

Abstract
Background:
The aim of this report was to assess the efficacy and safety of a combination of vitamin E, an antioxidant, and Eve Primrose in the management of painful diabetes mellitus (DM) neuropathy.
Materials and Methods:
This was an interventional study that evaluated the efficacy and safety of a combination of vitamin E and Eve Primrose in the management of DM neuropathy. The study was conducted at the Diabetic Centre of the Lagos State University Teaching Hospital, Ikeja. Eighty individuals with type 2 DM who had painful neuropathy were recruited for this study, which took place for a duration of 1 year. The study subjects underwent clinical and biochemical assessment at baseline and were given vitamin E in a dose of 400 mg in combination with Eve Primrose in doses ranging 500-1000 mg/day. They were afterward assessed for relief of symptoms and possible untoward effects after 2 weeks and, thereafter, monthly for 3 months. The main outcome measure was amelioration of symptoms of neuropathy.
Results:
The mean age and age range of the study subjects were 58.2 years and 37-70 years, respectively. A total of 70 patients (88%) of the study population reported relief from neuropathic pains. Clinical parameters were comparable between the responders and non-responders. One characteristic feature of the non-responders was that they all had vibration perception threshold of ≥25 mV, which was indicative of severe neuropathy.
Conclusion:
The combination of vitamin E and Eve Primrose is beneficial in the management of mild to moderate diabetic neuropathy.
Keywords: Diabetes mellitus, Eve Primrose, neuropathy, vitamin E
INTRODUCTION
Diabetes mellitus (DM) neuropathy (DMN) is a long-term microvascular complication that is highly contributory to DM associated morbidity.[1] DMN represents a major health problem being responsible for substantial morbidity, increased mortality, and impaired quality of life in those affected. The reported prevalence rates of DM neuropathy in Nigerians is 70-80%,[2] with sensori-motor type being the commonly documented form of neuropathy. In a study from the United Kingdoms, the prevalence of painful diabetic peripheral neuropathy was found to be 26.4% and it was noted that this all-important complication of DM had a significant negative effect on the quality of life.[3]
Botanicals and dietary supplements that have been found to improve symptoms of neuropathy without affecting glucose control include Evening Primrose (EP) oil, alpha-lipoic acid, capsaicin, and vitamin E. EP oil is a rich source of omega-6 essential fatty acids, primarily gamma-linolenic acid (GLA) and linoleic acid, both are essential components of myelin and the neuronal cell membrane. Given the high burden of neuropathy and the limited treatment options available in our setting for its management, it is thus desirable that pharmacotherapy for neuropathy that combines efficacy and accessibility be made available. Such an agent that combines the above stated characteristics and has been used elsewhere in the management of DM neuropathy is EP oil.[4,5] Vitamin E, a group of compounds that includes tocopherols and tocotrienols that are potent lipophilic antioxidants,[6] has also been found to ameliorate the unpleasant effects of the neuropathic complications of DM.[4,5] The recommended dosage of EP oil for the treatment of DMN is 500-1000 mg daily. Vitamin E, like EP oil, is available in the form of soft gels and usually administered in doses of 400 mg for DMN.
The aims of this report are to assess the efficacy of EP and vitamin E in the amelioration of the symptoms of painful neuropathy and to determine the safety profile of EP and vitamin E in patients with neuropathy.
MATERIALS AND METHODS
Eighty individuals with type 2 DM, who had histories of painful neuropathy and were aged >30 years were recruited for this study, which was conducted at the Diabetes Centre of the Lagos State University Teaching Hospital (LASUTH), Ikeja. Approval was given by the Ethics committee of LASUTH and the research procedures were in accordance with the Helsinki Declaration.
The Study duration was for a year from December 2010 to December 2011.
The inclusion criteria were as follows: Patients with DM aged >30 years and 70 years; patients with a diagnosis of painful neuropathy; patients with DM neuropathy who are treatment naïve; and patients who consented to the study by completing the informed consent form.
The exclusion criteria were as follows: Patients with DM who were pregnant; patients who had indications for hospitalizations for medical or surgical reasons; patients who are presently on treatment of neuropathy; patients with histories of psychiatry disorder and patients with histories of seizure disorder.
Questionnaires, which were interviewer administered, were used to obtain histories on biodata, histories pertaining to DM, and glucose lowering medications used. Questions relating to neuropathy were derived from the Michigan Neuropathy Screening Instrument.[7]
All study subjects were examined and physical examination included determination of anthropometric indices and blood pressure measurements.
Vibration perception thresholds (VPTs) were determined using a hand-held digital Biothesiometer (BM) Vibrometer VPT (Diabetik Foot India). Biothesiometry was performed in all patients in the supine position to determine the VPT.
