

Abstract
Background:
Neck and shoulder pains are the prevalent complaints among computer office workers. The purpose of this study was to assess the relationship of somatization tendency, expectation of pain, mental health and beliefs about causation of pain with persistence of neck/shoulder pains among computer office workers.
Methods:
This research is a kind of prospective cohort study with 1-year follow-up. It has done among all eligible computer office workers of Shahroud universities (n = 182) in 2008-2009 and 1-year later. Data were collected using the Cultural and Psychosocial Influences on Disability questionnaire. Multiple logistic regression analysis was used to analyze the data through SPSS (P < 0.05).
Results:
At the baseline 100 (54.9%) of participants reported neck/shoulder pains and at follow-up 34.3% of them reported persistence pains. Significant relationships were found between persistence of neck/shoulder pains and negative expectation about pain in next 1-year P = 0.002, (odds ratio [OR] =8.3, 95% confidence interval [CI]: 2.1-32.9) and somatization tendency P = 0.01, (OR = 6.5, 95% CI: 1.6-27.4).
Conclusions:
Pain expectation and somatization tendency recognized as associated risk factors of persistent neck/shoulder pain among computer operators. This confirmed some other similar studies on work-related musculoskeletal disorders in Europe countries in recent years.
Keywords: Beliefs, computer office workers, neck pain, shoulder pains, somatization tendency
INTRODUCTION
According to the previously conducted studies around the world, musculoskeletal disorders (MSDs) are the most prevalent disorders among computer operators.[1,2,3,4] The prevalence of the neck and shoulders pain is reported to be high, in comparison with the pains in the other limbs[1,5,6] that leading to sickness absence and disability, decreasing work efficiency,[7] and extensive costs upon the organizations and societies.[8,9] As a matter of fact, developing appropriate programs and prevention of work-related MSDs among workers is a national precedence in several countries.[10]
However, predictors of these diseases are relatively weak.[8] In addition, previously conducted studies have indicated that the related factors of persistent neck/shoulder pains can be different from the etiological factors.[11] In a study conducted by Grooten et al., it is reported that merely almost of only one-third of those who suffer from the neck/shoulder pains could release from these pains after 5-6 years.[8]
Although the relationship between MSDs and both individual and work-related factors have been studied and confirmed through various researches,[12,13] these recognized risk factors do not clarify unusual progressive modifications that have been detected in chronic pains and disabilities attributed to the prevalent MSDs. In 1980s, for instance, a disability resulted from arm pain became epidemic in Australia, which could not be found in the other countries with similar work conditions.[14] Furthermore, rate of disability due to back pain increased during the years of 1953-1992 in Britain, although the required physical load at work was largely decreasing.[15]
These findings have encouraged the hypothesis that the progress and persistence of nonspecific MSDs and related disabilities are influenced by culturally-determined health beliefs, in addition to mental health and physical activities.[16] Furthermore, several observations have been conducted which support the role of somatization tendency (i.e., a “general tendency to either report or worry about common somatic” (nonmusculoskeletal symptoms) on MSDs.[16,17,18,19]
In a longitudinal study conducted by Solidaki et al. among 518 nurses, office workers and postal clerks in Crete, it was found that persistence of MSDs significantly associated with somatising tendency, physical loading of work, and beliefs about work-causation of pain with odds ratio (OR) (95% confidence interval [CI]) of 2.6, 2.3 and 1.9 respectively.[17]
Ryall et al. in their studies on patients, who were receiving primary care and physiotherapy services, found that fear-avoidance beliefs and mental health are prognostic factors for arm pain.[20]
In addition, based on the study of Warnakulasuriya et al. among 852 computer operators, sewing machinists, nurses and postal workers in Sri Lanka, low mood and tendency to somatize were identified to be constantly associated with Musculoskeletal pains.[21]
Coggon et al., indicated that somatizing tendency, health beliefs, and low mood could influence the persistence of MSDs and related disabilities more than the rate of acute complaints.[22]
This study conducted considering above-mentioned findings, points and international differences in the prevalence of MSDs and related disabilities among occupational groups who are carrying out similar tasks, which is not completely clarified by the individual and psychosocial risk factors. Therefore, this study is aimed to assess the relationship of these new factors with persistence of neck/shoulder pains among computer office workers in Shahroud, Iran.
