recruited serially into the study until the sample size was reached. Using WHO guidelines for sepsis in young infants a standard structured data collection tool was designed and used to obtain social demographic data and other relevant factors related to neonatal septicaemia like maternal fever, premature rupture of membrane (PROM), mode of delivery, birth weight of the baby, gestational age (less than 37 completed weeks was considered as premature), temperature of the infant, respiratory rate, cyanosis, jaundice, umbilical redness, convulsion, decreased movement and ability to breast feed.
Laboratory procedures
C - reactive protein assay
C-reactive protein was tested qualitatively using Immunopak (RECKON DIAGNOSTICS, INDIA). About 0.3 ml or 0.5 ml of venous blood was collected at 24 hours, 48 hours and 72 hours after admission using plain bottles (BD Vacutainer, Nairobi, Kenya). Assays were done following manufacturer instructions; presence of agglutination similar to positive control was considered as positive CRP assay indicating CRP level of more than 6 mg/dl.
Blood culture
Blood culture was performed using Brain Heart Infusion broth (BHI) (Oxoid Ltd) in a ratio of blood to BHI of 1:10 as previously described [3]. Subsequent sub-culture was done on day 1, 3 and 7 on 5% sheep blood agar, chocolate agar and MacConkey agar (Oxoid, UK). Identification of bacteria was performed using conventional physiological and biochemical methods [13, 14]. Repeat blood culture was ordered in all cases where Coagulase negative staphylococcus (CNS) was isolated. Re-isolation of CNS was considered significant blood culture result. Antimicrobial susceptibility of isolates was determined using disk diffusion method according to the Clinical Laboratory standard Institute (CLSI) [15].
Complete blood count
About 2 ml of blood in EDTA container (BD Vacutainer, Nairobi, Kenya) was collected for WBC count and platelet count and estimated using hematological analyzer (Beckman coulter (UK) LTD). WBC count of less than 9 × 109/l or more than 30 × 109/l were considered as leucopenia and leukocytosis respectively [16].
Data analysis
Data were double entered into Microsoft excel and analyzed using STATA version 11. Results were summarized using proportions (%) for categorical data and means (SD) or medians (IQR) for continuous variables. Categorical variables were compared using either Pearson’s Chi–squared or Fisher’s exact test where appropriate. The continuous variables were compared using student t-test and Wilcoxon sign rank test for parametric and non-parametric variables respectively. To determine the sensitivity and specificity of the CRP in the diagnosing neonatal septicaemia we used 2-by-2 contingency tables. We used Receiver operating characteristic (ROC) to determine the performance WBC in the diagnosis of neonatal septicemia. While, to determine predictors of positive CRP, univariate followed by multivariate logistic regressions analysis were performed. Predictors investigated included; socio-demographic factors, clinical features and laboratory parameters. Odds ratios with respective 95% confidence interval (CI) were reported. Predictors with a p-value of less than 0.05 were considered statistically significant.
Quality control
Data from questionnaires were entered into a data sheet. The reading of CRP test was done by two qualified laboratory technologists to avoid bias. All microbiological testing were controlled using quality control strains; Escherichia coli ATCC 25922, Klebsiella pneumoniae ATCC 13883 and Staphylococcus aureus ATCC 25923.
Ethical considerations
The proposal of this study was presented to the CUHAS-Bugando/BMC department of Pediatric and Child Health for approval and then to CUHAS-Bugando ethics committee for clearance. Written Informed consent for the participation in the study was obtained from mother/caretaker of the respective neonate.
Results
Baseline characteristics of patient enrolled in the study
During the study period a total of 624 neonates were admitted at NICU and premature neonatal unit. Out of 310 neonates with clinical suspicion of sepsis, 305 (98%) were enrolled in the study from September 2013 to April 2014. Of 305 neonates, 224(73.4%) were ≤72 hours of age (Table 1). Median age was 1 day with IQR of 1–4 days. Among 305 neonates; 149(48.9%) were male and 156(51.2%) were female. A total of 69 (22.6%) neonates were premature. Regarding place of delivery, 30(9.8%) of neonates were delivered at home (Table 1). Thirty one (10.2%) of the neonates had history of convulsions, 59(19.3%) had jaundice, 186(61%) had body temperature of more than 37.5°C and 133(43.6%) had oxygen saturation of less than 90%.
