

Abstract
The purpose of this study was to investigate canal configuration of mandibular first premolars in an Egyptian population. Two hundred fifty human extracted mandibular first premolars were collected from Egyptian patients and a small hole in the center of the occlusal surface of each tooth was made perforating the roof of the pulp chamber. Teeth were decalcified by immersing in nitric acid and dehydrated in ascending concentrations of ethyl alcohol. A waterproof black ink was passively injected from the occlusal hole into pulp system and stained teeth were immersed in methyl salicylate solution for clearing. Standardized pictures of the cleared teeth were obtained and anatomical features of the root canal were observed. The average length of the mandibular first premolar teeth was 22.48 ± 1.74 mm, one-rooted teeth were 96.8% and the two-rooted were 3.2%. Vertucci Type I canal configuration represented the highest percentage (61.2%) followed by Type V (16.4%), Type IV (13.2%), Type II (5.6%) and Type III (2.8%). Vertucci Type VI canal configuration represented the lowest percentage (0.4%) and a complex configuration was found in one tooth. Accessory canals were detected in 22.8% and inter-canal connections were observed in 24.8% while 54% showed apical delta. Such knowledge is clinically useful for localization and negotiation of canals of mandibular first premolar, as well as their subsequent management in Egyptian population.
Keywords: Egyptian population, Ethnic, Internal root anatomy, Mandibular first premolar
Introduction
Root canal’s configuration has its important significance in endodontics because the entire canal system must be adequately debrided and filled to achieve a healthy response following root canal treatment [1]. Therefore, clinicians must have an understanding of the complexity of the root canal system and its possible variations in order to achieve a technically satisfactory outcome [2]. False assumptions about root and canal configuration may lead to incomplete debridement and obturation with eventual endodontic failure [1].
Various methods have been used to study canal morphology including tooth sectioning, radiographs, post-treatment clinical observation, direct observation with microscope, tooth clearing, 3D reconstruction, and computed tomography [2]. Of these techniques, it has been reported that most detailed information can be obtained by in vitro staining and tooth clearing method which is considered to be the simplest and most convenient [1,3].
The interior of teeth has shown many anatomic variations and can be extremely complex [1–2]. Several studies reported different trends in shape and number of roots and their canals amongst the different races [4–5]. Other factors that may affect the findings of anatomical variations include gender [6], age [7] and the study design, either in vivo or in vitro [8]. Among the most frequently teeth requiring root canal treatment is the permanent mandibular first premolar that has a wide variety of root canal configurations caused by genetic and environmental influences and can be extremely complex [2]. Therefore, root canal morphology of the mandibular first premolars has been investigated based on the study of various population groups, including Mexican, [9] American [4,6,10–12], Chinese [13,14], Kuwait [15], France [16], Turkish, [7,17] Japanese [18,19], Indian [20–23], Jordanian [24], Seri-Lankan [19], Iranian [25] and Polish patients of Caucasian origin [26]. Published reports on the root canal anatomy of mandibular first premolars in Egyptian population could not be found in the literature. Therefore, the current study was conducted to investigate canal configuration of mandibular first premolars in an Egyptian population.
Material and methods
Human 250 extracted mandibular first premolars were collected from Egyptian patients. The age and gender for each individual patient was not recorded during teeth collection. Teeth with incompletely formed roots, carious cavities, cracks, fracture, resorption, calcifications, metallic restorations, or previous root canal interference were not included in the study. Coronal morphological features were considered to identify and confirm that all the studied teeth were mandibular first premolars and the study was performed in accordance with the study guide of the American Association of Endodontics [27].
The collected teeth were cleaned out of any bone fragments, calculus or remaining external soft tissues using an ultrasonic scalar (Sirona, Bensheim, Germany) and the teeth were then stored in a 10% formalin solution until processing. Tooth length was measured using a digital measuring micrometer (Mitutoyo™, Kawasaki, Japan). The length of the teeth was measured from the tip of the buccal cusp to the apex of the root. In case of a curved root, tangents were drawn to the curved portions of the tooth and the length was then measured by connecting the points of tangency.
