

Abstract
Trastuzumab that targets human epidermal growth factor receptor 2 (HER2) protein is the only approved molecular targeting agent for treating gastric cancer in Japan and the outcomes have been favorable. However, trastuzumab is effective for only 10% to 20% of the population with gastric cancer that expresses HER2 protein. Molecular targeting therapy with bevacizumab against vascular endothelial growth factors (VEGF) and with cetuximab and panitumumab against the epidermal growth factors pathway that have been approved for treating colorectal cancer are not considered effective for treating gastric cancer according to several clinical trials. However, ramucirumab that targets VEGF receptor-2 prolonged overall survival in a large phase III clinical trial and it might be an effective molecular targeting therapy for gastric cancer. The significance of molecular targeting therapy for gastric cancer remains controversial. A large-scale randomized clinical trial of novel molecular targeting agents with which to treat gastric cancer is needed.
Keywords: Gastric cancer, Molecular targeting therapy, Human epidermal growth factor receptor 2 protein, Vascular endothelial growth factors/Vascular endothelial growth factor receptor pathway, Epidermal growth factors pathway
Core tip: So far, trastuzumab is the only molecular targeting therapy that has been approved for treating gastric cancer. The significance of molecular targeting therapy for gastric cancer remains controversial, but large scale randomized clinical trials might confirm the benefits of other novel molecular targeting therapies for gastric cancer in the near future.
INTRODUCTION
Gastric cancer is the fourth most common cancer worldwide; 603003 and 330290 new diagnoses for men and women, respectively, were recorded during 2002[1]. The disease is associated with an annual death rate of 700000, making it the second most common cause of cancer death worldwide[2]. The geographic variation in prevalence is remarkable, as 60% of gastric cancers arise in East Asia[3,4]. Although the incidence of gastric cancer is declining in western countries, the frequency of adenocarcinomas of the gastro-esophageal junction (GEJ) is increasing[3-6]. Surgery and perioperative therapy are potentially curative strategies for treating patients with resectable cancer. However, most patients with gastric cancer have stage IV disease at presentation and thus are candidates for palliative chemotherapy. The median survival of patients with advanced gastric cancer who do not receive chemotherapy is 3-4 mo. Chemotherapy plays an important role in the treatment of advanced gastric cancer, but an effective chemotherapy regimen for unresectable or recurrent gastric carcinoma was not established until the 1990s. The new oral fluoropyrimidine S-1, which comprises tegafur, 5-chloro-2,4-dihydropyrimidine and potassium oxonate, was recognized as being effective against gastric cancer during the mid-1990s[7]. The recent Japanese ACTS-GC trial demonstrated the effectiveness of S-1 against stage II-III gastric cancer after curative resection with D2 lymphadenectomy, and S-1 improved the 3-year overall survival (OS) rate from 70.1% for surgery alone to 80.1%[8]. Several novel chemotherapeutic agents, including irinotecan (CPT-11), taxanes (paclitaxel and docetaxel), and oxaliplatin, in combination with S-1, have offered hope for improving the outcomes of patients with gastric cancer[9-11]. The recent response rates to several chemotherapy regimens, such as S-1 with cisplatin in the SPIRITS trial, have been remarkably high[12], and this regimen is frequently administered as a first-line chemotherapy, with good results against advanced disease[13]. However, the prognosis of advanced or recurrent gastric cancer remains unsatisfactory. We believe that molecular targeting therapy will increase the survival rates of patients with advanced or recurrent gastric cancer.
To date, various factors, such as epidermal growth factors (EGFR) including HER2, VEGF, FEGFR, and mammalian target of rapamycin (mTOR), have been considered as targets of therapy of gastric cancer. Monoclonal antibodies (trastuzumab, bevacizumab, ramucirumab, cetuximab, and panitumumab), tyrosine kinase inhibitors (sunitinib and lapatinib) and an mTOR inhibitor (everolimus) have been administered to patients with gastric cancer in various clinical trials. However, molecular targeting therapy is less effective against gastric cancer compared with other cancers such as colorectal and breast cancers. In fact, only trastuzumab, which is a fully humanized monoclonal antibody that binds to the extracellular domain of the HER2 receptor, is available for treating gastric cancer. Here, we describe molecular targeting therapy for gastric cancer and review clinical trials.
TRASTUZUMAB
The 185-kDa HER2 protein is encoded by a gene located on chromosome 17q21. It is a transmembrane tyrosine kinase receptor with an extracellular ligand-binding domain that comprises a short transmembrane domain and an intracellular domain that has kinase activity. The HER2 protein is a member of the epidermal growth factor (EGFR) family of growth factors that comprises structurally related HER1 or ErbB1, also known as EGFR, HER2 or ErbB2, HER3 or ErbB3 and HER4 or ErbB4. HER2 receptors also localize in the nucleus, where they function as transcription factors for cyclin D1 and p53[14,15]. Therefore, HER2 (also known as c-erbB-2/neu) acts as an oncogene that is involved in the regulation of cell proliferation, differentiation, motility and apoptosis[16-20] (Figure 1).
Figure 1.
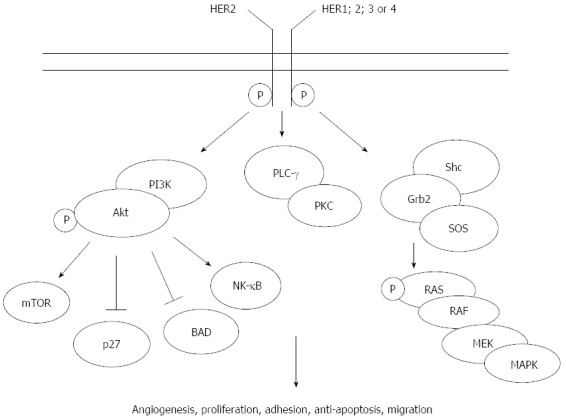
Human epidermal growth factor receptor 2 signaling pathways. HER: Human epidermal growth factor receptor; BAD: Bcl-2-associated death promotor protein; Grb2: Growth factor receptor-bound protein 2; MAPK: Mitogen-activated protein kinase; MEK: Mitogen-activated protein kinase kinase 1; NF-κB: Nuclear factor κB; PI3K: Phospohoinositide 3-kinase; PKC: Protein kinase C; PLC-γ: Phospholipase C gamma 1; SOS: Son of sevenless; mTOR: Mammalian target of rapamycin; RAS: Rat sarcoma viral oncogene; RAF: Rapidly accelerated fibrosarcoma.
The importance of addressing HER as a therapeutic target is underscored by many molecular and pathological findings. Amplified HER2 relates to carcinogenetic processes and adverse pathological features such as tumour size, invasion and metastatic spread; far more HER2 gene is expressed in cancer cells than in non-malignant adult cells[21]. The HER2 protein is overexpressed in breast, lung, salivary gland, ovarian, colon, prostate and pancreatic cancers[22,23]. Although HER2 is not associated with an adverse prognosis of gastric cancer to the extent that it is in breast cancer, inhibition of the HER2 pathway in patients with tumours overexpressing HER2 has conferred clinical benefits.
The expression of HER2 in gastric cancer is primarily detected using immunohistochemistry (ICH) and in situ hybridization (ISH). The basolateral membrane typically immunostains for HER2 in gastric cancer and less so on the luminal aspect of the cells, conferring a U-shaped appearance to the staining, whereas complete membrane staining is the rule for high scores in breast cancer. Another difference is the heterogeneity of immunostaining, which is rare in breast, but frequent in gastric tumours. The ICH should be used as the primary test; patients with scores of 3+ would be candidates for HER2 directed therapy, those with 2+ should be re-tested using ISH, and ISH-positive patients would be eligible for trastuzumab with chemotherapy[24]. HER2 is becoming regarded more and more as an important biomarker and cause of gastric cancer, as it is mainly amplified or overexpressed in 7%-34% of intestinal as well as GEJ and proximal tumours[21,25,26].
Trastuzumab is a fully humanized monoclonal antibody that binds to the extracellular domain of the receptor, and it acts by blocking HER2 receptor cleavage, thus inhibiting dimerization, inducing antibody-dependent cellular cytotoxicity, and increasing endocytosis of the receptor, possibly through anti-angiogenic effects[27-29].
The phase III multicentre, international ToGA trial that proceeded in 24 countries constitutes a milestone, as it established trastuzumab as the first biological therapy to confer survival benefits upon patients with gastric cancer[30-32]. The trial compared the effects of trastuzumab combined with standard chemotherapy (cisplatin + either capecitabine or 5-FU) upon inoperable locally advanced, recurrent or metastatic HER2-positive gastric cancer as a first-line therapy with those of chemotherapy alone. Patients were treated with six cycles of chemotherapy in both treatment arms, with patients in the experimental arm continuing treatment with trastuzumab until disease progressed. Cisplatin (80 mg/m2) was intravenously infused on day 1. Capecitabine (1000 mg/m2) was orally administered twice daily for 2 wk followed by a 1-wk rest or a continuous infusion of 5-FU (800 mg/m2 per day) on days 1-5 of each cycle. Trastuzumab was intravenously administered at a loading dose of 8 mg/kg on day 1 of the first cycle, followed by 6 mg/kg thereafter.
The primary objective of the study was to compare OS in both arms, and the secondary objectives were to compare progression-free survival (PFS), time to progression, overall response rates, disease control, duration of response and quality of life between the two treatment arms. Among 3665 tumour tissue specimens screened for HER2 positivity, 22% were HER2-positive (intestinal, diffuse and mixed types: 34%, 6% and 20%, respectively). Specimens were scored using IHC and fluorescence ISH (FISH) as 3+ (candidates for HER2-directed therapy) or 2+ (specimens should be re-examined using ISH; ISH-positive tumours were eligible for trastuzumab with chemotherapy). The rate was highest in 34% of GEJ and in 20% of gastric cancer samples[33], findings that agreed with those of other studies in which positivity rates were between 24% and 35% and between 9.5% and 21%, respectively[21,25,34-36].
The combination of trastuzumab with chemotherapy led to a significantly better median OS compared with the same chemo-therapeutic regimen alone in patients with advanced HER2-positive cancers (13.8 mo vs 11.1 mo). This effect was evident in patients with intestinal, but not diffuse-type gastric cancer[32,37]. Trastuzumab also improved the median PFS (6.7 mo vs 5.5 mo) and the radiological response rate (47% vs 35%) (Table 1). A sub-analysis of these ToGA data that excluded patients with IHC 0-1+ FISH+ tumours found a main gain in median survival of 4.2 mo, which was comparable to the outcomes for breast cancer[38]. In fact, patients with the highest levels of HER2 expression (IHC 3+ FISH+) treated with trastuzumab plus chemotherapy gained the greatest benefit compared with chemotherapy alone (median survival: 17.9 mo vs 12.3 mo). These findings have established platinum-based chemotherapy plus trastuzumab as a standard treatment for HER2-positive gastric cancer.
Table 1.