Blood pressure measurements with the patient supine and upright were measured.
The study subjects were given a daily combination of EP oil in doses ranging from 500-1000 mg and vitamin E in a dosing strength of 400 mg. The symptoms of neuropathic pain were assessed after 2 weeks of administration of EP and vitamin E and, subsequently, every month for a 12-week period.
At every visit after commencement of EP oil and vitamin E treatment, the study participants were asked about any untoward effects of the drugs.
Operational diagnosis/definitions
Neuropathic pain was said to present in the presence of any of the following symptoms: Burning, peppery, throbbing, shooting, and electric shock sensations. Severe neuropathy referred to the presence of any of the symptoms listed above and a VPT of ≥25 V
Good glycemic control was defined as a glycosylated hemoglobin level of <7%
Responders referred to patients who observed that there was sustained amelioration of burning pain sensation, following at least 2 weeks of administration of a combination of EP and vitamin E.
Statistical analysis was carried out using SPSS version 17. Student's t test was used for analysis of quantitative variables. We compared clinical and biochemical parameters between responders to the combination of vitamin E and EP and non-responders to these drugs. P ≤ 0.05 was considered statistically significant.
RESULTS
The females were 51 in number and this made up 64% of the study population. The mean age of both sexes were comparable (M: 56.3 years vs F: 59.2 years, P = 0.2).
Hypertension was present in 28 (35%) of the subjects.
The majority of the subjects (86%) had poor long-term glycemic control.
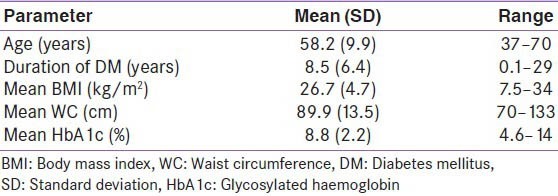
VPT values ranged from 6 to 45 mV. The baseline clinical characteristics of the study subjects are shown in Table 1.
Table 1.
Clinical characteristics of the study subjects
Treatment type for DM
Well over half of the study subjects were on oral hypoglycemic agents (OHA). The distribution of glucose lowering agent in the study subjects showed that 48 (60%) were on OHAs, 20 (25%) were on combinations of insulin and OHAs, and 12 (15%) were on sole insulin therapy.
Response to vitamin E and EP oil
A total of 70 (88%) of the study subject admitted to relief from “burning pain,” and this was noticed 2 weeks following usage of the combination of vitamin E and EP oil. The relief from neuropathic symptoms was sustained a month following the first and subsequent visits. There were no untoward effects reported by the responders and non-responders. It is pertinent to note that all 10 non-responders had severe neuropathy.
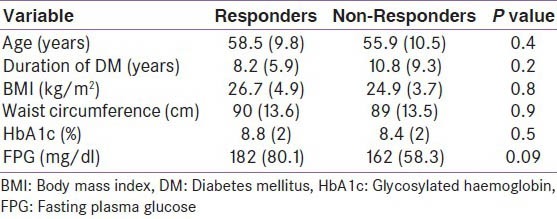
Clinical and biochemical parameters were comparable between responders and non-responders. These results are shown in Table 2.
Table 2.
Comparison of clinical and biochemical parameters between responders and non-responders
DISCUSSION
DM-associated neuropathy is a long-term complication of DM that is often associated with great morbidity and is also implicated in the pathogenesis of foot ulceration.
Pain relief is one of the most challenging issues in diabetic neuropathy.
We have shown in this report that painful neuropathy in DM is often ameliorated following treatment with the combination of vitamin E and EP. Well over half of the study subjects with DMN responded positively to the combination of vitamin E and EP in dosages ranging from 400 mg and 500-1000 mg, respectively, for both drugs. The possible role of vitamin E in the management of diabetic neuropathy may be attributed to the concept of oxidative stress and antioxidant treatment,[6] which has been shown to play a role in experimental diabetic neuropathy. Some researchers have shown that defective nerve conduction in diabetic subjects with mild-moderate peripheral neuropathy may be improved by pharmacological doses of vitamin E supplementation.[8] In a randomized, double-blind, placebo-controlled trial, which evaluated the effect of vitamin E on nerve function in 21 type 2 diabetic patients diagnosed with mild-to-moderate neuropathy, the results showed a reduction of symptoms.[9]
GLA, the major component of EP oil has been widely studied in the management of diabetic neuropathy and has been found to be useful in this regards.[4,10] In a multi-centre trial, GLA at a dose of 480 mg/day was found to have a beneficial effect on the course of diabetic neuropathy irrespective of sex, age, and type of diabetes.[10] The reason for the beneficial role of GLA in the management of DM neuropathy may be adduced to impaired conversion of linoleic acid to GLA, which had been demonstrated in animals with diabetes and inferred from fatty acid profiles in human diabetes.[11] In our report, GLA at doses of 500-1000 mg/day were found to be beneficial for the management of painful DMN.