A small hole in the center of the occlusal surface of each tooth that extended to the roof of the pulp chamber was made using a fine tapered diamond fissure bur in a high speed hand piece with water spray. Teeth were then immersed in 5.25% sodium hypochlorite for 4 h, rinsed under running water for 2 h and bench-dried overnight.
Teeth were decalcified by immersing in nitric acid (10% for 3 days followed by 5% for 2 days). Decalcified teeth were rinsed thoroughly, stored in water overnight and bench-dried for 3 h. The teeth were then dehydrated in ascending concentrations of ethyl alcohol (70%, 95% and 100%) for 12 h each [3]. Complete decalcification was determined by radiographs for random samples to check for a uniform decalcification of the tooth. Once the dehydration process was completed, teeth were allowed to bench-dry for 2 h.
A waterproof black ink (Sanford Rotring GmbH, Hamburg, Germany) was passively injected from the occlusal hole into the pulp chamber and root canal system using a fine insulin needle until the ink was seen out through the apical foramen. Excess ink was wiped out with gauze soaked in alcohol. To obtain transparent teeth, the dried dehydrated stained teeth were immersed in methyl salicylate solution (98%) into which the teeth were stored until they were examined not more than 10 days.
Standardized pictures were obtained, by digital camera (ScopeTek ScopePhoto 3.0, Hangzhou ScopeTek opto-Electric Co., Ltd, China), for the proximal surfaces of the transparent teeth with a fixed distance (10 cm) and zoom (x2.5). Anatomical features of the root canal was observed and classified according to Vertucci’s classification (Vertucci 1984). The observed criteria included root canals number and configuration, the presence of accessory canals or inter-canal communications, and number of apical foramina. The recorded data were collected, tabulated and analyzed for descriptive statistics using SPSS program version 17 (SPSS Inc., Chicago, USA).
Results
The tooth length recorded for first mandibular premolar teeth ranged from 17.80 to 26.60 mm and the average length was 22.48 ± 1.74 mm. A 95% confidence interval of the tooth length for first mandibular premolar based on the mean and standard deviation of sample’s data was (22.26–22.69 mm). Of the 250 teeth, one-rooted mandibular first premolars were 242 teeth (96.8%) and the two-rooted were 8 teeth (3.2%). A mandibular premolar with more than two roots was not found in this study.
Regarding number of canals for first mandibular premolars, 202 teeth (80.8%) had one canal orifice per root including the two-rooted teeth that has one canal orifice in each root. On the other hand, 48 teeth (19.2%) of the one-rooted teeth had two canal orifices. A single main apical foramen was found in 174 teeth (69.6%) whereas 76 teeth (30.4%) showed two or more apical foramina.
Clearing investigation revealed that Vertucci Type I canal configuration represented the highest percentage (61.2%) of all canal types found in this study. There was a complex configuration observed in one tooth that was not described in Vertucci classification. Teeth that have Type IV and V configuration mainly show mesial invagination of their roots. Table 1 shows the frequency distribution of Vertucci classification for the investigated teeth. Fig. 1 shows different types of root canal configurations found in the first mandibular premolar for the studied population.
Table 1.
Frequency of root canal classification of mandibular first premolars for an Egyptian population using tooth clearing method.
| Canal type | Frequency | % |
|---|---|---|
| Vertucci classification | ||
| Type I (1-1) | 153 | 61.2 |
| Type II (2-1) | 14 | 5.6 |
| Type III (1-2-1) | 7 | 2.8 |
| Type IV (2-2) | 33 | 13.2 |
| Type V (1-2) | 41 | 16.4 |
| Type VI (2-1-2) | 1 | 0.4 |
| Complex configuration | ||
| Type (1-2-3) | 1 | 0.4 |
| Total | 250 | 100 |
Fig. 1.