Clinical trial of trastuzumab
| Patients | Phase | Treatment | n | OS (m) | PFS (m) | RR |
| Advanced HER-positive gastric cancer as first line (TOGA) | III | 5-FU + cisplatin or capecitabine + cisplatin | 290 | 11.1 | 5.5 | 34.5% |
| 5-FU + cisplatin + trastuzumab or capecitabine + cisplatin + trastuzumab | 294 | 13.8 | 6.7 | 47.3% |
OS: Overall survival; PFS: Progression-free-survival; RR: Response rate; 5-FU: 5-fluorouracil.
In contrast, the S-1 plus CDDP (SP) regimen is a standard treatment for advanced gastric cancer in Japan[39,40]. Despite several studies of HER2-positive gastric cancer, the effects of SP in patients with different HER2 status remain unknown. Therefore, Honma et al[41] retrospectively compared the effects of the SP regimen between HER2- positive and negative types of gastric cancer. They could not conclude whether HER2 status influenced the survival of patients who received SP as a first-line chemotherapy. However, their report was the first to describe the effect of SP in HER2-positive, advanced gastric cancer. Their findings provide important historical data with which to interpret the outcomes of current worldwide phase II evaluations of the effects of SP combined with trastuzumab.
Trastuzumab is the only molecular targeting drug for treating gastric cancer that has been approved by large-scale phase III clinical trials associated with anti-cancer drugs. It is thought to have high therapeutic potential. Furthermore, HER2 has acquired a key role in gastric cancer management and it is also mandatory in order to predict the trastuzumab response in association with standard platinum-based chemotherapy.
SUNITINIB
Vascular endothelial growth factors (VEGF), platelet-derived growth factors (PDGF) and stem cell receptors (KIT) are expressed or overexpressed in gastric cancer. Indeed, these pathways appear to play important roles in gastric cancer growth and metastasis and they have therefore become targets for the development of cancer therapies.
Sunitinib malate (SUTENT; Pfizer Inc., New York, NY, United States) is an oral, multitargeted tyrosine kinase inhibitor of VEGF receptors (1, 2, and 3), PDGF receptors (α and β), KIT and several other related receptor tyrosine kinases[42-44]. Sunitinib has received multinational approval to treat unresectable and/or metastatic imatinib-resistant/intolerant gastrointestinal stromal tumours, advanced/metastatic renal cell carcinoma, and unresectable or metastatic well-differentiated pancreatic neuroendocrine tumours[45,46].
A Phase II study investigated the outcomes of sunitinib monotherapy in pre-treated patients with advanced gastric cancer. The patients were administered with sunitinib (50 mg/d) for 4 wk with a 2-wk rest until disease progressed or toxicity became unacceptable. In the intent-to-treat population (n = 51), the objective response rate (ORR) was 3.9%, median progression free survival (PFS) was 1.28 (95%CI: 1.18-1.90) mo, the median OS was 5.81 (95%CI: 12.8-36.5) mo and the estimated 1-year survival rate was 23.7% (95%CI: 12.8-36.5) (Table 2). Serious adverse events developed in 26 patients, leading to 13 deaths, none of which were related to sunitinib. Thirty-eight patients died of progressive disease and nine others died within 60 d of treatment. Sunitinib monotherapy thus appeared to be associated with a limited tumour response[47].
Table 2.
Clinical trials of sunitinib
| Patients | Phase | Treatment | n | OS (m) | PFS (m) | TTP (m) | RR | DCR |
| Pretreated patients with advanced gastric cancer | II | Sunitinib | 51 | 5.8 | 1.28 | N/A | 3.9% | 20.0% |
| Second line treatment for advanced gastric cancer | II | Sunitinib | 78 | 6.8 | 2.3 | 2.3 | 2.6% | 34.7% |
| Unresectable or metastatic advanced gastric cancer after failed treatment with fluoropyrimidine + platinum | II | Docetaxel | 49 | 6.6 | N/A | 2.6 | 14.3% | 51.0% |
| Docetaxel + sunitinib | 56 | 8.0 | N/A | 3.9 | 41.1% | 75.0% |
DCR: Disease control rate; N/A: Not available; OS: Overall survival; PFS: Progression-free-survival; RR: Response rate; TTP: Time to progression.
A Phase II study evaluated the safety and efficacy of sunitinib as a second-line treatment for advanced gastric in 78 patients. Two patients (2.6%) had partial responses and 25 (32.1%) had the best response of stable disease for ≥ 6 wk. The median PFS was 2.3 mo (95%CI: 1.6-2.6) and median OS was 6.8 mo (95%CI: 4.4-9.6) (Table 2). Grade ≥ 3 thrombocytopenia and neutropenia were identified in 34.6% and 29.4% of patients, respectively, and the most common non-haematological adverse effects were fatigue, anorexia, nausea, diarrhoea and stomatitis. Although sunitinib alone has insufficient clinical value as a second-line treatment for advanced gastric cancer, its role in combination with chemotherapy merits further study[48].
A randomized phase II trial investigated the effects of docetaxel and sunitinib in patients with unresectable or metastatic gastric cancer who were previously treated with fluoropyridine and platinum. The patients were assigned to either a docetaxcel monotherapy arm (D: 60 mg/m2 every 3 wk) or a combination of docetaxel + sunitinib (DS: 37.5 mg/d). The time to progression (TTP) was not significantly prolonged in the DS arm compared with the D arm 3.9 (95%CI: 2.9-4.9) vs 2.6 (95%CI: 1.8-3.5) mo (P = 0.206). The hazard ratio for TTP was 0.77 (95%CI: 0.53-1.16). However, the ORR was significantly higher in the DS arm (41.1% vs 14.3%, P = 0.002) (Table 2). Patients in the DS arm more frequently experienced stomatitis, diarrhoea and hand-foot syndrome. The investigators concluded that adding sunitinib to docetaxel did not significantly prolong TTP, although it significantly increased the response[49].
These findings indicated an insufficient therapeutic effect of sunitinib.
BEVACIZUMAB
Studies of tumour angiogenesis have provided a foundation for radical developments in the management and treatment of human cancers. The most sensitive angiogenic factor is VEGF, which is expressed in cancer cells. Several clinical trials have confirmed that some clinical benefit can be derived by targeting the vascular VEGF/VEGF receptor pathway. Senger et al[50] initially described VEGF in 1983 as a vascular permeability factor, and Ferrara and Henzel in 1989[51] later cloned the factor and found homology with VEGF. Among its many actions, VEGF enhances the permeability of tumour vessels[52], induces serine protease or metalloproteases[53,54], inhibits apoptosis in endothelial cells[55,56], and inhibits dendritic cell maturation[57]. Several randomized trials have shown that various VEGF-targeted agents confer clinical benefits upon patients with metastatic colorectal cancer, advanced non-small cell lung cancer, renal cell carcinoma, hepatocellular carcinoma and metastatic breast cancer[58]. Therapy targeting VEGF has thus become an important treatment option for several human malignancies.
The tumour/normal ratio of VEGF mRNA in gastric cancer tends to correlate with distant metastasis[59] and the positive expression of tissue VEGF, circulating VEGF, VEGF-C and VEGF-D were each associated with poor prognosis for patients with resected gastric cancer[60]. We previously reported that tissue VEGF is a useful indicator of the peritoneal recurrence of gastric cancer[61]. Our immunohistochemical study of clinical specimens identified a significantly higher VEGF score among patients with peritoneal recurrence than those without, and that the VEGF score was a significant parameter of peritoneal recurrence, suggesting that VEGF correlates with peritoneal metastasis from gastric cancer and is thus a useful indicator of such recurrence[61]. Bevacizumab is a humanized monoclonal antibody against VEGF that was the first angiogenesis inhibitor to become commercially available. The United States Food and Drug Administration approved bevacizumab in combination with standard chemotherapy to treat metastatic colorectal cancer in 2004, non-small cell lung cancer in 2006, and breast cancer in 2008. Bevacizumab was approved in Japan in combination with anticancer drugs to treat unresectable advanced or metastatic colorectal cancer in 2007. We performed a pilot study using a nude mouse model of peritoneal metastasis to determine whether bevacizumab could suppress peritoneal dissemination from gastric cancer[62]. The results indicated a significantly lower volume of ascites, a lower mitotic index and significantly better survival rates in the treated, than in the non-treated group. We concluded that VEGF correlates with peritoneal metastasis from gastric cancer, and that bevacizumab could inhibit VEGF and thus suppress peritoneal dissemination from gastric cancer[62].
Shah et al[63] performed a phase II study of irinotecan, cisplatin and bevacizumab in 47 patients with metastatic or unresectable gastric and GEJ adenocarcinoma. At a median follow up of 12.2 mo, the median TTP was 8.3 mo. The ORR was 65% and the median survival was 12.3 mo in 34 patients with measurable disease. They concluded that TTP and OS are encouraging, with TTP being improved over historical controls by 75%[63] (Table 3).
Table 3.
Clinical trials of bevacizumab
| Patients | Phase | Treatment | n | OS (m) | PFS (m) | TTP (m) | RR |
| Metastatic or unresectable gastric and GEJ adenocarcinoma | II | Irinotecan + cisplatin + bevacizumab | 47 | 12.3 | N/A | 8.3 | 65% |
| Previously untreated metastatic gastroesophageal adenocarcinoma | II | Docetaxel + fluorouracil + bevacizumab | 44 | 16.8 | 12 | N/A | 67% |
| First-line treatment for advanced gastric cancer (AVAGASTA) | III | Capecitabine + cisplatin | 387 | 10.1 | 5.3 | 37.4 | N/A |
| 387 | 12.1 | 6.7 | 46 | N/A | |||
| First-line treatment for advanced gastric cancer (AVAGASTA) | III | Capecitabine + cisplatin + bevacizumab |
GFJ: Gastroesophageal junction; N/A: Not available; OS: Overall survival; PFS: Progression-free-survival; RR: Response rate; TTP: Time to progression.
Shah et al[64] performed a phase II study of a modified administration schedule of docetaxel, cisplatin and fluorouracil (mDCF) with bevacizumab in 44 eligible patients with cancer (gastric, n = 22; GEJ, n = 20; oesophageal, n = 2). The confirmed response rate was 67% in 39 patients with measurable disease. The 6-mo PFS was 79%, and the median PFS was 12 mo. At 26 mo of follow up, the median OS was 16.8 mo, and the 2-year survival rate was 37%. They found that the 6-mo PFS was 79%, which surpassed their defined endpoint, and the median and 2-year OS were 16.8 mo and 37%, respectively (Table 3).
AVAGASTA was a global, randomized, phase III trial that evaluated the outcomes of bevacizumab plus chemotherapy with capecitabine xeloda/cisplatin as a first-line treatment for patients with advanced gastric cancer. While the primary endpoint was not met (median overall survival HR = 0.87; P = 0.1002), PFS and overall response rates significantly improved and the safety profile for bevacizumab + chemotherapy was acceptable in these patients[65] (Table 3). However, a sub-analysis of the AVAGAST trial that evaluated the benefit of bevacizumab in advanced gastric cancer, found distinct differences in the outcomes according to disease subtype. Shah[66] reported that combining bevacizumab especially with chemotherapy appeared to improve outcomes for non-Asian patients with diffuse or distal gastric cancer.