Table 1.
Distribution of demographic characteristics of neonates with sepsis
| Child’s characteristic | Number | Percent (%) |
|---|---|---|
| Sex | ||
| Female | 149 | 48.9 |
| Male | 156 | 51.2 |
| Age | ||
| ≤ 72 hours | 224 | 73.4 |
| > 72 hours | 81 | 26.6 |
| Mode of delivery | ||
| Caesarean section | 67 | 22 |
| Spontaneous vertex delivery | 238 | 78 |
| Birth weight | ||
| Very low birth weight | 18 | 5.9 |
| Low birth weight | 73 | 23.9 |
| Normal birth weight | 214 | 70.2 |
| Gestation age | ||
| Premature | 69 | 22.6 |
| Full term | 236 | 77.4 |
| Hospital delivery | ||
| Yes | 275 | 90.2 |
| No | 30 | 9.8 |
| Convulsion | ||
| Yes | 31 | 10.2 |
| No | 274 | 89.8 |
| Jaundice | ||
| Yes | 59 | 19.3 |
| NO | 249 | 80.7 |
| Poor feeding | ||
| Yes | 182 | 59 |
| No | 123 | 40.3 |
| Oxygen saturation | ||
| <90% | 133 | 43.6 |
| >90% | 172 | 56.4 |
| Body temperature | ||
| Hypothermia | 96 | 31.5 |
| Normal | 23 | 7.5 |
| Hyperthermia | 186 | 61.0 |
C-reactive protein and blood culture results
Out of 305 neonates; 104(34.1%) had any positive CRP; the positive CRP on day 1, 2 and 3 were 67(22%) 80(26.2%) and 88(28.9%) respectively. Positive aerobic blood culture was detected in 62(20.3%) of neonates (Table 2). All specimens with positive culture were detected within 48 hrs of incubation.
Table 2.
Sensitivity, Specificity, Positive and negative predictive values
| Parameters | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| Any CRP + ve | 62.9% (49.7-74.8) | 73.3% (67.2-78.7) | 37.5% (28.2-47.5) | 88.6% (83.3-92.6) |
| CRP day 1 | 40.3% (28.1-53.6) | 82.7% (77.4-87.3) | 37.5% (25.8-50.0) | 84.5% (79.2-88.8) |
| CRP day 2 | 53.2% (40.1-66.0) | 80.7% (75.1-85.4) | 41.3% (30.4-52.8) | 87.1% (82.0-91.2) |
| CRP day 3 | 54.8% (41.7-67.5) | 77.8% (72.0-82.8) | 38.6% (28.4-49.6) | 87.1% (81.9-91.3) |
| WBC | 64.5% (51.3-76.3) | 66.7% (60.4-72.6) | 33.1 (24.8-42.2) | 88.4 (82.5-92.4) |
| Any CRP + WBC | 90.3% (80.1-96.4) | 50.2% (43.7-56.7) | 31.6% (24.9-39.0) | 95.3% (90.1-98.3) |
| CRP gram negative sepsis | 75.0% (53.3-90.2) | 73.3% (67.8-78.7) | 21.7% (13.4-32.1) | 96.7% (93.0-98.8) |
| CRP gram positive sepsis | 55.3% (38.3-71.4) | 73.2% (67.2-78.7) | 24.4% (15.8-34.9) | 91.3% (86.4-94.8) |
Sensitivity, specificity, PPV and NPV of qualitative CRP assay and WBC
The sensitivity of CRP was found to be 40.4%, 53.2% and 54.8% on day 1, 2 and 3 with specificity of 82.7%, 80.7% and 77.8% respectively. While the positive predictive value was found to be 37.5%, 41.3% and 38.6% with negative predictive value of 84.5%, 87.1%, and 88.6% on day 1, 2 and 3 respectively. Any positive CRP had sensitivity of 62.9% with specificity of 73.3% (Table 2). Higher sensitivity was obtained when CRP was used to diagnose gram negative septicaemia than in the diagnosis of gram positive septicaemia (75% vs. 50%) with the same specificity. Using WBC cut off point of ≥13 × 109 /L the sensitivity obtained was of 64.5% with specificity of 66.7% and area under the curve of 0.6924 (Figure 1). When any positive CRP was combined with raised WBC of ≥13 × 109 /L the sensitivity and specificity obtained were 90.3% and 50.2% respectively (Table 2).