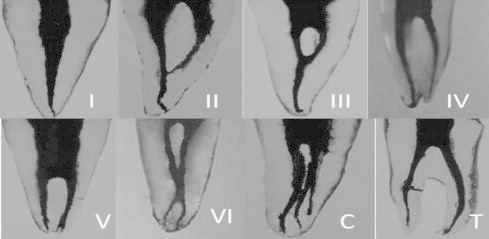
Mesial view for roots of mandibular first premolar: Vertucci’s canal classification Types I, II, III, IV, V and VI. (C) complex configuration (T) two-root premolar.
Accessory canals were detected in a total of 57 teeth (22.8%) that were mainly located in the apical third. There were 28 teeth with one root canal showed apical delta. Inter-canal connections (isthmi) were observed in 62 teeth (24.8%) mainly in the middle third of the root. The apical foramina observation indicated 135 teeth (54%) with apical foramina located laterally (Fig. 2). Table 2 shows the frequency of distribution of the accessory canal and inter-canal connections for the studied teeth.
Fig. 2.
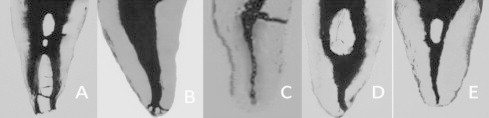
Different features of root canal in mandibular first premolar: (A) inter-canal isthmi connecting two canals, (B) apical delta (C) lateral canal, (D) laterally located apex, and (E) centrally located apex.
Table 2.
Number and percentage of accessory canals and inter-canal connections along different thirds of the root.
| Feature | Accessory canals |
Inter-canal connections (isthmi) |
||
|---|---|---|---|---|
| Root third | Number of teeth | Percentage | Number of teeth | Percentage |
| Coronal third | 2 | 0.8 | 0 | 0 |
| Middle third | 11 | 4.4 | 25 | 10 |
| Apical third | 28 | 11.2 | 19 | 7.6 |
| Mixed (more than one third) | 16 | 6.4 | 18 | 7.2 |
| Total | 57 | 22.8 | 62 | 24.8 |
Discussion and conclusion
Several works have been attempted to clarify the frequency and variations of internal anatomy in various teeth with documented varieties in the external and internal anatomy of the mandibular first premolar [24]. An ethnic influence in dental morphology is expected, as it does for other anatomical features [2]. Therefore, extracted mandibular first premolars were collected for the current study from an indigenous Egyptian population of different areas including the Great Cairo and the Nile delta cities. The current study may not include pure ethnic groups in Egypt such as Bedouin or Nubian population. In addition, age changes were not monitored and variations related to different genders were not recorded. However, the cities included in the study are urban areas with heterogenous inhabitants that can represent the Egyptian population.
Clearing method was used to investigate the internal anatomy to get as much details of the mandibular first premolar. Although various techniques have been used for teeth internal anatomy studies, tooth clearing technique has considerable values because it gives a three-dimensional view of the pulp cavity in relation to the exterior of the tooth. This method also allows visualization of root canal forms and the anastomoses among them [28–29]. The original form and relation of canals is maintained because canal negotiation with instruments is unnecessary [30]. However, the limitation of this method is the difficulty to detect C-shape canal which is better seen with cross sectioning method [31].
The results of the present study revealed 96.8% of first mandibular premolars with one root and 3.2% with two roots. The one-root percentage is close to the rate of an Indian population according to Jain and Bahuguna [32] and a Jordanian population according to Awawdeh and Al-Qudah [24]. A first mandibular premolar with more than two roots was not found which agreed with several studies [4,7,15,17,19,24,32]. Table 3 shows number of roots in the mandibular first premolar for the previous studies compared to the current study.
Table 3.