A large-scale phase III trial found that bevacizumab was not effective against gastric cancer and this agent was not approved for this purpose. However, bevacizumab was effective against gastric cancer in some patients.
LAPATINIB
Lapatinib is a dual tyrosine kinase inhibitor (TKI) that acts on both EGFR and HER2, and exerts activity against trastuzumab-resistant advanced breast cancer. The data suggest that trastuzumab is not associated with cross-resistance and lapatinib restored trastuzumab sensitivity in preclinical models[38,67]. Wainberg et al[68] found that lapatinib inhibits the growth of HER2-amplified cell lines and HER2-positive tumours in xenograft models, induces cell cycle arrest and apoptosis, and synergistically acts with trastuzumab.
A phase II study of lapatinib as a first-line therapy in 47 patients with advanced gastric cancer showed modest single-agent activity, with a 12% response rate, 20% disease stabilization, a partial response in 7% of patients and a median OS of 5 mo, which was lower than that found with conventional cytotoxic chemotherapy[69]. Another phase II study of lapatinib monotherapy in patients with GEJ overexpressing HER2 or oesophageal cancer reported limited single-agent activity, with no objective responses and stable disease in 8% of patients[70]. Lapatinib in conjunction with capecitabine as a first line treatment in the HER2-positive metastatic gastric cancer setting has been addressed in a multicentre phase II trial. The response and stable disease rates were 22% and 45%, respectively[71]. Another phase II trial found a partial response of 24% and stable disease in 34% of patients treated with lapatinib + capecitabine. The most frequent grade 3 and 4 side effects were anorexia, hand-foot syndrome, anemia and nausea and cardiotoxicity, none of which was significant[72]. Two phase III studies are currently evaluating the outcomes of lapatinib combined with chemotherapy in advanced oesophagogastric cancer: the LOGIC trial[73,74] has combined lapatinib with oxaliplatin and capecitabine as a first-line treatment and the TYTAN trial[75,76] has combined lapatinib with weekly paclitaxel in a second-line setting. The OS results should be available from the LOGIC trial in 2014. TYTAN is the first randomized trial to compare the outcomes and safety of adding lapatinib to weekly paclitaxel as a second-line treatment for HER2-positive advanced gastric cancer. The TYTAN study includes 430 patients with advanced gastric cancer who had progressed after first-line therapy with fluoropyrimidine and/or cisplatin and had HER2 amplification detected by FISH. The median OS of lapatinib + paclitaxel and of paclitaxel alone were 11.0 and 8.9 mo, respectively (NS; HR = 0.48; P = 0.2088), whereas those in a HER2 IHC3+ subgroup were 14.0 and 7.6 mo, respectively (HR = 0.59; P = 0.0176). The PFS (5.6 mo vs 4.2 mo; HR = 0.54; P = 0.0101) and the objective response rate (27% vs 9%) were also noticeably better with, than without lapatinib among patients in the IHC 3+ subgroup[75,76] (Table 4).
Table 4.
Clinical trial of lapatinib
| Patients | Phase | Treatment | n | OS (m) | PFS (m) | RR |
| Second-line treatment for HER2+ advanced gastric cancer (TYTAN) | III | Paclitaxel | 129 | 8.9 | 4.2 | 9% |
| Paclitaxel + lapatinib | 132 | 11.0 | 5.2 | 27% |
OS: Overall survival; PFS: Progression-free-survival; RR: Response rate; HER2: Human epidermal growth factor receptor 2.
The TYTAN trial found that lapatinib was not effective against gastric cancer and this agent was not approved for this purpose. However, lapatinib might be effective against HER2 IHC3+ gastric cancer.
EVEROLIMUS
Inhibition of the mammalian target of rapamycin (mTOR) pathway represents a new therapeutic target in the treatment of various human cancers. The key protein kinase that regulates cell growth and proliferation, cellular metabolism and angiogenesis, mTOR, is mainly activated via the PI3 kinase pathway through Akt/PKB and tuberous sclerosis complex[77]. Mutations in these components or in PTEN, a negative regulator of PI3 kinase, results in inappropriate mTOR activation[77]. The mTOR pathway is frequently dysregulated in various human cancers, including gastric cancer[78]. Oncogenic transformation maintained by a dysregulated mTOR pathway might sensitize tumour cells to mTOR inhibitors[77]. The mTOR downstream effectors, eIF4E and 4E binding protein 1 (4E-BP1) are overexpressed in GI cancer cells[77]. Everolimus reduced 4E-BP1 phosphorylation and attenuated the production of the proangiogenic factors, hypoxia-inducible factor 1α (HIF-1α) and VEGF in these gastric cancer cell lines[78]. Everolimus is an orally bioavailable mTOR inhibitor that binds with high affinity to its intracellular receptor FKBP12[79].
Preclinical studies[77,78,80] and a phase I study[81] have shown that everolimus has antitumour activity against advanced gastric cancer. A multicentre phase II study has assessed the effects of everolimus in patients with previously treated metastatic gastric cancer in Japan[82]. Patients with advanced gastric cancer that progressed despite prior chemotherapy received oral everolimus (10 mg/d) until disease progressed or the study was discontinued. Fifty-three patients were assessable. Although a complete or partial response was not obtained, a central review found that the size of the tumour had decreased from baseline in 45% of patients. The disease control rate (DCR) was 56.0% and the median PFS was 2.7 mo. At a median follow-up of 9.6 mo, the median OS was 10.1 mo (Table 5). Thus, everolimus monotherapy appeared to result in a promising DCR for patients with previously treated advanced gastric cancer[82].
Table 5.
Clinical trials of everolimus
| Patients | Phase | Treatment | n | OS (mo) | PFS (mo) | RR | DCR |
| Previously treated metastatic gastric cancer | II | Everolimus | 53 | 10.1 | 2.7 | 0% | 54.7% |
| Second-line treatment for advanced gastric cancer (GRANITE-1) | III | Placebo | 217 | 4.34 | 1.41 | 2.1% | N/A |
| Everolimus | 439 | 5.39 | 1.68 | 4.5% | N/A |
DCR: Disease control rate; N/A: Not available; OS: Overall survival; PFS: Progression-free-survival; RR: Response rate; TTP: Time to progression.
Eric Van Cutsem[83] presented phase III results from the GRANITE-1 trial of everolimus monotherapy as a second-line treatment for advanced gastric cancer at the ASCO GI 2012 Cancer Symposium. The study enrolled 656 patients in 23 countries between July 2009 and December 2010. Among them, 439 were randomly assigned to receive everolimus 10 mg/d and 217 received a placebo. Roughly 75% of the patients were male, 53.3% were Asian, 47.7% had undergone one previous line of chemotherapy and 50.6% had undergone gastrectomy. The drug failed to meet the primary endpoint of improved OS. The median OS with everolimus vs placebo was 5.39 mo vs 4.34 mo (HR = 0.90; 95%CI: 0.75-1.08; P = 0.1244). However, the median PFS was 1.68 mo vs 1.41 mo (HR = 0.66; 95%CI: 0.56-0.78, P < 0.0001). The estimated 6-mo PFS were 12.0% and 4.3% in the experimental and placebo groups, respectively (Table 5).
Everolimus extended the 6-mo PFS and improved patient responses. The ORR of the everolimus vs the placebo group was 4.5% (95%CI: 2.6%-7.1%) vs 2.1% (95%CI: 0.6%-5.3%) (Table 5).
These findings suggested that everolimus has no meaningful activity as a single agent in patients with advanced gastric cancer. Given the evident improvement in PFS, everolimus might be valuable when combined with other biological or chemotherapeutic agents. Future studies should investigate this concept as a first-line therapy[83].
RAMUCIRUMAB
Tumour growth and metastasis are closely linked to angiogenesis in most human tumours and VEGF is the most potent and specific angiogenic factor known to date. The VEGF family includes VEGF-A, -B, -C, -D, and -E, and placenta growth factor (PGF). VEGF-A binds to VEGF receptors 1 and 2, whereas VEGF-B and PGF bind to VEGF receptor (VEGFR)-1, and VEGF-C and -D bind to VEGFR-2 and -3. Activation of these receptors stimulates a signaling cascade that results in endothelial mitogenesis and migration, the induction of proteinases, extracellular matrix remodeling, increased vascular permeability, and the maintained survival of blood vessels formed de novo[84] (Figure 2).
Figure 2.
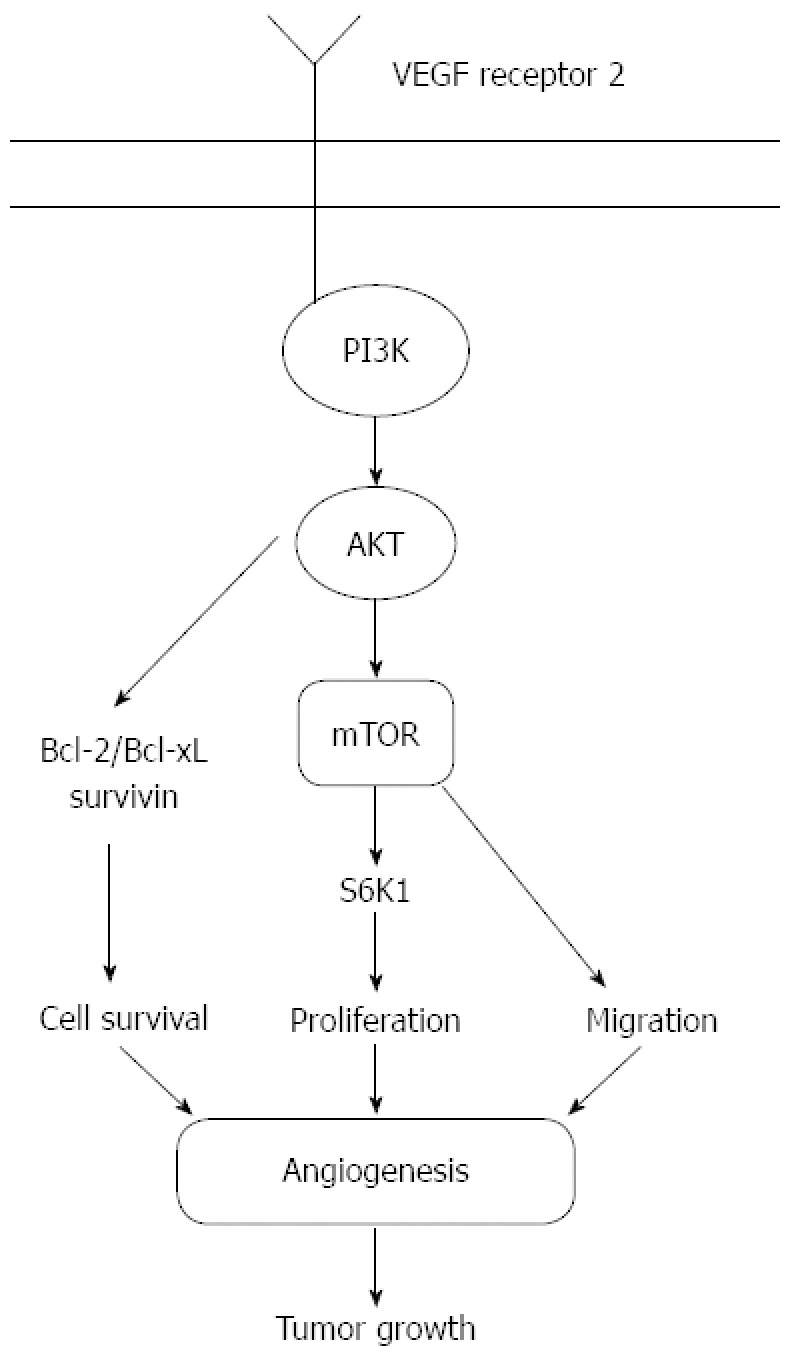
Angiogenic signaling pathways. AKT: Protein kinase B.