Figure 1.
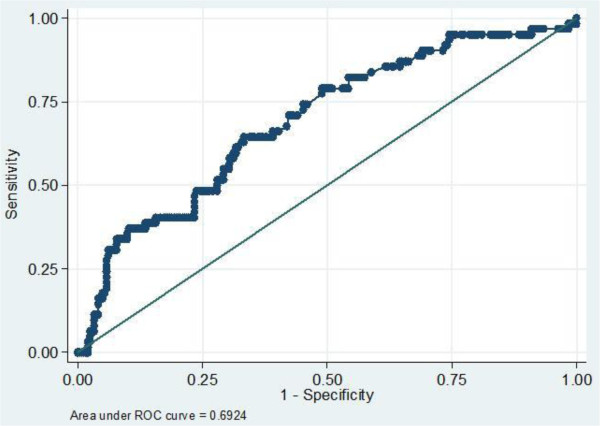
Receiver operating characteristic (ROC) of WBC and blood culture showing the performance WBC in the diagnosis of neonatal septicemia. Cut off points of WBC ≥ 13* 109 /L has sensitivity of 64.5% and specificity 66.7%.
C-reactive protein, WBC and neonatal sepsis
Higher rates of CRP positive were observed among neonates with confirmed neonatal sepsis than those with negative culture (p <0.05) Figure 2. Neonates with gram negative sepsis had significantly higher rates of positive CRP than neonates with gram positive neonatal sepsis and neonates with negative blood culture. Significantly higher means of WBC were observed among neonates with positive blood culture and those with positive CRP when compared to neonates with negative culture and negative CRP. Means WBC among neonates with gram negative septicaemia and gram positive septicaemia were 20431.25c/mm3 and 20525.26 c/mm3 respectively compared to the mean of 13915.72/mm3 among children with negative blood culture (Table 3).
Figure 2.
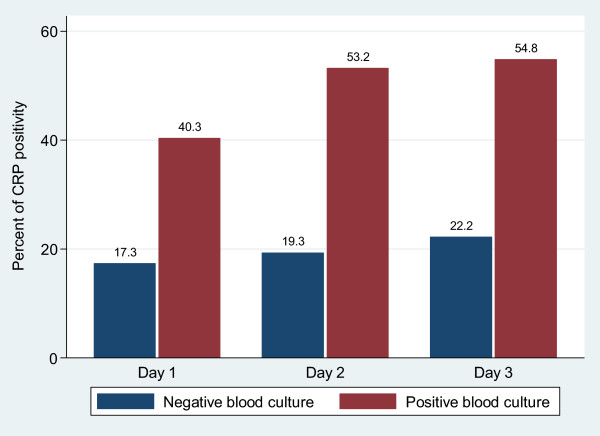
Bar charts showing the rates of positive CRP among culture positive and culture negative neonates on day 1, 2 and 3.
Table 3.