METHODS
Study design and participants
This is a prospective cohort study. All eligible computer office workers (n = 182) who were employed in four different universities of Shahroud University of Medical Sciences and its subsidiary units and hospitals, Shahroud University of Technology, Shahroud University of Quranic Sciences and Shahroud Azad University and its subsidiary hospital were selected and followed-up for 1-year. Inclusion criterion was at least 1-year experience of being a computer operator with at least 4 h/day of working with computer.
Study instrument
A standardized Cultural and Psychosocial Influences on Disability questionnaire[23] completed at the baseline (from July 2008 to March 2009) and 1-year later at follow-up was applied to collect the required data. Considering the base-line questionnaire, it was included with seven sections each one aimed to collect specific data. The first section was about the individual characteristics (e.g. gender, age, education etc.). For the second one, physical and psychosocial work-related factors (e.g., using a computer keyboard for longer than 4 h/day, manual lifting of weights ≥ 25 kg, repeated movements of the wrist or fingers for longer than 4 h in an average working day, time pressures, control at work, support from colleagues or supervisor, job satisfaction, decision latitude, job security, etc.) were included.
In the third section, 14 questions were included regarding the neck and shoulder pains (elements of Nordic Questionnaire)[23] and their disabilities for getting dressed and doing normal household jobs. Furthermore, a question about the expectation of pain (i.e., “if you expect your neck/shoulders pain would be a problem for you in next 12 months too?”) was added to this section. The next section, included with four questions about other people's pain (e.g., “do you know anyone who has had neck pain in the past 12 months’ at work or outside”).
In the section five, each worker was faced with five statements taken from Fear-Avoidance Beliefs Questionnaire[24] which were about their beliefs regarding the causation and prognosis of neck/shoulder pains. Three of the statements applied in this section were as the following: “How strongly the participant agreed with statements of the form,” “your work may cause you to develop musculoskeletal pain,” and “rest is needed to get better these problems.” The answers were categorized as “agree” in the cases that the one agrees completely with the statement or “tended to agree.” In the sixth section, seven questions (components of the Brief Symptom Inventory (BSI) questionnaire),[25] (faintness or dizziness, pains in the heart or chest, nausea or upset stomach, trouble getting breath, numbness or tingling in parts of your body that had been distressing during the past 7 days regarding the somatizing tendency) were applied.
Mental health by applying the relevant subscale of the Short Form-36 questionnaire[26] with five questions was the subject of the last section. Some of the questions included in that section are as the following: “During the past month were you a happy person?,” “Have you felt calm and peaceful?” and “have you been a very nervous person?”. Validity and reliability of these questionnaires have confirmed in many studies.[27,28,29]
In somatization tendency section, each symptom was scored 0-4, depending on the distress it caused.
Furthermore, the optional answers for mental health section were as the followings: “All of the time,” “most of the time,” “a good bit of the time,” “some of the time,” “a little of the time,” “none of the time.” The scores attributed to these answers ranged 0-6.
In somatization tendency and mental health section of questionnaire scores were summed and subjects were categorized into three bands, representing approximate thirds of the distribution (denoted low, middle, and high) for the whole sample.
At the base-line, the participants were asked about pains in their neck/shoulders lasted for at least a day over the past 12 months.
The follow-up questionnaire was shorter and after an interval of 12 months asked about pain in the last 1 month. Participants, who had declared their agreement for take part at follow-up, filled this questionnaire.
The original questionnaire by the author was translated from English to Farsi, and then by bilingual person it was back translated to English, also confirmed by occupational medicine specialists. The pilot study was conducted among 60 workers who were not included in this study in order to test whether the Farsi version of the questionnaire could be satisfactorily understood and completed.[30] Reliability of the questionnaire was tested with Chronbach alphas of 0.76.
In this study, neck/shoulder pains, was defined as the pains in the neck and/or either the shoulders. Furthermore, reported neck/shoulder pain lasting for at least a day over the previous 12 months at baseline and continuing presence of pain lasting for at least a day over 1-month at follow-up defined as persistent pain.
Ethical approval required to conduct this study was applied and received from the Research Committee of Shahroud University of Medical Sciences.
VARIABLES ASSESSMENT AND STATISTICAL ANALYSIS
In order to investigate the associations between persistence of neck/shoulder pains and all of the variables, initially univariate logistic regression was applied. Then in order to investigate the simultaneous relationships between these variables and the persistence of neck/shoulder pains (i.e., with the aim of effects of likely confounding factors can be controlled), all of the variables in the former process with age, job experience and educational level were entered into the multiple logistic regression analysis model. And, they were summarized as ORs with associated 95% CIs. The level of significance was set up at P < 0.05. For data analysis, SPSS (version 16, SPSS Inc., Chicago, IL)was used.