Percentage for number of roots in the mandibular first premolar for the different studies compared to the current study.
| Reference | Method of study | Population | Number of roots |
|||
|---|---|---|---|---|---|---|
| One (%) | Two (%) | Three (%) | Four (%) | |||
| Trope et al. [4] | In vivo radiographs | American | ||||
| African | 83.8 | 16.2 | 0 | 0 | ||
| Caucasian | 94.5 | 5.5 | 0 | 0 | ||
| Geider et al. [16] | Tooth sectioning and radiography | France | 90.6 | 6.4 | 2.4 | 0.6 |
| Çaliskan et al. [17] | Tooth clearing | Turkey | 100.0 | 0 | 0 | 0 |
| Zaatar et al. [15] | In vivo; postoperative radiographs | Kuwait | 85.0 | 15 | 0 | 0 |
| Sert and Bayirli [7] | Tooth clearing | Turkey | 100.0 | 0 | 0 | 0 |
| Iyer et al. [20] | In vivo; digital radiography | India | 95.9 | 3.9 | 0.2 | 0 |
| Cleghorn et al. [33] | Review article | Global | 97.9 | 1.8 | 0.2 | 0.1 |
| Awawdeh and Al-Qudah [24] | Tooth clearing | Jordan | 97 | 3 | 0 | 0 |
| Peiris [19] | Tooth clearing | Seri Lanka | 98.8 | 1.2 | 0 | 0 |
| Japan | 100 | 0 | 0 | 0 | ||
| Jain and Bahuguna [32] | Tooth clearing | India | 97.11 | 2.89 | 0 | 0 |
| Current study | Tooth clearing | Egypt | 96.8 | 3.2 | 0 | 0 |
The tooth length recorded in this study for first mandibular premolar ranged from 17.80 to 26.60 mm and the average length was 22.48 mm. An average length of 21.2 mm with a range of 17–26 mm was recorded for an Indian population [32] where the average reported for a Jordanian population was 22.6 mm with the shortest of 18 mm and longest of 27 mm [24].
One canal orifice was found in 80.8% of the mandibular first premolar roots of this study while19.2% of the one-rooted teeth had two canal orifices. Table 4 showed number of canal orifices in the mandibular first premolar for the previous studies. The findings of this study are close to the results of Yoshioka et al. [18] who used radiography and clearing to investigate mandibular first premolar in a Japanese population and reported 19.4% of teeth with two canals. However, Peiris [19] reported the lowest frequency of two canal orifices in a Japanese population (1.1%) using clearing method in his study. Lu et al. [14] reported the highest frequency of the two canal orifices in a Chinese population (46%) using in vitro radiography and sectioning method in their study.
Table 4.
Percentage for number of canal orifices in the mandibular first premolar.
| Reference | Method of study | Population | Coronal orifice |
|
|---|---|---|---|---|
| One canal | ⩾2 canals | |||
| Pineda and Kuttler [9] | Radiography | Mexico | 69.3% | 30.7% |
| Zillich and Dowson [10] | Radiography | USA | 75.1% | 24.9% |
| Walker [13] | Radiography | China | 64% | 36% |
| Geider et al. [16] | Sectioning and radiography | France | 68.9% | 31.1% |
| Baisden et al. [12] | Tooth sectioning | USA | 74% | 26% |
| Sabala et al. [6] | Review of patient records | USA | 81.8% | 18.2% |
| Çaliskan et al. [17] | Tooth clearing | Turkey | 64% | 36% |
| Zaatar et al. [15] | Radiographs of RCT teeth | Kuwait | 60% | 40% |
| Yoshioka et al. [18] | Tooth clearing | Japan | 80.6% | 19.4% |
| Sert and Bayirli [7] | Tooth clearing | Turkey | 60.5% | 39.5% |
| Yoshioka et al. [18] | Radiography and tooth clearing | Japan | 80.6 | 19.4 |
| Lu et al. [14] | Radiography and sectioning | China | 54% | 46% |
| Cleghorn et al. [33] | Review article | Global | 75.8% | 24.2% |
| Awawdeh and Al-Qudah [24] | Tooth clearing | Jordan | 58.2% | 41.8% |
| Peiris [19] | Tooth clearing | Seri Lanka | 95.1% | 4.8% |
| Japan | 98.9% | 1.1% | ||
| Velmurugan and Sandhya [21] | Tooth clearing | India | 83% | 17% |
| Jain and Bahuguna [32] | Tooth clearing | India | 88.40% | 11.59% |
| Current study | Tooth clearing | Egypt | 80.8% | 19.2% |
Vertucci’s canal classification [11] was used in this study because it is commonly used by authors in the literature and textbooks. In 1984, Vertucci [11] determined canal numbers and configurations by percentages for each of the human permanent teeth and this can be considered as a baseline point for root canal anatomy comparison [24]. In the current study, Vertucci Type I canal configuration represented the highest percentage (61.2%) of all canal types found in this study. The highest frequency of simple one canal (Class I) was reported as 88.47% in an Iranian population [25] and the lowest was 58.2% in Jordanian [24]. The frequency of simple one-canal pattern in this study lied between a Turkish (60.5%) [7] and a Seri-Lankan population (64.2%) [19]. The highest frequency of class V (1-2 pattern) was reported in a Seri-Lankan population (28.4%) [19] compared to the current study (16.2%). The frequency of two-canal pattern in this study lied between a Jordanian [24] and an Indian [32] populations. Table 5 illustrates the distribution frequency of canal configuration in different studies.