CRP, Neonatal sepsis and WBC in relation to gram reactions
| CRP | % CRP positive | OR | 95% CI | P value |
|---|---|---|---|---|
| CRP1 | ||||
| Negative culture (243) | 42 (17.3%) | 1 | ||
| Gram positive sepsis (38) | 12 (31.5%) | 2.2 | 0.93-4.9 | 0.0375 |
| Gram negative sepsis (24) | 13 (54.4%) | 5.6 | 2.1-14.87 | <0.0001 |
| CRP2 | ||||
| Negative culture (243) | 47 (19.3%) | 1 | ||
| Gram positive sepsis (38) | 17 (44.7%) | 3.4 | 1.5-7.2 | 0.0005 |
| Gram negative sepsis (24) | 16 (66.7%) | 8.3 | 3.1-23.67 | <0.0001 |
| CRP3 | ||||
| Negative culture (243) | 54 (22.2%) | 1 | ||
| Gram positive sepsis (38) | 17 (44.7%) | 2.8 | 1.2-6.0 | 0.003 |
| Gram negative sepsis (24) | 17 (70.0%) | 8.5 | 3.1-25.3 | <0.0001 |
| Any positive | ||||
| Negative culture (243) | 65 (26.7%) | 1 | ||
| Gram positive sepsis (38) | 21 (55.2%) | 3.3 | 1.5-7.2 | 0.0004 |
| Gram negative sepsis (24) | 18 (75.0%) | 8.2 | 2.9-26.2 | <0.0001 |
| Parameter | N | Mean WBC c/mm 3 | P value | |
| Negative culture | 243 | 13915.72 ± 11707.4 | ||
| Gram positive sepsis | 38 | 20525.26 ± 11800.8 | 0.0007 | |
| Gram negative sepsis | 24 | 20431.25 ± 14107.8 | 0.0056 | |
| CRP positive | ||||
| CRP1 | ||||
| Positive | 67 | 18025.1 ± 15964.6 | ||
| Negative | 238 | 14471.2 ± 10782.2 | 0.0173 | |
| CRP2 | ||||
| Positive | 80 | 16785.6 ± 13529.9 | ||
| Negative | 225 | 14706.6 ± 11633.8 | 0.0950 | |
| CRP3 | ||||
| Positive | 88 | 16925.8 ± 12697.2 | ||
| Negative | 217 | 14573.1 ± 11914.3 | 0.0632 | |
| Any CRP positive | ||||
| Positive | 104 | 17301.7 ± 14137.8 | ||
| Negative | 201 | 14191.3 ± 10865.0 | 0.0086 |
Predictors of positive CRP and neonatal septicaemia
On univariate analysis; the predictors of positive CRP were found to be older age (p = 0.03) and higher body temperature (p = 0.02), however on multivariate analysis only poor feeding and raised body temperature remained significantly associated with positive CRP (Table 4). Factors found to predict neonatal septicaemia were positive CRP (p < 0.001, 95% CI; 2.6-8.2), elevated WBC (p < 0.001, 95% CI; 1.03-1.08), high body temperature (p = 0.04, CI 1.01-1.32) and home delivery 95% CI; 2.29(1.05-5.01). Of 305 neonates, 22(7.2%) died during the study period. Meconium aspiration (OR 3.3, 95% CI (1.1-10.5), p = 0.038), convulsions (OR 5.4, 95% CI (1.8-16.2), p = 0.003), oxygen desaturation <90% (OR 4.7(CI 1.3-16.8) p = 0.017) and jaundice (OR 7.8(CI 2.3-26.9) p = 0.001 were independent factors found to be associated with death. Neonates with positive CRP had 1.7 times risk of death than those with negative CRP.
Table 4.