RESULTS
From 208 computer office workers employed in Shahroud universities, 182 (response rate 88%) completed the questionnaire at the baseline and 91.2% (166) of them participated at follow-up in 1-year later. Characteristics of the selected participants at the base-line and follow-up are summarized in Table 1.
Table 1.
Characteristics of study population at baseline and follow-up
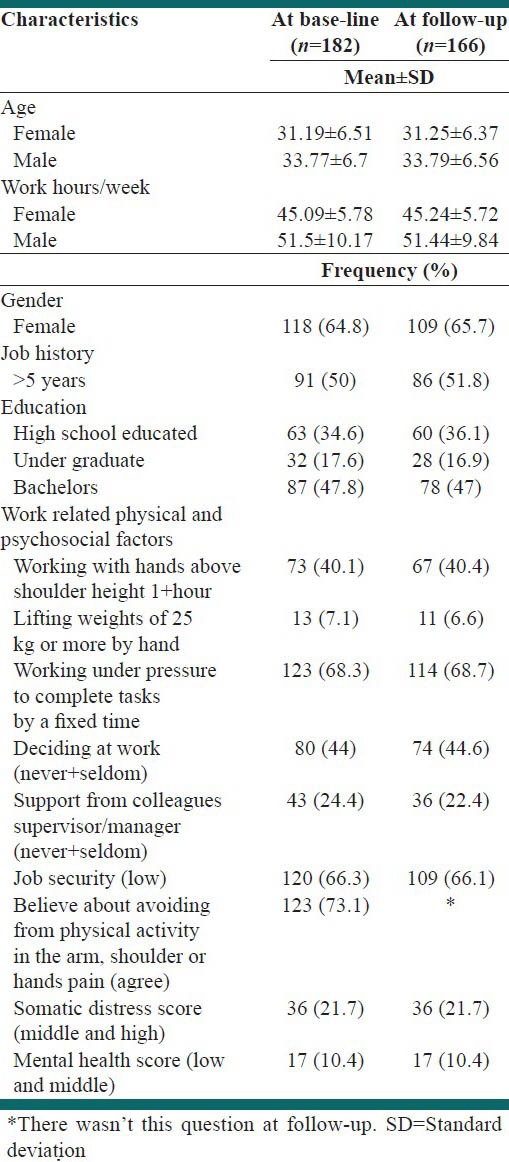
Mean age of the participants and weekly work hours were respectively 32.1 ± 6.7 (mean ± standard deviation [SD]) years and 47.4 ± 8.2 (mean ± SD). 50% (n = 81) of the study population had longer than 5 years’ experience of work. Most of the participants (64.8%) were females and 68.3% reported working under time pressure. In comparison with the females, the males significantly had more second jobs (P < 0.001).
At the baseline of the study, 54.9% (100) of computer operators reported neck/shoulder pains at previous 12 months. Prevalence of neck/shoulder pains among the females (63.6%) significantly (P < 0.002) was more than the males (39.1%).
57 (34.3%) of the participants who reported pains at the baseline, reported the pains 1-year later at follow-up. Persistence of neck/shoulder pains also among females was greater than males (40.4% vs. 22.8%).
However, based on the results derived from the follow-up, disability due to neck/shoulder pains was found to be higher among the females than the males. Disability in getting dressed was 57.7% among the females, in comparison with 28.6% found among the males. Furthermore, disability in performing the chores was 92.2% and 42.9% in the female and male participants. Referring to physician was 19 (57.6%) and the number of males who were visited by physicians was higher than the females (57.1% vs. 44.4%). Sickness absence due to neck/shoulder pains was just reported among the female participants at follow-up (25%).
Based on the results from surveying the related risk factors for persistent neck/shoulder pains which was conducted with using univariate logistic regression, significant relationships between persistent neck/shoulder pain and somatization tendency (P = 0.0), mental health (P = 0.002) and negative expectation of pain (P = 0.003) were found. The OR of this outcome was 5.9 times more in those categorized as the middle and high of somatization tendency, in comparison with the low category of somatization tendency and 3.2 times more in those with low and middle mental health scores versus high. Furthermore, persistent of neck/shoulder pains among participants with negative beliefs about expectation of pain was 4 times more than others haven’t this belief.