Table 5.
Canal configuration in the mandibular first premolar according to percentage of Vartucci’s classification.
| Reference | Population | Percentage of Vartucci classification |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | VII | VIII | A | ||
| Sert and Bayirli [7] | Turkey | 60.5 | 18.5 | 10.5 | 7 | 2.5 | 0 | 0 | 1 | 0 |
| Vartucci [11] | USA | 70 | 0 | 4 | 1.5 | 24 | 0 | 0 | 0.5 | 0 |
| Peiris [19] | Sri Lanka | 64.2 | 0 | 2.5 | 1.2 | 28.4 | 0 | 0 | 0 | 3.7 |
| Japan | 82.6 | 1.1 | 1.1 | 0 | 15.2 | 0 | 0 | 0 | 0 | |
| Velmurugan and Sandhya [21] | India | 72 | 6 | 3 | 10 | 8 | 0 | 0 | 0 | 1 |
| Awawdeh and Al-Qudah [24] | Jordan | 58.2 | 4.8 | 1.4 | 14.4 | 16.8 | 0.8 | 1.0 | 0 | 2.6 |
| Khidmat et al. [25] | Iran | 88.47 | 1.84 | 3.22 | 0.9 | 4.14 | 0 | 0 | 0 | 1.38 |
| Jain and Bahuguna [32] | India | 67.39 | 7.97 | 3.62 | 2.89 | 17.39 | 0.72 | 0 | 0 | 0 |
| Present study | Egypt | 61.2 | 5.6 | 2.8 | 13.2 | 16.4 | 0 | 0 | 0 | 0.4 |
There was a complex configuration observed in one tooth that was not described in Vertucci’s classification. However, this configuration is not considered as a common finding and depends on the sample size. Other studies [19,24,25] reported uncommon features which can be expected but not to be considered as a frequent occurrence.
Accessory canals were detected in 22.8% of the studied first mandibular premolar that were mainly located in the apical third. The highest and the lowest percentages of accessory canals were reported for Turkish populations. Caliskan et al. [17] reported 52.8% whereas Sert and Bayirli [7] reported 14% of accessory canals although both used clearing method in their studies. Awawdeh and Al-Qudah [24] reported 25.4% of accessory canals in a Jordanian population which seems to be the closest percentage to the current study. However, Vertucci [11] also reported a high percentage (44.3%) of accessory canals. The discrepancy in accessory canal percentages may be applied for inter-canal connections. The current study showed 24.8% of inter-canal connections mainly in the middle third of the root. Vertucci [11] reported 32.1% and Sert and Bayirli [7] reported 7% for this anatomic feature. These discrepancies in percentage can be related to not only the race differences or method of investigation but also to a specific population and the evaluators.
Apically, Sert and Bayirli [7] reported 52.5% of apical foramina located laterally which is the closest percentage to what observed in the present study (54%). Vertucci [11] reported the highest percentage (85%) whereas Caliskan et al. [17] reported the lowest (41.2%). Regarding the apical delta, there were 11.2% of mandibular first premolar observed with apical delta in this study. Lu et al. [14] reported 6% of apical delta in a Chinese population where Awawdeh and Al-Qudah [24] reported 29.2% of this anatomical feature.