Factors associated with positive CRP, neonatal sepsis and death on multivariate logistic regression
| CRP | Neonatal sepsis | Deaths | ||||
|---|---|---|---|---|---|---|
| OR [95% CI] | P value | OR [95% CI] | P value | OR [95% CI] | P value | |
| Age in days | 1.05 (1.00-1.11) | 0.034 | 1.1 (1.0-1.1) | 0.056 | - | - |
| Home delivery | 2.29 (1.05-5.01) | 0.045 | - | - | ||
| Poor feeding | 1.84 (1.1-3.188) | 0.029 | - | - | - | - |
| Body temperature | 1.18 (1.03-1.35) | 0.016 | 1.15 (1.01-132) | 0.038 | - | - |
| WBC | 1.02 (1.00-1.040) | 0.05 | 1.06 (1.03-1.08) | <0.001 | - | - |
| CRP positive | - | - | 4.6 (2.6-8.2) | <0.001 | 1.7 (0.6-4.8) | 0.352 |
| Convulsion | - | - | - | - | 5.49 (1.8-16.2) | 0.003 |
| Meconium liquor | - | - | - | - | 3.3 (1.1-10.5) | 0.038 |
| Jaundice | - | - | - | - | 7.8 (2.3-26.9) | 0.001 |
| O2 saturation < 90% | - | - | - | - | 4.7 (1.3-16.8) | 0.017 |
Discussion
Baseline characteristics
The study involved 305 neonates with suspected neonatal septicaemia attending BMC neonatal units. As in previous studies [3, 17, 18], most of these neonates were below 72 hrs of age and with low birth weight. The low birth weight in the current study is partially contributed to premature delivery because 22.6% of neonates were delivered prematurely of whom 29.5% had low birth weight. In contrast to previous study which observed home delivery in 38% of neonates with suspected neonatal sepsis in the current study only 9.8% of neonates were delivered at home. From 2010 to 2012, we observed a decrease in home delivery of more than 70%; this could be due to ongoing campaigns by NGOs and Ministry of Health Tanzania resulting in awareness of health services and importance of hospital delivery.
Clinical presentation of neonates
Clinical features of neonatal sepsis are usually non-specific and subtle and neonates with suspected sepsis can present with one or more of the following; fever, jaundice, convulsion, lethargy, poor feeding etc. Almost similar rates clinical findings (poor feeding, cyanosis, jaundice, body temperature, lethargy, chest in drawing) were observed in this study as in other studies in Tanzania [3, 18]. This could be explained by the fact that similar inclusion criteria were used to enroll study participants. Compare to previous study in the same setting 4 years ago, low convulsion rate was observed in the present study, this could be due to less birth asphyxia in present study since most neonates were hospital delivery and also there are improvements in NICU care especially in checking random blood glucose to prevent hypoglycemia.
Utility of qualitative CRP assay and WBC count in the diagnosis of neonatal septicaemia
In the present study, the overall sensitivity and specificity of CRP in the diagnosis of neonatal septicaemia were 63% and 73% respectively. Almost similar findings were observed in Nigeria whereby sensitivity and specificity of 74% and 74.1% respectively were observed using semi-quantitative assay [19]. The slightly difference could be explained by the type of the tests used, in Nigeria study they used Lorne CRP latex kit from Great Britain while in the current study the semi-quantitative assay from Reckon Diagnostic, India, Immunopak was used. Low sensitivity and specificity are observed when our results are compared with other studies [10, 20, 21] which used quantitative assays.
There are no established references intervals of CRP in the neonatal period and upper limit have been established only in symptomatic neonates. CRP may rise physiologically after stressful delivery, intraventricular hemorrhage, fetal distress, perinatal asphyxia and meconium aspiration. In these conditions the CRP level usually goes back to normal within 24–48 hours. These conditions contribute to the reduced specificity of the qualitative assay of CRP in the diagnosis of neonatal septicaemia. In these situations, a single normal value is not sufficient to diagnose neonatal septicaemia, therefore to increase specificity serial assays are recommended. In most of the time neonates with persistent high CRP levels are more likely to have neonatal sepsis. In the present study there was an increase in positive rates of CRP among neonates from day 1 to day 3 with majority of neonates who were positive on day 1 remained positive on day 3. These findings suggest that most of our neonates with positive CRP had septicaemia [22]. The discrepancy between CRP and culture results in this study could be explained by the culture technique used. In the present study manual blood culture was used; this technique has been found to contribute to low sensitivity of CRP when compared to automated techniques [23]. However, there has been wide range of CRP sensitivity reported ranging from 47-100% and this is due to different reference values and test methodologies [23]. Using quantitative methods; CRP assays have been shown to have higher sensitivity than qualitative methods. Other factors that could explain low sensitivity in our study is the predominant of gram positive bacteria; neonates with gram positive septicaemia were found to have significantly lower rates of positive CRP than among neonates with gram negative sepsis. Several studies have reported C-reactive protein to be higher in gram negative bacteria than gram positive bacteria neonatal septicaemia [24, 25]. In this study when sub-analysis was done the sensitivity of CRP to diagnose gram negative neonatal septicaemia increased to 75% while for gram positive septicaemia dropped to 50%.