All variables in the former process with age, job experience and educational level were entered into the logistic regression analysis model. Finally, associated risk factors of persistent neck/shoulder pains among computer office workers were found to be somatization tendency (P = 0.01), and negative expectation of pain (P = 0.002) [Table 2]. Thus, after adjustment for confounding variables the OR for persistent neck/shoulder pain was 6.5 (1.6-27.4) in the middle and high versus the low category of somatization tendency score and 8.3 (2.1-32.9) in those with negative beliefs about expectation of pain. It means persistent of neck/shoulder pain among participants with middle and high score of somatization tendency is 6.5 times more than others with low score. Participants with negative beliefs about expectation of pain 8.3 times more exposed to these persistent pains. In our study, although no associations were found between persistent neck/shoulder pain and belief about work-relatedness of neck/shoulder pain and avoidance from physical activity in these pains, result showed these beliefs 1.8 times increase risk of persistent pain.
Table 2.
Physical, organizational, beliefs, somatization tendency and mental health, risk factors for neck/shoulder disorders adjusted for age, gender, and education
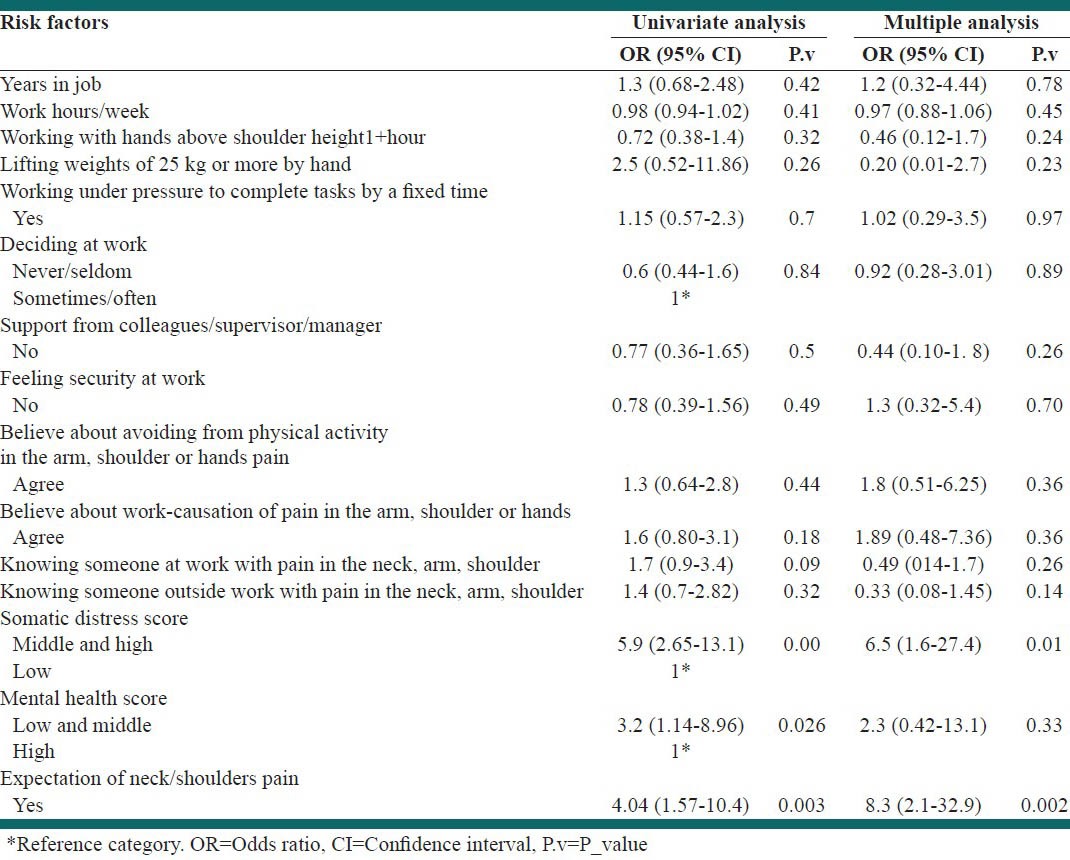
This study didn’t show significant association between individual factors includes work experience and work hours per week with persistent neck/shoulder pain, although work experience increases these pains (OR = 1.5). Furthermore, physical and psychosocial risk factors includes, lifting weights of 25 kg or more by hand, working with hands above shoulder height, working under pressure to complete tasks by a fixed time, deciding at work, support from colleagues/supervisor, security at work did not indicate significant association with persistent neck/shoulder pain.