Observations of the current study confirmed the presence of ethnic differences among various races and provided some information about the internal anatomy of the mandibular first premolar in an Egyptian population. Endodontists and dental clinicians can use such information to achieve a satisfactory prognosis for root canal treatment. Further studies are recommended for other teeth to develop a comprehensive picture for Egyptian dentition.
Footnotes
Peer review under responsibility of Cairo University.

References
- 1.Vertucci F.J. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3–29. [Google Scholar]
- 2.Vertucci F.J., Haddix J.E., Britto L.R. Tooth morphology and access cavity preparation. In: Cohen S., Hargreaves K.M., editors. Pathways of the pulp. St. Louis; Mosby: 2006. pp. 148–232. [Google Scholar]
- 3.Robertson D., Leeb I.J., McKee M., Brewer E. A clearing technique for the study of root canal systems. J Endod. 1980;6(1):421–424. doi: 10.1016/S0099-2399(80)80218-4. [DOI] [PubMed] [Google Scholar]
- 4.Trope M., Elfenbein L., Tronstad L. Mandibular premolars with more than one root canal in different race groups. J Endod. 1986;12(8):343–345. doi: 10.1016/S0099-2399(86)80035-8. [DOI] [PubMed] [Google Scholar]
- 5.Kim E., Fallahrastegar A., Hur Y.Y., Jung I.Y., Kim S., Lee S.J. Difference in root canal length between Asians and Caucasians. Int Endod J. 2005;38(3):149–151. doi: 10.1111/j.1365-2591.2004.00881.x. [DOI] [PubMed] [Google Scholar]
- 6.Sabala C.L., Benenati F.W., Neas B.R. Bilateral root or root canal aberrations in a dental school patient population. J Endod. 1994;20(3):38–42. doi: 10.1016/s0099-2399(06)80025-7. [DOI] [PubMed] [Google Scholar]
- 7.Sert S., Bayirli G.S. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391–398. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Oliver V.P., Roberto E., Manuel P.S., Carlos H., Nestor C. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 2010;36(5):1919–1931. doi: 10.1016/j.joen.2010.08.055. [DOI] [PubMed] [Google Scholar]
- 9.Pineda F., Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33(1):101–110. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 10.Zillich R., Dowson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol. 1973;36(5):738–744. doi: 10.1016/0030-4220(73)90147-3. [DOI] [PubMed] [Google Scholar]
- 11.Vertucci F.J. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–599. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 12.Baisden M.K., Kulild J.C., Weller R.N. Root canal configuration of the mandibular first premolar. J Endod. 1992;18(10):505–508. doi: 10.1016/S0099-2399(06)81352-X. [DOI] [PubMed] [Google Scholar]
- 13.Walker R.T. Root canal anatomy of mandibular first premolars in a southern Chinese population. Endod Dent Traumatol. 1988;4(5):226–228. doi: 10.1111/j.1600-9657.1988.tb00326.x. [DOI] [PubMed] [Google Scholar]
- 14.Lu T.Y., Yang S.F., Pai S.F. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod. 2006;32(10):932–936. doi: 10.1016/j.joen.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 15.Zaatar E.I., al-Kandari A.M., Alhomaidah S., al-Yasin I.M. Frequency of endodontic treatment in Kuwait: radiographic evaluation of 846 endodontically treated teeth. J Endod. 1997;23(7):453–456. doi: 10.1016/s0099-2399(97)80302-0. [DOI] [PubMed] [Google Scholar]
- 16.Geider P., Perrin C., Fontaine M. [Endodontic anatomy of lower premolars-apropos of 669 cases] J Odontol Conserv. 1989;10(1):11–15. [PubMed] [Google Scholar]