In several previous studies [26–28]; WBC shows little correlation with neonatal septicaemia however in the present study neonates with septicaemia had significantly higher mean of WBC than those with negative culture. The sensitivity of increased WBC of ≥13 × 109/L in the diagnosis of neonatal septicaemia was comparable to previous studies. When the increased WBC was combined with any positive CRP sensitivity of 90.3% was obtained similar to a recent study among preterm babies [29].
Including neonates admitted at Bugando Medical Center with clinical suspicion of neonatal sepsis was major limitation of this study. Other limitations include lack of lumbar puncture due to lack of appropriate instruments and/or supplies. Additionally the blood culture was done using only the aerobic manual system again because of lack of equipment and supplies. Finally, there was no control group due to ethical constraints and difficulty obtaining blood in infants who have no clinical suspicious for septicaemia.
Conclusion
Serial CRP qualitative assays combined with raised WBC has high sensitivity in the diagnosis of neonatal septicaemia. In place where blood culture is limited, neonates with positive qualitative CRP assay and raised WBC together with clinical features such as convulsion, raised body temperature and poor feeding should urgently be initiated on appropriate sepsis management in order to reduce associated morbidity and mortality. Based on these findings CRP and WBC counts can be used as inexpensive methods to diagnose neonatal septicaemia in developing countries in order reduce the duration of antibiotics treatment hence preventing resistance development. Another study using quantitative CRP assay should be considered in our setting in order to estimate the cutoff point of CRP which strongly predicts neonatal septicaemia.
Acknowledgements
We are very gratefully for the parents who allow their neonates to participate in the study. We would like to acknowledge the assistance and guidance provided by all staff members of the Department of Pediatrics, Bugando Medical Center, as well as the Department of Microbiology/Immunology, Catholic University of Health and Allied Sciences, Bugando Hospital. This research was supported by grants from Ministry of Health to FC, reagents from CUHAS to SEM.
Footnotes
Competing interest
The authors declare that they have no competing interests.
Authors’ contributions
FC, NK, MMM and SEM designed the study. FC, NK, AZ enrolled the patients and collected the samples. FC, BRK, MFM and SEM analyzed the data. FC, MMM and SEM wrote the manuscript which was revised and approved by all co authors.
Contributor Information
Flora Chacha, Email: chachaf733@gmail.com.
Mariam M Mirambo, Email: mmmirambo@gmail.com.
Martha F Mushi, Email: marthamushi@yahoo.com.
Neema Kayange, Email: n_eema@yahoo.com.
Antke Zuechner, Email: antke.zuechner@web.de.
Benson R Kidenya, Email: benkidenya@yahoo.com.
Stephen E Mshana, Email: mshana72@yahoo.com.