On basis of the results, knowing someone at work and outside with pain in the neck, arm, shoulder and mental health did not indicate significant association with persistent neck/shoulder pain, but theses pains among workers with low and middle score of mental health were 2.3 times more than high score.
DISCUSSION
In this study, prevalence of neck or shoulder pains among computer operators was found to be 54.9%, which is <63% reported in a similar study conducted in USA,[31] and more than the results of studies conducted in Nicaragua (30% upper extremely pain)[32] and The Netherlands (neck/shoulder, arm 54%).[5] In a cross-sectional study performed by Choobineh et al., among computer operators working in banks of Shiraz, Iran, neck and shoulder pains with 59.6% and 58.2%, respectively, in previous 12 months of frequency were the most prevalent reported pains, which are higher than the results of the present study.[33] Some of the other studies have indicated a range of 10-62% of neck/shoulder pains among computer users.[34,35,36]
Based on the results, 34.3% of the subjects which reported neck/shoulder pains at base-line showed also persistence of these pains at follow-up, which is less than some studies. In a study conducted in Germany, 41% of the office workers reported persistence of shoulder pains after 1-year follow-up.[37] Juul-Kristensen and Jensen, indicated in their studies that 61% of office workers in 11 Danish companies showed the symptoms of persistence of neck/shoulder symptoms in days after 1-year follow-up while persistence of low back or elbow/hand region, were 53% and 41%, respectively.[38] These differences in prevalence and persistence of neck/shoulder pains could be related to different cultures, different compensation and insurance systems.
In this study, prevalence and persistence of neck/shoulder pains among female computer operators were found to be higher than the males which are consistent with the results of several previously conducted studies.[5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] Repetitive work with not as much of rest, increased contact with etiological causes and gender imbalance in domestic work are interlinking factors that explain gender differences in neck/shoulder pains.
Our results showed that the persistence of neck/shoulder pains at follow-up was strongly influenced by somatization tendency and negative expectation of pain at the baseline, raising risks some 6.5- and 8-fold.
Regarding to somatization tendency and MSDs, many similar studies have found significant relationships.[17,40] However, in a study conducted in Australia on three groups of workers including office workers, it was indicated that the relations between MSDS and somatization tendency was weak.[41] At the present, cognitive behavior therapy is suggested for somatizing tendency and negative belief about pain in many studies.
In a study in England among 1798 participants in working age, persistent arm pain was significantly prevalent in persons who believed that arm pain would be a problem in future 12 months[19] which is consistent with our findings. This is necebo effect. However, nocebo effects create completely from psychological bases and in many studies are related to anxiety; it can be either psychological or physiological. Studies have shown brain processes of pain and the central nervous system, especially nociceptive portions of insula, cingulate and thalamus may be influenced by expectations as psychological factor.[42]
Although in this study mental health was found to have significant relation with neck/shoulder pains, persistent of neck/shoulders pains among persons with low and medium score of mental health were 2.3 times more than others with high score.
In study by Palmer et al., persistent arm pain in persons with low score of mental health were significantly prevalent.[19]
A study by Andersen et al., among workers who were performing monotonous and repetitive work; it was shown that neck/shoulder disorders are strongly associated with decreasing of health-related quality of life.[43]
However, in this study, beliefs about causation and prognosis of neck/shoulder pains were not found to have significant relationships; it was greater among participant with these beliefs. In studies conducted by Gimeno et al., in Nicaragua[32] and Palmer et al., in England[19] workers’ health beliefs was significantly associated with MSDs.
In another study, health beliefs about prognosis of pain were associated with the change from nondisabling to disabling MSDs (OR 3.7).[44]
Furthermore, the results of this study showed that refereeing to physician for neck/shoulder pains was 57.6% and sickness absence due to neck/shoulder pain was 25% which both are higher than some previously conducted studies (21-38%) and (13-21%), respectively.[7] It may be related to sickness absence compensation, work conditions, and belief about recovery of pain.
This study introduces several potential psychological risk factors, which could be helpful for healthcare in assessing the prognosis of patient with neck/shoulder pain. Our study confirms the importance of somatizing tendency and negative expectation about pain as risk factors for persistence of neck/shoulder pain among computer office workers. This finding is novel in our country and needs to be independently replicated in other occupations. However, it suggests that interventions with the aim of reducing the persistence of neck/shoulder pain should focus on recognizing somatization tendency by clinicians and modifying negative expectation about neck shoulders pain and generally ergonomic intervention should be account not only for prevention of injury but also for pleasing workplaces and reducing psychological risk factors.