Ramucirumab is a fully humanized IgG1 monoclonal antibody that targets the extracellular domain of VEGFR-2[85,86]. Phase I-II trials in patients with various malignancies have shown promising clinical antitumour effects and tolerability[87].
At the 2013 ASCO GI Cancer Symposium, Charles S. Fuchs presented the phase III clinical REGARD trial that was the largest phase III trial of ramucirumab as a second-line therapy for advanced gastric or GEJ adenocarcinoma[88]. This global, randomized, double-blind trial of 355 patients with disease progression during first-line platinum- or combination therapy containing fluoropyrimidine showed that adding ramucirumab provided the best supportive care (BSC) and significantly prolonged the median OS; the primary endpoint increased from 3.8 to 5.2 mo (P = 0.0473). This translated into a 22% reduction in the risk of death with ramucirumab. Bolstering the OS results, ramucirumab also significantly prolonged the median PFS from 1.3 to 2.1 mo when combined with BSC (HR = 0.483; P < 0.0001). Furthermore, ramucirumab plus BSC more than doubled the disease control rate compared with BSC alone (48.7% vs 23.1%; P < 0.0001) (Table 6). Patients appeared to tolerate the VEGFR-2 inhibitor fairly well. Most adverse events associated with treatment emerged at a similar frequency in both the ramucirumab and placebo arms[88]. The survival benefit attained by adding ramucirumab to BSC appeared comparable to that achieved by adding second-line cytotoxic chemotherapy to BSC, and the REGARD trial validated the role of VEGFR-2 signaling as an important therapeutic target of treating advanced gastric and GEJ adenocarcinoma[88].
Table 6.
Clinical trial of ramucirumab
| Patient | Phase | Treatment | n | OS (mo) | PFS (mo) | RR | DCR |
| Second-line treatment for advanced gastric cancer or GEJ adenocarcinoma (REGARD) | III | BSC | 117 | 3.8 | 1.3 | 2.6% | 23.1% |
| Ramucirumab | 238 | 5.2 | 2.1 | 3.4% | 48.7% |
BSC: Best supportive care; DCR: Disease control rate; GFJ: Gastroesophageal junction; OS: Overall survival; PFS: Progression-free-survival; RR: Response rate.
The results of the on-going phase III RAINBOW trial that compares second-line treatment between ramucirumab and paclitaxel might further increase the survival benefit.
Trastuzumab remains the only molecular targeting agent that is approved for treating gastric cancer. However, ramucirumab should soon receive approval as a molecular targeting therapeutic agent.
CETUXIMAB
The transmembrane glycoprotein EGFR belongs to the tyrosine kinase growth factor receptor superfamily and is an important target of cancer therapy. EGFR is expressed in many human normal tissues and is overexpressed in a variety of tumours[89]; for example, 18%-91% of primary gastric cancer tumours and/or metastases overexpress EGFR and this correlates with a poor prognosis[90-94]. Cetuximab is a monoclonal IgG antibody directed against EGFR that binds to the extracellular domain of EGFR in an inactive configuration and competes for receptor binding by occluding the ligand-binding region[95]. This antibody-receptor interaction prevents receptor dimerization and thus blocks ligand-induced EGFR tyrosine kinase activation. Cetuximab also induces EGFR internalization, downregulation and degradation. Antibody-dependent cytotoxicity might also contribute significantly to the anticancer activity of cetuximab (Figure 3). Cancer-cell proliferation (G1 phase arrest) is inhibited by cetuximab, thus provoking an immune system-mediated antitumour response, inducing VEGF as well as tumour-induced angiogenesis, and cancer cell invasion[95]. Cetuximab potentiates the antitumour activity of cytotoxic drugs and radiotherapy in preclinical and clinical tumour models[96] and when combined with irinotecan-based therapies, confers a benefit upon patients with metastatic colorectal cancer, particularly for those with KRAS wild-type tumours[97]. The encouraging preclinical and phase II data suggest a potential benefit of cetuximab especially in combination with conventional cytostatic therapy in patients with advanced gastroesophageal cancer[94,98,99]. Moreover, phase 2 studies of cetuximab plus various first-line chemotherapy regimens in patients with advanced gastric cancer have found manageable and predicted safety profiles with substantial activity (ORR: 41%-65%)[97,100-103].
Figure 3.
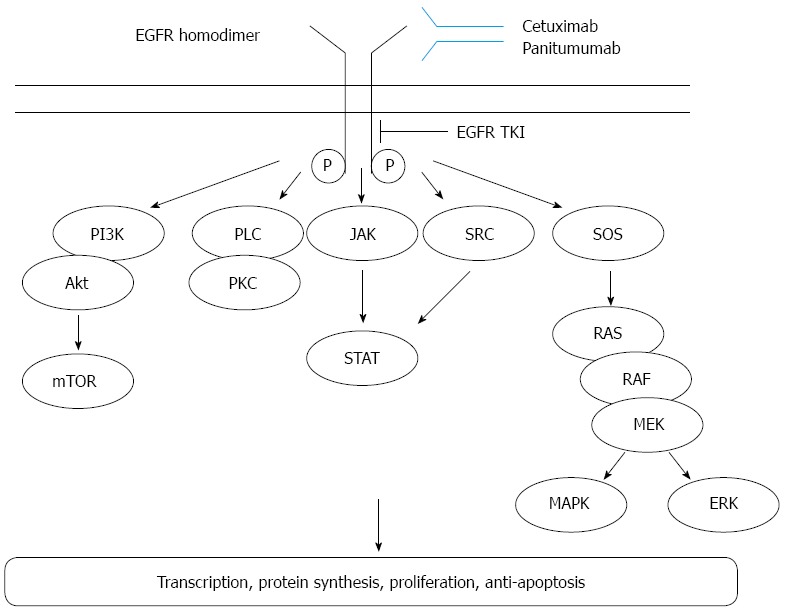
Epidermal growth factors signaling pathways. Activation of EGFR leads to downstream signaling pathways that ultimately drive tumour proliferation or impair apoptosis. JAK: Janus kinase; STAT: Signal transduction and activator of transcrption; ERK: Extracellular signal-regulated kinase; PI3K: Phospohoinositide 3-kinase; PKC: Protein kinase C; PLC: Phospholipase C; SOS: Son of sevenless; mTOR: Mammalian target of rapamycin; RAS: Rat sarcoma viral oncogene; RAF: Rapidly accelerated fibrosarcoma; EGFR: Epidermal growth factor receptor.
Lordick et al[103] described the randomized, open-label EXPAND phase 3 trial of capecitabine and cisplatin with or without cetuximab that included 908 adult patients aged ≥ 18 years with previously untreated and histologically confirmed locally advanced unresectable (M0) or metastatic (M1) adenocarcinoma of the stomach or GEJ. The study proceeded at teaching hospitals and clinics in 25 countries, and the participants were randomly assigned to groups that were eligible (1:1) to receive first-line chemotherapy with or without cetuximab. Treatment consisted of three-week cycles of capecitabine (1000 mg/m2) twice daily on days 1-14 and intravenous cisplatin (80 mg/m2) (on day 1), with or without weekly cetuximab (400 mg/m2 initial infusion on day 1 followed by 250 mg/m2 per week thereafter). The primary endpoint was PFS. The median PFS for 455 and 449 of the 908 patients allocated capecitabine-cisplatin with or without cetuximab were 4.4 (95%CI: 4.2-5.5) and 5.6 (95%CI: 5.1-5.7) mo, respectively (HR = 1.09; 95%CI: 0.92-1.29; P = 0.32) (Table 7). Lordick et al[103] concluded that combining cetuximab with capecitabine/cisplatin provided no additional benefit over chemotherapy alone as a first-line treatment for advanced gastric cancer.
Table 7.
Clinical trials of cetuximab and panitumumab
| Patients | Phase | Treatment | n | OS (m) | PFS (m) | RR | DCR |
| Previously untreated advanced gastric cancer (EXPAND) | III | Capecitabine + cisplatin | 449 | 10.7 | 5.6 | 29% | 71% |
| Capecitabine + cisplatin + cetuximab | 455 | 9.4 | 4.4 | 30% | 73% | ||
| Untreated metastatic or locally advanced oesophagogastric adenocarcinoma (REAL 3) | III | EOC (epirubicin + oxaliplatin + capecitabine) | 275 | 11.3 | 6.0 | 42% | 63% |
| Modified dose EOC + panitumumab | 278 | 8.8 | 7.4 | 46% | 64% |
DCR: Disease control rate; N/A: Not available; OS: Overall survival; PFS: Progression-free-survival; RR: Response rate.
The results of Phase III clinical trials did not find a sufficient therapeutic effect of cetuximab against gastric cancer.
PANITUMUMAB
Panitumumab is a fully human immunoglobulin G2 monoclonal antibody directed against the EGFR and it has conferred survival benefits for patients with advanced colorectal cancer[104].
The REAL2 non-inferiority study established epirubicin, oxaliplatin, and capecitabine (EOC) as a standard first-line regimen, and found a median OS of 11.2 mo[105]. This finding favorably compared with the alternative regimens assessed in REAL2, including a combination of epirubicin, cisplatin and fluorouracil that was associated with a median OS of 9.9 mo[105].
Waddell et al[106] reported a randomized open-label phase 3 trial of epirubicin, oxaliplatin and capecitabine with or without panitumumab that included 522 patients with previously untreated, metastatic or locally advanced oesophagogastric adenocarcinoma at 63 centres in the UK (REAL3). Eligible patients were randomly allocated (1:1) to receive up to eight 21-d cycles of open-label EOC [epirubicin (50 mg/m2) and oxaliplatin 130 mg/m2 on day 1 and capecitabine (1250 mg/m2 per day on days 1-21) or a modified dose of EOC plus panitumumab (mEOC+P: epirubicin, 50 mg/m2 and oxaliplatin 100 mg/m2 on day 1; capecitabine, 1000 mg/m2 per day on days 1-21 and panitumumab 9 mg/kg on day 1). The primary endpoint was OS in the intent-to-treat population. The median OS in 275 of the 533 patients who were allocated to receive EOC was 11.3 (95%CI: 9.6-13.0) vs 8.8 (95%CI: 7.7-9.8) mo and in 278 patients allocated to receive mEOC + P (HR = 1.37; 95%CI: 1.07-1.76; P = 0.013). Based on 333 events (EOC, n = 153; mEOC + P, n = 180), the effects of PFS did not differ between the treated groups (HR = 1.22; 95%CI, 0.98-1.52; P = 0.068). The median PFS in the mEOC + P and EOC groups were 6.0 (95%CI: 5.5-6.5) and 7.4 (95%CI: 6.3-8.5) mo, respectively (Table 7). Waddell et al[106] concluded that adding panitumumab to EOC chemotherapy does not increase OS and cannot be recommended for use in an unselected population with advanced oesophagogastric adenocarcinoma.