References
- 1.Vergnano S, Sharland M, Kazembe P, Mwansambo C, Heath P. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2005;90(3):F220–FF224. doi: 10.1136/adc.2002.022863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Blencowe H, Cousens S. Review: addressing the challenge of neonatal mortality. Trop Med Int Health. 2013;18(3):303–312. doi: 10.1111/tmi.12048. [DOI] [PubMed] [Google Scholar]
- 3.Kayange N, Kamugisha E, Mwizamholya DL, Jeremiah S, Mshana SE. Predictors of positive blood culture and deaths among neonates with suspected neonatal sepsis in a tertiary hospital, Mwanza-Tanzania. BMC Pediatr. 2010;10(1):39. doi: 10.1186/1471-2431-10-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lim DV, Morales W, Walsh A, Kazanis D. Reduction of morbidity and mortality rates for neonatal group B streptococcal disease through early diagnosis and chemoprophylaxis. J Clin Microbiol. 1986;23(3):489–492. doi: 10.1128/jcm.23.3.489-492.1986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Paes BA, Modi A. Value of superficial cultures: diagnosing neonatal sepsis in a community hospital. Can Fam Physician. 1992;38:1796–1800. [PMC free article] [PubMed] [Google Scholar]
- 6.Mshana SE, Hain T, Domann E, Lyamuya EF, Chakraborty T, Imirzalioglu C. Predominance of klebsiella pneumoniae ST14 carrying CTX-M-15 causing neonatal sepsis in Tanzania. BMC Infect Dis. 2013;13:466. doi: 10.1186/1471-2334-13-466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Volante E, Moretti S, Pisani F, Bevilacqua G. Early diagnosis of bacterial infection in the neonate. J Matern Fetal Neonatal Med. 2004;16(2):13–16. doi: 10.1080/jmf.16.2.13.16. [DOI] [PubMed] [Google Scholar]
- 8.Thaver D, Zaidi AK. Burden of neonatal infections in developing countries: a review of evidence from community-based studies. Pediatr Infect Dis J. 2009;28(1):S3–S9. doi: 10.1097/INF.0b013e3181958755. [DOI] [PubMed] [Google Scholar]
- 9.Chiesa C, Panero A, Osborn JF, Simonetti AF, Pacifico L. Diagnosis of neonatal sepsis: a clinical and laboratory challenge. Clin Chem. 2004;50(2):279–287. doi: 10.1373/clinchem.2003.025171. [DOI] [PubMed] [Google Scholar]
- 10.Hofer N, Zacharias E, Mueller W, Resch B. An update on the use of C-reactive protein in early-onset neonatal sepsis: current insights and new tasks. Neonatology. 2012;102(1):25–36. doi: 10.1159/000336629. [DOI] [PubMed] [Google Scholar]
- 11.Group WYIS. Clinical prediction of serious bacterial infections in young infants in developing countries. Pediatr Infect Dis J. 1999;18(10):S23–S31. doi: 10.1097/00006454-199910001-00005. [DOI] [PubMed] [Google Scholar]
- 12.Buderer NMF. Statistical methodology: I. Incorporating the prevalence of disease into the sample size calculation for sensitivity and specificity. Acad Emerg Med. 1996;3(9):895–900. doi: 10.1111/j.1553-2712.1996.tb03538.x. [DOI] [PubMed] [Google Scholar]
- 13.Christopher A, Mshana SE, Kidenya BR, Hokororo A, Morona D. Bacteremia and resistant gram-negative pathogens among under-fives in Tanzania. Ital J Pediatr. 2013;39(1):27. doi: 10.1186/1824-7288-39-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mshana S, Kamugisha E, Miramb M, Chalya P, Rambau P, Mahalu W, Lyamuya E. Prevalence of clindamycin inducible resistance among methicillin-resistant staphylococcus aureus at Bugando Medical Centre, Mwanza, Tanzania. Tanzan J Health Res. 2009;11(2):59–64. [Google Scholar]
- 15.Wikler MA, Cockerill FR, Clinical and Laboratory Standards Institute . Performance Standards for Antimicrobial Susceptibility Testing: Eighteenth Informational Supplement. Wayne: Clinical and Laboratory Standards Institute; 2008. [Google Scholar]