This study was self-reported questionnaire based survey and this is the limitation of this work. However, standardized questionnaire of many important risk factors, including physical, psychological, social and cultural, with follow-up design and high response rate are the points of strength in this study.
Future studies should consider the importance of all the risk factors during longer follow-up interval and workplace interventions about worker's health beliefs and somatization tendency and cognitive behavior therapy.
CONCLUSIONS
This study showed that neck/shoulder pains still pose a major problem among computer office workers and somatization tendency and negative expected pain at the baseline of the study are risk factors for persistent neck/shoulder pain after 1-year follow-up. This confirms similar studies in Europe countries and importance of psychological factors on work related MSD in recent years.
ACKNOWLEDGMENT
We thank the Research Deputy of Shahroud University of Medical Sciences for financial support of this project (NO. 8943), and Professor David Coggon from UK for valuable support of this study and all who participated in the study.
Footnotes
Source of Support: We thank the Research Deputy of Shahroud University of Medical Sciences for financial support of this project (NO. 8943), and Professor David Coggon from UK for valuable support of this study and all who participated in the study
Conflict of Interest: None declared.
REFERENCES
- 1.Wu S, He L, Li J, Wang J, Wang S. Visual display terminal use increases the prevalence and risk of work-related musculoskeletal disorders among Chinese office workers: A cross-sectional study. J Occup Health. 2012;54:34–43. doi: 10.1539/joh.11-0119-oa. [DOI] [PubMed] [Google Scholar]
- 2.Ranasinghe P, Perera YS, Lamabadusuriya DA, Kulatunga S, Jayawardana N, Rajapakse S, et al. Work related complaints of neck, shoulder and arm among computer office workers: A cross-sectional evaluation of prevalence and risk factors in a developing country. Environ Health. 2011;10:70. doi: 10.1186/1476-069X-10-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eltayeb SM, Staal JB, Khamis AH, de Bie RA. Symptoms of neck, shoulder, forearms, and hands: A cohort study among computer office workers in Sudan. Clin J Pain. 2011;27:275–81. doi: 10.1097/AJP.0b013e3181fe94ef. [DOI] [PubMed] [Google Scholar]
- 4.Ortiz-Hernández L, Tamez-González S, Martínez-Alcántara S, Méndez-Ramírez I. Computer use increases the risk of musculoskeletal disorders among newspaper office workers. Arch Med Res. 2003;34:331–42. doi: 10.1016/S0188-4409(03)00053-5. [DOI] [PubMed] [Google Scholar]
- 5.Eltayeb S, Staal JB, Kennes J, Lamberts PH, de Bie RA. Prevalence of complaints of arm, neck and shoulder among computer office workers and psychometric evaluation of a risk factor questionnaire. BMC Musculoskelet Disord. 2007;8:68. doi: 10.1186/1471-2474-8-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ranasinghe P, Perera YS, Lamabadusuriya DA, Kulatunga S, Jayawardana N, Rajapakse S, et al. Work-related complaints of arm, neck and shoulder among computer office workers in an Asian country: Prevalence and validation of a risk-factor questionnaire. BMC Musculoskelet Disord. 2011;12:68. doi: 10.1186/1471-2474-12-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Luime JJ, Koes BW, Miedem HS, Verhaar JA, Burdorf A. High incidence and recurrence of shoulder and neck pain in nursing home employees was demonstrated during a 2-year follow-up. J Clin Epidemiol. 2005;58:407–13. doi: 10.1016/j.jclinepi.2004.01.022. [DOI] [PubMed] [Google Scholar]
- 8.Grooten WJ, Mulder M, Josephson M, Alfredsson L, Wiktorin C. The influence of work-related exposures on the prognosis of neck/shoulder pain. Eur Spine J. 2007;16:2083–91. doi: 10.1007/s00586-007-0481-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hill J, Lewis M, Papageorgiou AC, Dziedzic K, Croft P. Predicting persistent neck pain: A 1-year follow-up of a population cohort. Spine (Phila Pa 1976) 2004;29:1648–54. doi: 10.1097/01.brs.0000132307.06321.3c. [DOI] [PubMed] [Google Scholar]