They listed three explanations for the poor outcome associated with mEOC + P in that trial[106]. Firstly, as previously reported[107], combining panitumumab with full-dose EOC during the initial stages of the trial was associated with unacceptably high rates of grade 3 diarrhoea. Therefore, the starting doses of oxaliplatin and capecitabine had to be reduced by 23% and 20%, respectively, in the experimental group.
Dose-intensity data also showed that a reduced proportion of patients in the experimental group achieved at least 80% of the planned capecitabine dose, suggesting that mEOC + P was still slightly more difficult to deliver than standard EOC. Panitumumab might have negatively interacted with one or more EOC components. Recent data derived from cell lines in vitro suggest that considerably more synergy might exist between anti-EGFR therapy and irinotecan than with oxaliplatin[108]. Furthermore, the results of adding cetuximab to treat colorectal cancer in the COIN trial suggested that the benefit derived from cetuximab might depend on the fluoropyrimidine partner, with patients receiving oxaliplatin plus fluorouracil perhaps deriving more benefit than those treated with oxaliplatin plus capecitabine[109]. At the time of their study, the significance of these potential interactions remained unknown, and they have not been assessed in the setting of oesophagogastric cancer.
Their findings might have been affected by assessing panitumumab therapy in a molecularly unselected population. Randomized clinical trials are therefore needed to establish whether targeting oncogenic signal transduction pathways such as KRAS, EGFR, HER2 and MET results in meaningful improvement.
The EXPAND trial that assessed the addition of cetuximab to a cisplatin-capecitabine doublet in 904 patients with previously untreated adenocarcinoma of the stomach and GEJ did not meet its primary endpoint of improved PFS[103]. The COG trial compared the anti-EGFR tyrosine-kinase inhibitor gefitinib with a placebo in the second-line treatment of 450 patients with oesophageal and type I-II GEJ cancers. This trial also did not meet its primary endpoint, as OS did not improve[110]. Adding panitumumab to EOC chemotherapy (REAL3 trial) also did not increase the OS.
These relatively consistent overall findings suggest that the EGFR pathway probably does not represent an important therapeutic target for most patients with oesophagogastric cancer.
OTHER MOLECULAR TARGETING THERAPIES
Matuzumab is a fully humanized EGFR-targeting monoclonal antibody. Rao et al[111] compared matuzumab plus epirubicin, cisplatin and capecitabine (ECX) with epirubicin, cisplatin and capecitabine alone as a first-line treatment for patients with advanced oesophagogastric (OG) cancer in a randomized, multicentre open-label phase II study. They concluded that matuzumab combined with ECX chemotherapy does not increase the response or survival of patients with OG cancer. Therefore, ECX/matuzumab should not be further assessed in phase III trials.
Recently, Trarbach et al[112] described a phase I study of matuzumab combined with 5-fluororouracil, leucovorin and cisplatin (PLF) in patients with advanced gastric and oesophagogastric adenocarcinomas. They concluded that the safety profile of matuzumab combined with PLF was acceptable and that it had modest anti-tumour activity.
Both c-Met and its ligand, hepatocyte growth factor (HGF), play important roles in oncogenesis. Aberrant activation of the HGF/c-Met signaling pathway might lead to increased tumour cell proliferation, resistance to apoptosis, invasive growth and tumour angiogenesis[113]. Low molecular-weight tivantinib (also known as ARQ 197) is the first in class, orally available, selective c-Met inhibitor[114].
Kang et al[115] described a phase II trial of tivantinib monotherapy as a second- or third-line therapy in patients with metastatic gastric cancer. They concluded that monotherapy with tivantinib was modestly effective against previously treated metastatic gastric cancer, and further studies of metastatic gastric cancer that take into account predictive biomarkers and/or combinations with other chemotherapies might be needed.
Signal transducer and activator of transcription 3 (STAT 3) is a transcription factor that is activated in response to growth factors and cytokines, and it contributes to the regulation of cell proliferation, apoptosis, and motility in many types of human tumours including gastric cancer[116]. Chronic STAT 3 activation is a key event in the induction and progression of gastric cancer. Therefore, STAT 3 deregulation during the initiation and progression of gastric cancer might serve as a new therapeutic strategy to hinder the development of gastric cancer[117].
CONCLUSION
So far, trastuzumab is the only molecular targeting therapy that has been approved for treating gastric cancer. The significance of molecular targeting therapy for gastric cancer remains controversial, but large-scale randomized clinical trials might confirm the benefits of other novel molecular targeting therapies for gastric cancer in the near future.
Footnotes
P- Reviewer: Feo F, Fujiwara T S- Editor: Ma YJ L- Editor: A E- Editor: Ma S
References
- 1.Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–2150. doi: 10.1200/JCO.2005.05.2308. [DOI] [PubMed] [Google Scholar]
- 2.Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from major cancers in the European Union, including acceding countries, in 2004. Cancer. 2004;101:2843–2850. doi: 10.1002/cncr.20666. [DOI] [PubMed] [Google Scholar]
- 3.Kelley JR, Duggan JM. Gastric cancer epidemiology and risk factors. J Clin Epidemiol. 2003;56:1–9. doi: 10.1016/s0895-4356(02)00534-6. [DOI] [PubMed] [Google Scholar]
- 4.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 5.Bosetti C, Bertuccio P, Levi F, Lucchini F, Negri E, La Vecchia C. Cancer mortality in the European Union, 1970-2003, with a joinpoint analysis. Ann Oncol. 2008;19:631–640. doi: 10.1093/annonc/mdm597. [DOI] [PubMed] [Google Scholar]
- 6.Malvezzi M, Bosetti C, Negri E, La Vecchia C, Decarli A. Cancer mortality in Italy, 1970-2002. Tumori. 2008;94:640–657. doi: 10.1177/030089160809400502. [DOI] [PubMed] [Google Scholar]
- 7.Maehara Y. S-1 in gastric cancer: a comprehensive review. Gastric Cancer. 2003;6 Suppl 1:2–8. doi: 10.1007/s10120-003-0232-9. [DOI] [PubMed] [Google Scholar]
- 8.Sakuramoto S, Sasako M, Yamaguchi T, Kinoshita T, Fujii M, Nashimoto A, Furukawa H, Nakajima T, Ohashi Y, Imamura H, et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med. 2007;357:1810–1820. doi: 10.1056/NEJMoa072252. [DOI] [PubMed] [Google Scholar]
- 9.Emi Y, Yamamoto M, Takahashi I, Orita H, Kakeji Y, Kohnoe S, Maehara Y. Phase II study of weekly paclitaxel by one-hour infusion for advanced gastric cancer. Surg Today. 2008;38:1013–1020. doi: 10.1007/s00595-008-3769-8. [DOI] [PubMed] [Google Scholar]
- 10.Nishiyama M, Wada S. Docetaxel: its role in current and future treatments for advanced gastric cancer. Gastric Cancer. 2009;12:132–141. doi: 10.1007/s10120-009-0521-z. [DOI] [PubMed] [Google Scholar]
- 11.Van Cutsem E, Haller D, Ohtsu A. The role of chemotherapy in the current treatment of gastric cancer. Gastric Cancer. 2002;5 Suppl 1:17–22. doi: 10.1007/s10120-002-0219-y. [DOI] [PubMed] [Google Scholar]
- 12.Koizumi W, Narahara H, Hara T, Takagane A, Akiya T, Takagi M, Miyashita K, Nishizaki T, Kobayashi O, Takiyama W, et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): a phase III trial. Lancet Oncol. 2008;9:215–221. doi: 10.1016/S1470-2045(08)70035-4. [DOI] [PubMed] [Google Scholar]
- 13.Nashimoto A, Yabusaki H, Nakagawa S, Takii Y, Tsuchiya Y, Otsuo T. Preoperative chemotherapy with S-1 and cisplatin for highly advanced gastric cancer. Anticancer Res. 2009;29:4689–4696. [PubMed] [Google Scholar]
- 14.Lin SY, Makino K, Xia W, Matin A, Wen Y, Kwong KY, Bourguignon L, Hung MC. Nuclear localization of EGF receptor and its potential new role as a transcription factor. Nat Cell Biol. 2001;3:802–808. doi: 10.1038/ncb0901-802. [DOI] [PubMed] [Google Scholar]
- 15.Williams CC, Allison JG, Vidal GA, Burow ME, Beckman BS, Marrero L, Jones FE. The ERBB4/HER4 receptor tyrosine kinase regulates gene expression by functioning as a STAT5A nuclear chaperone. J Cell Biol. 2004;167:469–478. doi: 10.1083/jcb.200403155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tai W, Mahato R, Cheng K. The role of HER2 in cancer therapy and targeted drug delivery. J Control Release. 2010;146:264–275. doi: 10.1016/j.jconrel.2010.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rüschoff J, Dietel M, Baretton G, Arbogast S, Walch A, Monges G, Chenard MP, Penault-Llorca F, Nagelmeier I, Schlake W, et al. HER2 diagnostics in gastric cancer-guideline validation and development of standardized immunohistochemical testing. Virchows Arch. 2010;457:299–307. doi: 10.1007/s00428-010-0952-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Coussens L, Yang-Feng TL, Liao YC, Chen E, Gray A, McGrath J, Seeburg PH, Libermann TA, Schlessinger J, Francke U. Tyrosine kinase receptor with extensive homology to EGF receptor shares chromosomal location with neu oncogene. Science. 1985;230:1132–1139. doi: 10.1126/science.2999974. [DOI] [PubMed] [Google Scholar]
- 19.Akiyama T, Sudo C, Ogawara H, Toyoshima K, Yamamoto T. The product of the human c-erbB-2 gene: a 185-kilodalton glycoprotein with tyrosine kinase activity. Science. 1986;232:1644–1646. doi: 10.1126/science.3012781. [DOI] [PubMed] [Google Scholar]
- 20.Popescu NC, King CR, Kraus MH. Localization of the human erbB-2 gene on normal and rearranged chromosomes 17 to bands q12-21.32. Genomics. 1989;4:362–366. doi: 10.1016/0888-7543(89)90343-1. [DOI] [PubMed] [Google Scholar]
- 21.Tanner M, Hollmén M, Junttila TT, Kapanen AI, Tommola S, Soini Y, Helin H, Salo J, Joensuu H, Sihvo E, et al. Amplification of HER-2 in gastric carcinoma: association with Topoisomerase IIalpha gene amplification, intestinal type, poor prognosis and sensitivity to trastuzumab. Ann Oncol. 2005;16:273–278. doi: 10.1093/annonc/mdi064. [DOI] [PubMed] [Google Scholar]
- 22.Niehans GA, Singleton TP, Dykoski D, Kiang DT. Stability of HER-2/neu expression over time and at multiple metastatic sites. J Natl Cancer Inst. 1993;85:1230–1235. doi: 10.1093/jnci/85.15.1230. [DOI] [PubMed] [Google Scholar]
- 23.Yan SY, Hu Y, Fan JG, Tao GQ, Lu YM, Cai X, Yu BH, Du YQ. Clinicopathologic significance of HER-2/neu protein expression and gene amplification in gastric carcinoma. World J Gastroenterol. 2011;17:1501–1506. doi: 10.3748/wjg.v17.i11.1501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Albarello L, Pecciarini L, Doglioni C. HER2 testing in gastric cancer. Adv Anat Pathol. 2011;18:53–59. doi: 10.1097/PAP.0b013e3182026d72. [DOI] [PubMed] [Google Scholar]
- 25.Gravalos C, Jimeno A. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann Oncol. 2008;19:1523–1529. doi: 10.1093/annonc/mdn169. [DOI] [PubMed] [Google Scholar]
- 26.Bang Y, Chung H, Xu J, Lordick F, Sawaki A, Lipatov O, See C, Rueschoff J, Cutsem EV. Pathological features of advanced gastric cancer (GC): Relationship to human epidermal growth factor receptor 2 (HER2) positivity in the global screening programme of the ToGA trial. J Clin Oncol. 2009;27:4556. [Google Scholar]
- 27.Stoss O, Nagelmeier I, Zielinski D, Rüschoff J National Cancer Institute. The ToGA (Trastuzumab for GAstric Cancer) Trial: Importance from a Biomarker Perspective. 2010. pp. 52–53. Available from: http://www.dako.com.