- 17.Caliskan M.K., Pehlivan Y., Sepetcioglu F., Turkun M., Tuncer S.S. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995;21(4):200–204. doi: 10.1016/S0099-2399(06)80566-2. [DOI] [PubMed] [Google Scholar]
- 18.Yoshioka T., Villegas J.C., Kobayashi C., Suda H. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod. 2004;30(2):73–74. doi: 10.1097/00004770-200402000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Peiris R. Root and canal morphology of human permanent teeth in a Sri Lankan and Japanese population. Anthropol Sci. 2008;116(2):123–133. [Google Scholar]
- 20.Iyer V.H., Indira R., Ramachandran S., Srinivasan M.R. Anatomical variations of mandibular premolars in Chennai population. Indian J Dent Res. 2006;17(1):7–10. doi: 10.4103/0970-9290.29898. [DOI] [PubMed] [Google Scholar]
- 21.Velmurugan N., Sandhya R. Root canal morphology of mandibular first premolars in an Indian population: a laboratory study. Int Endod J. 2008;42(1):54–58. doi: 10.1111/j.1365-2591.2008.01494.x. [DOI] [PubMed] [Google Scholar]
- 22.Sandhya R., Velmurugan N., Kandaswamy D. Assessment of root canal morphology of mandibular first premolars in the Indian population using spiral computed tomography: An in vitro study. Indian J Dent Res. 2010;21(2):169–173. doi: 10.4103/0970-9290.66626. [DOI] [PubMed] [Google Scholar]
- 23.Parekh V., Shah N., Joshi H. Root canal morphology and variations of mandibular premolars by clearing technique: an in vitro study. J Contemp Dent Pract. 2011;12(4):318–321. doi: 10.5005/jp-journals-10024-1052. [DOI] [PubMed] [Google Scholar]
- 24.Awawdeh L.A., Al-Qudah A. Root form and canal morphology of mandibular premolars in a Jordanian population. Int Endod J. 2008;41(3):240–248. doi: 10.1111/j.1365-2591.2007.01348.x. [DOI] [PubMed] [Google Scholar]
- 25.Khedmat S., Assadian H., Saravani A.A. Root canal morphology of the mandibular first premolars in an Iranian population using cross-sections and radiography. J Endod. 2010;36(2):214–217. doi: 10.1016/j.joen.2009.10.002. [DOI] [PubMed] [Google Scholar]
- 26.Różyło, Miazek, Różyło-Kalinowska, Burdan Morphology of root canals in adult premolar teeth. Folia Morphol. 2008;67(4):280–285. [PubMed] [Google Scholar]
- 27.JOE Editorial Board. Root Canal Anatomy: An Online Study Guide. J Endod 2008; 34(Number 5S): e7–e17. [DOI] [PubMed]
- 28.Skidmore A.E., Bjorndal A.M. Root canal morphology of the human mandibular first molar. Oral Surg Oral Med Oral Pathol. 1971;32(5):778–784. doi: 10.1016/0030-4220(71)90304-5. [DOI] [PubMed] [Google Scholar]
- 29.Robinson S., Czerny C., Gahleitner A., Bernhart T., Kainberger F.M. Dental CT evaluation of mandibular first premolar root configurations and canal variations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(3):328–332. doi: 10.1067/moe.2002.120055. [DOI] [PubMed] [Google Scholar]
- 30.Gulabivala K., Aung T.H., Alavi A., Ng Y.L. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34(5):359–370. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 31.Fan B., Yang J., Gutmann J.L., Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: Microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod. 2008;34(11):1337–1341. doi: 10.1016/j.joen.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 32.Jain A., Bahuguna R. Root canal morphology of mandibular first premolar in a Gujarati population – an in vitro study. Dent Res J. 2011;8(3):118–122. [PMC free article] [PubMed] [Google Scholar]
- 33.Cleghorn B.M., Christie W.H., Dong C.C. The root and root canal morphology of the human mandibular first premolar: a literature review. J Endod. 2007;33(5):509–516. doi: 10.1016/j.joen.2006.12.004. [DOI] [PubMed] [Google Scholar]