- 10.Spielholz P, Silverstein B, Morgan M, Checkoway H, Kaufman J. Comparison of self-report, video observation and direct measurement methods for upper extremity musculoskeletal disorder physical risk factors. Ergonomics. 2001;44:588–613. doi: 10.1080/00140130118050. [DOI] [PubMed] [Google Scholar]
- 11.Lassen CF, Mikkelsen S, Kryger AI, Andersen JH. Risk factors for persistent elbow, forearm and hand pain among computer workers. Scand J Work Environ Health. 2005;31:122–31. doi: 10.5271/sjweh.859. [DOI] [PubMed] [Google Scholar]
- 12.Waersted M, Hanvold TN, Veiersted KB. Computer work and musculoskeletal disorders of the neck and upper extremity: A systematic review. BMC Musculoskelet Disord. 2010;11:79. doi: 10.1186/1471-2474-11-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Habibi E, Pourabdian S, Atabaki AK, Hoseini M. Evaluation of work-related psychosocial and ergonomics factors in relation to low back discomfort in emergency unit nurses. Int J Prev Med. 2012;3:564–8. [PMC free article] [PubMed] [Google Scholar]
- 14.Gun RT. The incidence and distribution of RSI in South Australia 1980-81 to 1986-87. Med J Aust. 1990;153:376–80. doi: 10.5694/j.1326-5377.1990.tb125492.x. [DOI] [PubMed] [Google Scholar]
- 15.Clinical Standards Advisory Group. London: HMSO; 1994. Epidemiology Review: The Epidemiology and Cost of Back Pain. [Google Scholar]
- 16.Coggon D. Occupational medicine at a turning point. Occup Environ Med. 2005;62:281–3. doi: 10.1136/oem.2004.017335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Solidaki E, Chatzi L, Bitsios P, Coggon D, Palmer KT, Kogevinas M. Risk factors for new onset and persistence of multi-site musculoskeletal pain in a longitudinal study of workers in Crete. Occup Environ Med. 2013;70:29–34. doi: 10.1136/oemed-2012-100689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McBeth J, Macfarlane GJ, Hunt IM, Silman AJ. Risk factors for persistent chronic widespread pain: A community. based study. Rheumatology (Oxford) 2001;40:95–101. doi: 10.1093/rheumatology/40.1.95. [DOI] [PubMed] [Google Scholar]
- 19.Palmer KT, Reading I, Linaker C, Calnan M, Coggon D. Population-based cohort study of incident and persistent arm pain: Role of mental health, self-rated health and health beliefs. Pain. 2008;136:30–7. doi: 10.1016/j.pain.2007.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ryall C, Coggon D, Peveler R, Poole J, Palmer KT. A prospective cohort study of arm pain in primary care and physiotherapy – Prognostic determinants. Rheumatology (Oxford) 2007;46:508–15. doi: 10.1093/rheumatology/kel320. [DOI] [PubMed] [Google Scholar]
- 21.Warnakulasuriya SS, Peiris-John RJ, Coggon D, Ntani G, Sathiakumar N, Wickremasinghe AR. Musculoskeletal pain in four occupational populations in Sri Lanka. Occup Med (Lond) 2012;62:269–72. doi: 10.1093/occmed/kqs057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Coggon D, Ntani G, Palmer KT, Felli VE, Harari R, Barrero LH, et al. The CUPID (Cultural and Psychosocial Influences on Disability) study: Methods of data collection and characteristics of study sample. PLoS One. 2012;7:e39820. doi: 10.1371/journal.pone.0039820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 24.Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52:157–68. doi: 10.1016/0304-3959(93)90127-B. [DOI] [PubMed] [Google Scholar]
- 25.Derogatis LR, Melisaratos N. The brief symptom inventory: An introductory report. Psychol Med. 1983;13:595–605. [PubMed] [Google Scholar]
- 26.Ware JE. Institute for the Improvement of Medical Care and Health. Quality Quest Inc; 1989. SF-36 Health Status Questionnaire. Boston, MA. [Google Scholar]
- 27.Rostami M, Noorian N, Mansournia MA, Sharafi E, Babaki AE, Kordi R. Validation of the Persian version of the fear avoidance belief questionnaire in patients with low back pain. J Back Musculoskelet Rehabil. 2014;27:213–21. doi: 10.3233/BMR-130439. [DOI] [PubMed] [Google Scholar]
- 28.Sahin NH, Durak Batigün A, Ugurtas S. The validity, reliability and factor structure of the brief symptom inventory (BSI) Turk Psikiyatri Derg. 2002;13:125–35. [PubMed] [Google Scholar]