- 28.Petit AM, Rak J, Hung MC, Rockwell P, Goldstein N, Fendly B, Kerbel RS. Neutralizing antibodies against epidermal growth factor and ErbB-2/neu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by tumor cells in vitro and in vivo: angiogenic implications for signal transduction therapy of solid tumors. Am J Pathol. 1997;151:1523–1530. [PMC free article] [PubMed] [Google Scholar]
- 29.Baselga J, Swain SM. Novel anticancer targets: revisiting ERBB2 and discovering ERBB3. Nat Rev Cancer. 2009;9:463–475. doi: 10.1038/nrc2656. [DOI] [PubMed] [Google Scholar]
- 30.Fujimoto-Ouchi K, Sekiguchi F, Yasuno H, Moriya Y, Mori K, Tanaka Y. Antitumor activity of trastuzumab in combination with chemotherapy in human gastric cancer xenograft models. Cancer Chemother Pharmacol. 2007;59:795–805. doi: 10.1007/s00280-006-0337-z. [DOI] [PubMed] [Google Scholar]
- 31.Matsui Y, Inomata M, Tojigamori M, Sonoda K, Shiraishi N, Kitano S. Suppression of tumor growth in human gastric cancer with HER2 overexpression by an anti-HER2 antibody in a murine model. Int J Oncol. 2005;27:681–685. [PubMed] [Google Scholar]
- 32.Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376:687–697. doi: 10.1016/S0140-6736(10)61121-X. [DOI] [PubMed] [Google Scholar]
- 33.De Vita F, Giuliani F, Silvestris N, Catalano G, Ciardiello F, Orditura M. Human epidermal growth factor receptor 2 (HER2) in gastric cancer: a new therapeutic target. Cancer Treat Rev. 2010;36 Suppl 3:S11–S15. doi: 10.1016/S0305-7372(10)70014-1. [DOI] [PubMed] [Google Scholar]
- 34.Moelans CB, van Diest PJ, Milne AN, Offerhaus GJ. Her-2/neu testing and therapy in gastroesophageal adenocarcinoma. Patholog Res Int. 2011;2011:674182. doi: 10.4061/2011/674182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hede K. Gastric cancer: trastuzumab trial results spur search for other targets. J Natl Cancer Inst. 2009;101:1306–1307. doi: 10.1093/jnci/djp341. [DOI] [PubMed] [Google Scholar]
- 36.Polkowski W, van Sandick JW, Offerhaus GJ, ten Kate FJ, Mulder J, Obertop H, van Lanschot JJ. Prognostic value of Laurén classification and c-erbB-2 oncogene overexpression in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol. 1999;6:290–297. doi: 10.1007/s10434-999-0290-2. [DOI] [PubMed] [Google Scholar]
- 37.Yamashita K, Sakuramoto S, Watanabe M. Genomic and epigenetic profiles of gastric cancer: potential diagnostic and therapeutic applications. Surg Today. 2011;41:24–38. doi: 10.1007/s00595-010-4370-5. [DOI] [PubMed] [Google Scholar]
- 38.Okines AF, Cunningham D. Trastuzumab in gastric cancer. Eur J Cancer. 2010;46:1949–1959. doi: 10.1016/j.ejca.2010.05.003. [DOI] [PubMed] [Google Scholar]
- 39.Boku N, Yamamoto S, Fukuda H, Shirao K, Doi T, Sawaki A, Koizumi W, Saito H, Yamaguchi K, Takiuchi H, et al. Fluorouracil versus combination of irinotecan plus cisplatin versus S-1 in metastatic gastric cancer: a randomised phase 3 study. Lancet Oncol. 2009;10:1063–1069. doi: 10.1016/S1470-2045(09)70259-1. [DOI] [PubMed] [Google Scholar]
- 40.Sano T, Aiko T. New Japanese classifications and treatment guidelines for gastric cancer: revision concepts and major revised points. Gastric Cancer. 2011;14:97–100. doi: 10.1007/s10120-011-0040-6. [DOI] [PubMed] [Google Scholar]
- 41.Honma Y, Shimada Y, Takashima A, Iwasa S, Kato K, Hamaguchi T, Yamada Y, Taniguchi H, Sekine S, Kushima R. Efficacy of S-1 plus cisplatin combination chemotherapy in patients with HER2-positive advanced gastric cancer. Int J Clin Oncol. 2013:Nov 12; Epub ahead of print. doi: 10.1007/s10147-013-0629-3. [DOI] [PubMed] [Google Scholar]
- 42.Abrams TJ, Lee LB, Murray LJ, Pryer NK, Cherrington JM. SU11248 inhibits KIT and platelet-derived growth factor receptor beta in preclinical models of human small cell lung cancer. Mol Cancer Ther. 2003;2:471–478. [PubMed] [Google Scholar]
- 43.Mendel DB, Laird AD, Xin X, Louie SG, Christensen JG, Li G, Schreck RE, Abrams TJ, Ngai TJ, Lee LB, et al. In vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and platelet-derived growth factor receptors: determination of a pharmacokinetic/pharmacodynamic relationship. Clin Cancer Res. 2003;9:327–337. [PubMed] [Google Scholar]
- 44.O'Farrell AM, Abrams TJ, Yuen HA, Ngai TJ, Louie SG, Yee KW, Wong LM, Hong W, Lee LB, Town A, et al. SU11248 is a novel FLT3 tyrosine kinase inhibitor with potent activity in vitro and in vivo. Blood. 2003;101:3597–3605. doi: 10.1182/blood-2002-07-2307. [DOI] [PubMed] [Google Scholar]
- 45.Demetri GD, van Oosterom AT, Garrett CR, Blackstein ME, Shah MH, Verweij J, McArthur G, Judson IR, Heinrich MC, Morgan JA, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368:1329–1338. doi: 10.1016/S0140-6736(06)69446-4. [DOI] [PubMed] [Google Scholar]
- 46.Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, Oudard S, Negrier S, Szczylik C, Kim ST, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–124. doi: 10.1056/NEJMoa065044. [DOI] [PubMed] [Google Scholar]
- 47.Moehler M, Mueller A, Hartmann JT, Ebert MP, Al-Batran SE, Reimer P, Weihrauch M, Lordick F, Trarbach T, Biesterfeld S, et al. An open-label, multicentre biomarker-oriented AIO phase II trial of sunitinib for patients with chemo-refractory advanced gastric cancer. Eur J Cancer. 2011;47:1511–1520. doi: 10.1016/j.ejca.2011.04.006. [DOI] [PubMed] [Google Scholar]
- 48.Bang YJ, Kang YK, Kang WK, Boku N, Chung HC, Chen JS, Doi T, Sun Y, Shen L, Qin S, et al. Phase II study of sunitinib as second-line treatment for advanced gastric cancer. Invest New Drugs. 2011;29:1449–1458. doi: 10.1007/s10637-010-9438-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yi JH, Lee J, Lee J, Park SH, Park JO, Yim DS, Park YS, Lim HY, Kang WK. Randomised phase II trial of docetaxel and sunitinib in patients with metastatic gastric cancer who were previously treated with fluoropyrimidine and platinum. Br J Cancer. 2012;106:1469–1474. doi: 10.1038/bjc.2012.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS, Dvorak HF. Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science. 1983;219:983–985. doi: 10.1126/science.6823562. [DOI] [PubMed] [Google Scholar]
- 51.Ferrara N, Henzel WJ. Pituitary follicular cells secrete a novel heparin-binding growth factor specific for vascular endothelial cells. Biochem Biophys Res Commun. 1989;161:851–858. doi: 10.1016/0006-291x(89)92678-8. [DOI] [PubMed] [Google Scholar]
- 52.Dvorak HF, Brown LF, Detmar M, Dvorak AM. Vascular permeability factor/vascular endothelial growth factor, microvascular hyperpermeability, and angiogenesis. Am J Pathol. 1995;146:1029–1039. [PMC free article] [PubMed] [Google Scholar]
- 53.Pepper MS, Ferrara N, Orci L, Montesano R. Vascular endothelial growth factor (VEGF) induces plasminogen activators and plasminogen activator inhibitor-1 in microvascular endothelial cells. Biochem Biophys Res Commun. 1991;181:902–906. doi: 10.1016/0006-291x(91)91276-i. [DOI] [PubMed] [Google Scholar]
- 54.Unemori EN, Ferrara N, Bauer EA, Amento EP. Vascular endothelial growth factor induces interstitial collagenase expression in human endothelial cells. J Cell Physiol. 1992;153:557–562. doi: 10.1002/jcp.1041530317. [DOI] [PubMed] [Google Scholar]
- 55.Shaheen RM, Davis DW, Liu W, Zebrowski BK, Wilson MR, Bucana CD, McConkey DJ, McMahon G, Ellis LM. Antiangiogenic therapy targeting the tyrosine kinase receptor for vascular endothelial growth factor receptor inhibits the growth of colon cancer liver metastasis and induces tumor and endothelial cell apoptosis. Cancer Res. 1999;59:5412–5416. [PubMed] [Google Scholar]
- 56.Gerber HP, McMurtrey A, Kowalski J, Yan M, Keyt BA, Dixit V, Ferrara N. Vascular endothelial growth factor regulates endothelial cell survival through the phosphatidylinositol 3’-kinase/Akt signal transduction pathway. Requirement for Flk-1/KDR activation. J Biol Chem. 1998;273:30336–30343. doi: 10.1074/jbc.273.46.30336. [DOI] [PubMed] [Google Scholar]
- 57.Lissoni P, Malugani F, Bonfanti A, Bucovec R, Secondino S, Brivio F, Ferrari-Bravo A, Ferrante R, Vigoré L, Rovelli F, et al. Abnormally enhanced blood concentrations of vascular endothelial growth factor (VEGF) in metastatic cancer patients and their relation to circulating dendritic cells, IL-12 and endothelin-1. J Biol Regul Homeost Agents. 2001;15:140–144. [PubMed] [Google Scholar]
- 58.Ellis LM, Hicklin DJ. Pathways mediating resistance to vascular endothelial growth factor-targeted therapy. Clin Cancer Res. 2008;14:6371–6375. doi: 10.1158/1078-0432.CCR-07-5287. [DOI] [PubMed] [Google Scholar]