It is pertinent to note that none of the study subjects reported untoward effects with the combination of vitamin E and GLA, and this is despite the fact that some were on blood pressure lowering medications. This finding is not unexpected, given the fact that vitamin E is relatively non-toxic and most long-term trials had found no negative side effects with its supplementation.[11,12,13]
It is notable that the clinical and biochemical features were comparable between responders and non-responders. Importantly, high VPTs were constant features of non responders. From these findings, it may be safely inferred that other than the severity of neuropathy as defined by a high VPT, age, duration of DM, glycemic control, and anthropometric indices do not influence response to treatment of DPN with vitamin E and EP oil.
There were no untoward effects of vitamin E and EP oil reported by the study participants.
CONCLUSION
The combination of vitamin E and EP oil is effective and safe in the management of mild to moderate neuropathy and in individuals with DM who have severe neuropathy and may have to resort to other management options.
Footnotes
Source of Support: Strides Vital Nigeria Limited
Conflict of Interest: None declared.
REFERENCES
- 1.Ogbera AO, Fasanmade OA, Chinenye S, Akinlade A. Characterization of lipid parameters in diabetes mellitus. Int Arch Med. 2009;20:19. doi: 10.1186/1755-7682-2-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ugoya SO, Echejoh GO, Ugoya TA, Agaba EI, Puepet FH, Ogunniyi A. Clinically diagnosed diabetic neuropathy: Frequency, types and severity. J Natl Med Assoc. 2006;98:1763–6. [PMC free article] [PubMed] [Google Scholar]
- 3.Davies M, Brophy S, Williams R, Taylor A. The prevalence, severity, and impact of painful diabetic neuropathy in type 2 diabetes. Diabet Care. 2006;29:1518–22. doi: 10.2337/dc05-2228. [DOI] [PubMed] [Google Scholar]
- 4.Keen H, Payan J, Allawi J, Walker J, Jamal GA, Weir AI, et al. Treatment of diabetic neuropathy with gamma-linolenic acid. The gamma-Linolenic Acid Multicenter Trial Group. Diabet Care. 1993;16:8–15. doi: 10.2337/diacare.16.1.8. [DOI] [PubMed] [Google Scholar]
- 5.Backonja M, Beydoun A, Edwards KR, Schwartz SL, Fonseca V, Hes M, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA. 1998;280:1831–6. doi: 10.1001/jama.280.21.1831. [DOI] [PubMed] [Google Scholar]
- 6.Connell SO. Select vitamins and minerals in the management of diabetes. Diabetes Spectr. 2001;14:133–48. [Google Scholar]
- 7.Moghtaderi A, Bakhshipour A, Rashidi H. Validation of Michigan neuropathy screening instrument for diabetic peripheral neuropathy. Clin Neurol Neurosurg. 2006;108:477–81. doi: 10.1016/j.clineuro.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 8.Tutuncu NB, Bayraktar N, Varli K. Reversal of defective nerve conduction with vitamin E supplementation in type 2 diabetes. Diabet Care. 1998;21:1915–8. doi: 10.2337/diacare.21.11.1915. [DOI] [PubMed] [Google Scholar]
- 9.Jamal GA, Carmichael H. The effect of gamma-linolenic acid on human diabetic neuropathy: A double-blind placebo–controlled trial. Diabet Met. 1990;7:319–23. doi: 10.1111/j.1464-5491.1990.tb01397.x. [DOI] [PubMed] [Google Scholar]
- 10.Horrobin DF. Essential fatty acids in the management of impaired nerve function in diabetes. Diabetes. 1997;46:S90–3. doi: 10.2337/diab.46.2.s90. [DOI] [PubMed] [Google Scholar]
- 11.Stephens NG, Parsons A, Schofield PM, Kelly F, Cheeseman K, Mitchison MJ. Randomized controlled trial of vitamin E in patients with coronary disease: Cambridge Heart Antioxidant Study. Lancet. 1996;347:781–6. doi: 10.1016/s0140-6736(96)90866-1. [DOI] [PubMed] [Google Scholar]
- 12.Jain SK. Should high-dose vitamin E supplementation be recommended to diabetic patients? Diabet Care. 1999;22:1242–4. doi: 10.2337/diacare.22.8.1242. [DOI] [PubMed] [Google Scholar]
- 13.Low PA, Nickander KK, Tritschler HJ. The roles of oxidative stress and antioxidant treatment in experimental neuropathy. Diabetes. 1997;46:S38–42. doi: 10.2337/diab.46.2.s38. [DOI] [PubMed] [Google Scholar]