- 16.Bhandari V, Wang C, Rinder C, Rinder H. Hematologic profile of sepsis in neonates: neutrophil CD64 as a diagnostic marker. Pediatrics. 2008;121(1):129–134. doi: 10.1542/peds.2007-1308. [DOI] [PubMed] [Google Scholar]
- 17.Mugalu J, Nakakeeto MK, Kiguli S, Kaddu-Mulindwa DH. Aetiology, risk factors and immediate outcome of bacteriologically confirmed neonatal septicaemia in Mulago Hospital, Uganda. Afr Health Sci. 2006;6(2):120–126. doi: 10.5555/afhs.2006.6.2.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mhada TV, Fredrick F, Matee MI, Massawe A. Neonatal sepsis at Muhimbili national hospital, Dar es salaam, Tanzania; aetiology, antimicrobial sensitivity pattern and clinical outcome. BMC Public Health. 2012;12(1):904. doi: 10.1186/1471-2458-12-904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.West BA, Peterside O, Ugwu RO, Eneh AU. Prospective evaluation of the usefulness of C-reactive protein in the diagnosis of neonatal sepsis in a sub-Saharan African region. Antimicrob Resist Infect Control. 2012;1(1):22. doi: 10.1186/2047-2994-1-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nuntnarumit P, Pinkaew O, Kitiwanwanich S. Predictive values of serial C-reactive protein in neonatal sepsis. J Med Assoc Thai. 2002;85(Suppl 4):S1151–1158. [PubMed] [Google Scholar]
- 21.Khassawneh M, Hayajneh WA, Kofahi H, Khader Y, Amarin Z, Daoud A. Diagnostic markers for neonatal sepsis: comparing C-reactive protein, interleukin-6 and immunoglobulin M. Scand J Immunol. 2007;65(2):171–175. doi: 10.1111/j.1365-3083.2006.01878.x. [DOI] [PubMed] [Google Scholar]
- 22.Polin RA. Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics. 2012;129(5):1006–1015. doi: 10.1542/peds.2012-0541. [DOI] [PubMed] [Google Scholar]
- 23.Malik A, Hui CP, Pennie RA, Kirpalani H. Beyond the complete blood cell count and C-reactive protein: a systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med. 2003;157(6):511–516. doi: 10.1001/archpedi.157.6.511. [DOI] [PubMed] [Google Scholar]
- 24.Alexandraki I, Palacio C. Gram-negative versus gram-positive bacteremia: what is more alarming. Crit Care. 2010;14:161. doi: 10.1186/cc9013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vallance H, Lockitch G. Rapid, semi-quantitative assay of C-reactive protein evaluated. Clin Chem. 1991;37(11):1981–1982. [PubMed] [Google Scholar]
- 26.Franz AR, Kron M, Pohlandt F, Steinbach G. Comparison of procalcitonin with interleukin 8, C-reactive protein and differential white blood cell count for the early diagnosis of bacterial infections in newborn infants. Pediatr Infect Dis J. 1999;18(8):666–671. doi: 10.1097/00006454-199908000-00003. [DOI] [PubMed] [Google Scholar]
- 27.Ohlsson A, Vearncombe M. Congenital and nosocomial sepsis in infants born in a regional perinatal unit: cause, outcome, and white blood cell response. Am J Obstet Gynecol. 1987;156(2):407–413. doi: 10.1016/0002-9378(87)90294-8. [DOI] [PubMed] [Google Scholar]
- 28.Yoon BH, Jun JK, Park KH, Syn HC, Gomez R, Romero R. Serum C-reactive protein, white blood cell count, and amniotic fluid white blood cell count in women with preterm premature rupture of membranes. Obstet Gynecol. 1996;88(6):1034–1040. doi: 10.1016/S0029-7844(96)00339-0. [DOI] [PubMed] [Google Scholar]
- 29.Du J, Li L, Dou Y, Li P, Chen R, Liu H. Diagnostic utility of neutrophil CD64 as a marker for early-onset sepsis in preterm neonates. PLoS One. 2014;9(7):e102647. doi: 10.1371/journal.pone.0102647. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pre-publication history
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2431/14/248/prepub