- 59.Ryu KH, Shim KN, Jung SA, Yoo K, Joo YH, Lee JH. Significance of preoperative tissue levels of vascular-endothelial cadherin, liver-intestine cadherin and vascular endothelial growth factor in gastric cancer. Korean J Gastroenterol. 2012;60:229–241. doi: 10.4166/kjg.2012.60.4.229. [DOI] [PubMed] [Google Scholar]
- 60.Liu L, Ma XL, Xiao ZL, Li M, Cheng SH, Wei YQ. Prognostic value of vascular endothelial growth factor expression in resected gastric cancer. Asian Pac J Cancer Prev. 2012;13:3089–3097. doi: 10.7314/apjcp.2012.13.7.3089. [DOI] [PubMed] [Google Scholar]
- 61.Aoyagi K, Kouhuji K, Yano S, Miyagi M, Imaizumi T, Takeda J, Shirouzu K. VEGF significance in peritoneal recurrence from gastric cancer. Gastric Cancer. 2005;8:155–163. doi: 10.1007/s10120-005-0329-4. [DOI] [PubMed] [Google Scholar]
- 62.Aoyagi K, Kouhuji K, Miyagi M, Kizaki J, Isobe T, Hashimoto K, Shirouzu K. Molecular targeting therapy using bevacizumab for peritoneal metastasis from gastric cancer. World J Crit Care Med. 2013;2:48–55. doi: 10.5492/wjccm.v2.i4.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Shah MA, Ramanathan RK, Ilson DH, Levnor A, D’Adamo D, O’Reilly E, Tse A, Trocola R, Schwartz L, Capanu M, et al. Multicenter phase II study of irinotecan, cisplatin, and bevacizumab in patients with metastatic gastric or gastroesophageal junction adenocarcinoma. J Clin Oncol. 2006;24:5201–5206. doi: 10.1200/JCO.2006.08.0887. [DOI] [PubMed] [Google Scholar]
- 64.Shah MA, Jhawer M, Ilson DH, Lefkowitz RA, Robinson E, Capanu M, Kelsen DP. Phase II study of modified docetaxel, cisplatin, and fluorouracil with bevacizumab in patients with metastatic gastroesophageal adenocarcinoma. J Clin Oncol. 2011;29:868–874. doi: 10.1200/JCO.2010.32.0770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ohtsu A, Shah MA, Van Cutsem E, Rha SY, Sawaki A, Park SR, Lim HY, Yamada Y, Wu J, Langer B, et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a randomized, double-blind, placebo-controlled phase III study. J Clin Oncol. 2011;29:3968–3976. doi: 10.1200/JCO.2011.36.2236. [DOI] [PubMed] [Google Scholar]
- 66.Shah MA. Survival analysis by gastric cancer subtypes in AVAGAST phase III trial. In: Helwick C, editor. Proceedings of the 2012 Gastrointestinal Cancers Symposium: 19-21 January 2012; San Francisco. The ASCO post. 2012;3:6. [Google Scholar]
- 67.Ritter CA, Perez-Torres M, Rinehart C, Guix M, Dugger T, Engelman JA, Arteaga CL. Human breast cancer cells selected for resistance to trastuzumab in vivo overexpress epidermal growth factor receptor and ErbB ligands and remain dependent on the ErbB receptor network. Clin Cancer Res. 2007;13:4909–4919. doi: 10.1158/1078-0432.CCR-07-0701. [DOI] [PubMed] [Google Scholar]
- 68.Wainberg ZA, Anghel A, Desai AJ, Ayala R, Luo T, Safran B, Fejzo MS, Hecht JR, Slamon DJ, Finn RS. Lapatinib, a dual EGFR and HER2 kinase inhibitor, selectively inhibits HER2-amplified human gastric cancer cells and is synergistic with trastuzumab in vitro and in vivo. Clin Cancer Res. 2010;16:1509–1519. doi: 10.1158/1078-0432.CCR-09-1112. [DOI] [PubMed] [Google Scholar]
- 69.Iqbal S, Goldman B, Fenoglio-Preiser CM, Lenz HJ, Zhang W, Danenberg KD, Shibata SI, Blanke CD. Southwest Oncology Group study S0413: a phase II trial of lapatinib (GW572016) as first-line therapy in patients with advanced or metastatic gastric cancer. Ann Oncol. 2011;22:2610–2615. doi: 10.1093/annonc/mdr021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Luis M, Tavares A, Carvalho LS, Lara-Santos L, Araújo A, de Mello RA. Personalizing therapies for gastric cancer: molecular mechanisms and novel targeted therapies. World J Gastroenterol. 2013;19:6383–6397. doi: 10.3748/wjg.v19.i38.6383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Pishvaian M, Sakaeva D, Hsieh R. A global, multi-center phase II trial of lapatinib plus capecitabine in gastric cancer. J Clin Oncol. 2011;29 suppl 4:abstr 88. [Google Scholar]
- 72.Lenz H, Zhang J, Kemner AM, Kaneko T, Yang D, Franklin N, Iqbal S. Lapatinib capecitabine in advanced gastric cancer: An open-label phase II study of non ERBB2-targeted disease. Anall Oncol. 2010;21:S817. [Google Scholar]
- 73.GlaxoSmithKline LOGiC - Lapatinib Optimization Study in ErbB2 (HER2) Positive Gastric Cancer: A Phase III Global, Blinded Study Designed to Evaluate Clinical Endpoints and Safety of Chemotherapy Plus Lapatinib. 2008; Available from: http://clinicaltrials.gov/ct2/show/NCT00680901.
- 74.Hecht JR, Urba SG, Koehler M, Ellis C, Gagnon R, Kemner A. Lapatinib monotherapy in recurrent upper gastrointestinal malignancy: Phase II efficacy and biomarker analyses. Proceedings of the Gastrointestinal Cancers Symposium. ASCO GI. 2008:43a. [Google Scholar]
- 75.GlaxoSmithKline Lapatinib in Combination With Weekly Paclitaxel in Patients With ErB2 Amplified Advanced Gastric Cancer. 2007. Available from: http://clinicaltrials.gov/ct2/show/NCT00486954.
- 76.Satoh T, Bang Y, Wang J, Xu J, Chung HC, Yeh K, Chen J, Mukaiyama A, Yoshida P, Ohtsu A. Interim safety analysis from TYTAN: A phase III Asian study of lapatinib in combination with paclitaxel as second-line therapy in gastric cancer. J Clin Oncol. 2010;28:abstr4057. [Google Scholar]
- 77.Bjornsti MA, Houghton PJ. The TOR pathway: a target for cancer therapy. Nat Rev Cancer. 2004;4:335–348. doi: 10.1038/nrc1362. [DOI] [PubMed] [Google Scholar]
- 78.Martín ME, Pérez MI, Redondo C, Alvarez MI, Salinas M, Fando JL. 4E binding protein 1 expression is inversely correlated to the progression of gastrointestinal cancers. Int J Biochem Cell Biol. 2000;32:633–642. doi: 10.1016/s1357-2725(00)00007-8. [DOI] [PubMed] [Google Scholar]
- 79.Wan X, Helman LJ. The biology behind mTOR inhibition in sarcoma. Oncologist. 2007;12:1007–1018. doi: 10.1634/theoncologist.12-8-1007. [DOI] [PubMed] [Google Scholar]
- 80.Cejka D, Preusser M, Woehrer A, Sieghart W, Strommer S, Werzowa J, Fuereder T, Wacheck V. Everolimus (RAD001) and anti-angiogenic cyclophosphamide show long-term control of gastric cancer growth in vivo. Cancer Biol Ther. 2008;7:1377–1385. doi: 10.4161/cbt.7.9.6416. [DOI] [PubMed] [Google Scholar]
- 81.Okamoto I, Doi T, Ohtsu A, Miyazaki M, Tsuya A, Kurei K, Kobayashi K, Nakagawa K. Phase I clinical and pharmacokinetic study of RAD001 (everolimus) administered daily to Japanese patients with advanced solid tumors. Jpn J Clin Oncol. 2010;40:17–23. doi: 10.1093/jjco/hyp120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Doi T, Muro K, Boku N, Yamada Y, Nishina T, Takiuchi H, Komatsu Y, Hamamoto Y, Ohno N, Fujita Y, et al. Multicenter phase II study of everolimus in patients with previously treated metastatic gastric cancer. J Clin Oncol. 2010;28:1904–1910. doi: 10.1200/JCO.2009.26.2923. [DOI] [PubMed] [Google Scholar]
- 83.Van Cutsem E. Abtract LBA3. Presented at: ASCO Gastrointestinal Cancers Symposium; 19-21 January; 2012. p. San Francisco. [Google Scholar]
- 84.Youssoufian H, Hicklin DJ, Rowinsky EK. Review: monoclonal antibodies to the vascular endothelial growth factor receptor-2 in cancer therapy. Clin Cancer Res. 2007;13:5544s–5548s. doi: 10.1158/1078-0432.CCR-07-1107. [DOI] [PubMed] [Google Scholar]
- 85.Lu D, Shen J, Vil MD, Zhang H, Jimenez X, Bohlen P, Witte L, Zhu Z. Tailoring in vitro selection for a picomolar affinity human antibody directed against vascular endothelial growth factor receptor 2 for enhanced neutralizing activity. J Biol Chem. 2003;278:43496–43507. doi: 10.1074/jbc.M307742200. [DOI] [PubMed] [Google Scholar]
- 86.Zhu Z, Hattori K, Zhang H, Jimenez X, Ludwig DL, Dias S, Kussie P, Koo H, Kim HJ, Lu D, et al. Inhibition of human leukemia in an animal model with human antibodies directed against vascular endothelial growth factor receptor 2. Correlation between antibody affinity and biological activity. Leukemia. 2003;17:604–611. doi: 10.1038/sj.leu.2402831. [DOI] [PubMed] [Google Scholar]
- 87.Spratlin JL, Cohen RB, Eadens M, Gore L, Camidge DR, Diab S, Leong S, O’Bryant C, Chow LQ, Serkova NJ, et al. Phase I pharmacologic and biologic study of ramucirumab (IMC-1121B), a fully human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J Clin Oncol. 2010;28:780–787. doi: 10.1200/JCO.2009.23.7537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Fuchs CS, Tomasek J, Cho JY. REGARD: a phase III, randomized, double-blind trial of ramucirumab and best supportive care (BSC) versus placebo and BSC in the treatment of metastatic gastric or gastroesophageal junction (GEJ) adenocarcinoma following disease progression on first-line platinum- and/or fluoropyrimidine-containing combination therapy. J Clin Oncol. 2012;30 suppl 34:abstr LBA5. [Google Scholar]
- 89.Ciardiello F, Tortora G. A novel approach in the treatment of cancer: targeting the epidermal growth factor receptor. Clin Cancer Res. 2001;7:2958–2970. [PubMed] [Google Scholar]