- 29.Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The short form health survey (SF-36): Translation and validation study of the Iranian version. Qual Life Res. 2005;14:875–82. doi: 10.1007/s11136-004-1014-5. [DOI] [PubMed] [Google Scholar]
- 30.Sadeghian F, Sadeghian A, Raei M, Kasaeian A. Musculoskeletal disorders among oil field workers: Influences of health beliefs, mental health and somatisation tendency. J Med Sci. 2012;12:114–20. [Google Scholar]
- 31.Gerr F, Marcus M, Ensor C, Kleinbaum D, Cohen S, Edwards A, et al. A prospective study of computer users: I. Study design and incidence of musculoskeletal symptoms and disorders. Am J Ind Med. 2002;41:221–35. doi: 10.1002/ajim.10066. [DOI] [PubMed] [Google Scholar]
- 32.Gimeno D, Felknor SA, Adejumo R, Aragon A, Berrios A, Salazar E, et al. Psychosocial factors and musculoskeletal symptoms in a vulnerable working population in Nicaragua. Occup Environ Med. 2011;68(Suupl):1. A70. [Google Scholar]
- 33.Choobineh A, Nouri E, Arjmandzadeh A, Mohamadbaigi A. Musculoskeletal disorders among bank computer operators. Iran Occup Health J. 2006;3:12–7. [Google Scholar]
- 34.Jensen C, Finsen L, Søgaard K, Christensen H. Musculoskeletal symptoms and duration of computer and mouse use. Int J Ind Ergon. 2002;30:265–75. [Google Scholar]
- 35.Karlqvist LK, Hagberg M, Köster M, Wenemark M, Nell R. Musculoskeletal symptoms among computer-assisted design (CAD) operators and evaluation of a self-assessment questionnaire. Int J Occup Environ Health. 1996;2:185–94. doi: 10.1179/oeh.1996.2.3.185. [DOI] [PubMed] [Google Scholar]
- 36.Bergqvist U, Wolgast E, Nilsson B, Voss M. Musculoskeletal disorders among visual display terminal workers: Individual, ergonomic, and work organizational factors. Ergonomics. 1995;38:763–76. doi: 10.1080/00140139508925148. [DOI] [PubMed] [Google Scholar]
- 37.van der Windt DA, Koes BW, Boeke AJ, Devillé W, De Jong BA, Bouter LM. Shoulder disorders in general practice: Prognostic indicators of outcome. Br J Gen Pract. 1996;46:519–23. [PMC free article] [PubMed] [Google Scholar]
- 38.Juul-Kristensen B, Jensen C. Self-reported workplace related ergonomic conditions as prognostic factors for musculoskeletal symptoms: The “BIT” follow up study on office workers. Occup Environ Med. 2005;62:188–94. doi: 10.1136/oem.2004.013920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cassou B, Derriennic F, Monfort C, Norton J, Touranchet A. Chronic neck and shoulder pain, age, and working conditions: Longitudinal results from a large random sample in France. Occup Environ Med. 2002;59:537–44. doi: 10.1136/oem.59.8.537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Matsudaira K, Palmer KT, Reading I, Hirai M, Yoshimura N, Coggon D. Prevalence and correlates of regional pain and associated disability in Japanese workers. Occup Environ Med. 2011;68:191–6. doi: 10.1136/oem.2009.053645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Harcombe H, McBride D, Derrett S, Gray A. Physical and psychosocial risk factors for musculoskeletal disorders in New Zealand nurses, postal workers and office workers. Inj Prev. 2010;16:96–100. doi: 10.1136/ip.2009.021766. [DOI] [PubMed] [Google Scholar]
- 42.Atlas LY, Wager TD. How expectations shape pain. Neurosci Lett. 2012;520:140–8. doi: 10.1016/j.neulet.2012.03.039. [DOI] [PubMed] [Google Scholar]
- 43.Andersen JH, Kaergaard A, Frost P, Thomsen JF, Bonde JP, Fallentin N, et al. Physical, psychosocial, and individual risk factors for neck/shoulder pain with pressure tenderness in the muscles among workers performing monotonous, repetitive work. Spine (Phila Pa 1976) 2002;27:660–7. doi: 10.1097/00007632-200203150-00017. [DOI] [PubMed] [Google Scholar]
- 44.Vargas-Prada S, Martínez JM, Coggon D, Delclos G, Benavides FG, Serra C. Health beliefs, low mood, and somatizing tendency: Contribution to incidence and persistence of musculoskeletal pain with and without reported disability. Scand J Work Environ Health. 2013;39:589–98. doi: 10.5271/sjweh.3377. [DOI] [PMC free article] [PubMed] [Google Scholar]