- 90.Tokunaga A, Onda M, Okuda T, Teramoto T, Fujita I, Mizutani T, Kiyama T, Yoshiyuki T, Nishi K, Matsukura N. Clinical significance of epidermal growth factor (EGF), EGF receptor, and c-erbB-2 in human gastric cancer. Cancer. 1995;75:1418–1425. doi: 10.1002/1097-0142(19950315)75:6+<1418::aid-cncr2820751505>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 91.Albanell J, Rojo F, Baselga J. Pharmacodynamic studies with the epidermal growth factor receptor tyrosine kinase inhibitor ZD1839. Semin Oncol. 2001;28:56–66. doi: 10.1016/s0093-7754(01)90283-0. [DOI] [PubMed] [Google Scholar]
- 92.Mendelsohn J. Targeting the epidermal growth factor receptor for cancer therapy. J Clin Oncol. 2002;20:1S–13S. [PubMed] [Google Scholar]
- 93.Takehana T, Kunitomo K, Suzuki S, Kono K, Fujii H, Matsumoto Y, Ooi A. Expression of epidermal growth factor receptor in gastric carcinomas. Clin Gastroenterol Hepatol. 2003;1:438–445. doi: 10.1016/s1542-3565(03)00219-2. [DOI] [PubMed] [Google Scholar]
- 94.Pinto C, Di Fabio F, Siena S, Cascinu S, Rojas Llimpe FL, Ceccarelli C, Mutri V, Giannetta L, Giaquinta S, Funaioli C, et al. Phase II study of cetuximab in combination with FOLFIRI in patients with untreated advanced gastric or gastroesophageal junction adenocarcinoma (FOLCETUX study) Ann Oncol. 2007;18:510–517. doi: 10.1093/annonc/mdl459. [DOI] [PubMed] [Google Scholar]
- 95.Martinelli E, De Palma R, Orditura M, De Vita F, Ciardiello F. Anti-epidermal growth factor receptor monoclonal antibodies in cancer therapy. Clin Exp Immunol. 2009;158:1–9. doi: 10.1111/j.1365-2249.2009.03992.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Ciardiello F, Tortora G. EGFR antagonists in cancer treatment. N Engl J Med. 2008;358:1160–1174. doi: 10.1056/NEJMra0707704. [DOI] [PubMed] [Google Scholar]
- 97.Van Cutsem E, Köhne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, D’Haens G, Pintér T, Lim R, Bodoky G, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. doi: 10.1056/NEJMoa0805019. [DOI] [PubMed] [Google Scholar]
- 98.Pinto C, Di Fabio F, Barone C, Siena S, Falcone A, Cascinu S, Rojas Llimpe FL, Stella G, Schinzari G, Artale S, et al. Phase II study of cetuximab in combination with cisplatin and docetaxel in patients with untreated advanced gastric or gastro-oesophageal junction adenocarcinoma (DOCETUX study) Br J Cancer. 2009;101:1261–1268. doi: 10.1038/sj.bjc.6605319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Lordick F, Luber B, Lorenzen S, Hegewisch-Becker S, Folprecht G, Wöll E, Decker T, Endlicher E, Röthling N, Schuster T, et al. Cetuximab plus oxaliplatin/leucovorin/5-fluorouracil in first-line metastatic gastric cancer: a phase II study of the Arbeitsgemeinschaft Internistische Onkologie (AIO) Br J Cancer. 2010;102:500–505. doi: 10.1038/sj.bjc.6605521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Han SW, Oh DY, Im SA, Park SR, Lee KW, Song HS, Lee NS, Lee KH, Choi IS, Lee MH, et al. Phase II study and biomarker analysis of cetuximab combined with modified FOLFOX6 in advanced gastric cancer. Br J Cancer. 2009;100:298–304. doi: 10.1038/sj.bjc.6604861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Moehler M, Mueller A, Trarbach T, Lordick F, Seufferlein T, Kubicka S, Geissler M, Schwarz S, Galle PR, Kanzler S. Cetuximab with irinotecan, folinic acid and 5-fluorouracil as first-line treatment in advanced gastroesophageal cancer: a prospective multi-center biomarker-oriented phase II study. Ann Oncol. 2011;22:1358–1366. doi: 10.1093/annonc/mdq591. [DOI] [PubMed] [Google Scholar]
- 102.Kim C, Lee JL, Ryu MH, Chang HM, Kim TW, Lim HY, Kang HJ, Park YS, Ryoo BY, Kang YK. A prospective phase II study of cetuximab in combination with XELOX (capecitabine and oxaliplatin) in patients with metastatic and/or recurrent advanced gastric cancer. Invest New Drugs. 2011;29:366–373. doi: 10.1007/s10637-009-9363-0. [DOI] [PubMed] [Google Scholar]
- 103.Lordick F, Kang YK, Chung HC, Salman P, Oh SC, Bodoky G, Kurteva G, Volovat C, Moiseyenko VM, Gorbunova V, et al. Capecitabine and cisplatin with or without cetuximab for patients with previously untreated advanced gastric cancer (EXPAND): a randomised, open-label phase 3 trial. Lancet Oncol. 2013;14:490–499. doi: 10.1016/S1470-2045(13)70102-5. [DOI] [PubMed] [Google Scholar]
- 104.Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham D, Jassem J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol. 2010;28:4697–4705. doi: 10.1200/JCO.2009.27.4860. [DOI] [PubMed] [Google Scholar]
- 105.Cunningham D, Starling N, Rao S, Iveson T, Nicolson M, Coxon F, Middleton G, Daniel F, Oates J, Norman AR. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358:36–46. doi: 10.1056/NEJMoa073149. [DOI] [PubMed] [Google Scholar]
- 106.Waddell T, Chau I, Cunningham D, Gonzalez D, Okines AF, Okines C, Wotherspoon A, Saffery C, Middleton G, Wadsley J, et al. Epirubicin, oxaliplatin, and capecitabine with or without panitumumab for patients with previously untreated advanced oesophagogastric cancer (REAL3): a randomised, open-label phase 3 trial. Lancet Oncol. 2013;14:481–489. doi: 10.1016/S1470-2045(13)70096-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Okines AF, Ashley SE, Cunningham D, Oates J, Turner A, Webb J, Saffery C, Chua YJ, Chau I. Epirubicin, oxaliplatin, and capecitabine with or without panitumumab for advanced esophagogastric cancer: dose-finding study for the prospective multicenter, randomized, phase II/III REAL-3 trial. J Clin Oncol. 2010;28:3945–3950. doi: 10.1200/JCO.2010.29.2847. [DOI] [PubMed] [Google Scholar]
- 108.Vora N, Evans S, Bernard PJ, Francisco F, Nagourney RA. Optimal combination therapy for advanced colorectal cancer: an examination of synergy and antagonism with EGFR inhibition. Proc Am Soc Clin Oncol. 2012;30(suppl):abstr e14075. [Google Scholar]
- 109.Maughan TS, Adams RA, Smith CG, Meade AM, Seymour MT, Wilson RH, Idziaszczyk S, Harris R, Fisher D, Kenny SL, et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet. 2011;377:2103–2114. doi: 10.1016/S0140-6736(11)60613-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Ferry DR, Dutton SJ, Mansoor W. Phase III multi-centre, randomized, double-blind, placebo-controlled trials of gefitinib versus placebo in esophageal cancer progressing after chemotherapy, COG (cancer oesophagus gefitinib) Ann Oncol. 2012;23(suppl 9):ixe12. doi: 10.1016/S1470-2045(14)70024-5. [DOI] [PubMed] [Google Scholar]
- 111.Rao S, Starling N, Cunningham D, Sumpter K, Gilligan D, Ruhstaller T, Valladares-Ayerbes M, Wilke H, Archer C, Kurek R, et al. Matuzumab plus epirubicin, cisplatin and capecitabine (ECX) compared with epirubicin, cisplatin and capecitabine alone as first-line treatment in patients with advanced oesophago-gastric cancer: a randomised, multicentre open-label phase II study. Ann Oncol. 2010;21:2213–2219. doi: 10.1093/annonc/mdq247. [DOI] [PubMed] [Google Scholar]
- 112.Trarbach T, Przyborek M, Schleucher N, Heeger S, Lüpfert C, Vanhoefer U. Phase I study of matuzumab in combination with 5-fluorouracil, leucovorin and cisplatin (PLF) in patients with advanced gastric and esophagogastric adenocarcinomas. Invest New Drugs. 2013;31:642–652. doi: 10.1007/s10637-012-9848-0. [DOI] [PubMed] [Google Scholar]
- 113.Gherardi E, Birchmeier W, Birchmeier C, Vande Woude G. Targeting MET in cancer: rationale and progress. Nat Rev Cancer. 2012;12:89–103. doi: 10.1038/nrc3205. [DOI] [PubMed] [Google Scholar]
- 114.Munshi N, Jeay S, Li Y, Chen CR, France DS, Ashwell MA, Hill J, Moussa MM, Leggett DS, Li CJ. ARQ 197, a novel and selective inhibitor of the human c-Met receptor tyrosine kinase with antitumor activity. Mol Cancer Ther. 2010;9:1544–1553. doi: 10.1158/1535-7163.MCT-09-1173. [DOI] [PubMed] [Google Scholar]
- 115.Kang YK, Muro K, Ryu MH, Yasui H, Nishina T, Ryoo BY, Kamiya Y, Akinaga S, Boku N. A phase II trial of a selective c-Met inhibitor tivantinib (ARQ 197) monotherapy as a second- or third-line therapy in the patients with metastatic gastric cancer. Invest New Drugs. 2014;32:355–361. doi: 10.1007/s10637-013-0057-2. [DOI] [PubMed] [Google Scholar]
- 116.Okamoto W, Okamoto I, Arao T, Yanagihara K, Nishio K, Nakagawa K. Differential roles of STAT3 depending on the mechanism of STAT3 activation in gastric cancer cells. Br J Cancer. 2011;105:407–412. doi: 10.1038/bjc.2011.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Giraud AS, Menheniott TR, Judd LM. Targeting STAT3 in gastric cancer. Expert Opin Ther Targets. 2012;16:889–901. doi: 10.1517/14728222.2012.709238. [DOI] [PubMed] [Google Scholar]