

Abstract
Little is known about specific outcomes and early experiences of total talar prosthesis replacement surgery in the current literature, and ankle arthroplasty in Southeast Asia. This study reported on four patients with talar loss or ankle arthritis. Patients were treated with a custom total talar prosthesis (anatomic-metallic version) replacement (TPR, n=1) or with total ankle replacement (TAR, n=3). Baseline data, including Visual-Analog-Scale Foot and Ankle (VAS-FA) and Quality of Life scores via Short-Form-36 (SF-36), were collected for all patients. Mean follow-up time was 7.6 months. From preoperative to postoperative, VAS-FA score increased from 6.0 to 57.5, and SF-36 score increased from 19.3 to 73.7 in a patient with TPR. Mean VAS-FA scores increased from 51.5±15.6 to 85.7±4.7 (P=0.032), and mean SF-36 scores tended to increase from 65.2±13.3 to 99.3±1.2 (P=0.055) in TAR group. This study is the first report of anatomic-metallic TPR which appears to provide satisfactory outcomes for treatment of talar loss at a short-term follow-up. TAR also provides acceptable results for treatment of ankle arthritis at this point.
Key words: ankle, talus, total ankle replacement, talar prosthesis
Introduction
Since the 1970s, ankle replacements have been performed in Asia in selected patients with end-stage ankle disorders caused by painful osteoarthritis or inflammatory arthritis.1 The initial implant designs were associated with subsidence and loosening, and patient failure rates requiring revision were as high as 8.3-50% over the 5-12.5-year follow-up period.1 These failure rates have raised substantial concerns about the long-term reliability of such prostheses. New ankle replacement designs were developed based on the results of several studies defining normal ankle biomechanics and a review of previous implant failures.2-4 The current implant designs use either two-component (fixed bearings) or three-component (mobile bearings) designs, and fixation without cement is considered better than fixation with cement by most implant manufacturers and surgeons.2,4-8 In addition, the procedure is thought by some to be a sound alternative to the use of ankle arthrodesis.9 However, little was known about the outcomes and experiences of the total talar prosthesis (metallic version) which is the rare type of ankle reconstruction in the current literature and ankle replacements as a treatment for ankle arthritis in Southeast Asia. The aim of this study is to report the results and experiences of the anatomic total talar prosthesis replacement surgery as a main focus, and ankle arthroplasty in our institute, which is the foot and ankle center in Thailand.
Materials and Methods
From May 2013 to April 2014, four patients (mean age: 52.8 years) with ankle arthritis or talar loss were recruited for this study. The patients were divided into two groups based on the mode of ankle replacement: either total ankle replacement (TAR, n=3) or a custom hemi-ankle replacement (HAR)/total talar prosthesis replacement (TPR, n=1). Baseline clinical and radiographic data, including Visual Analog Scale Foot and Ankle (VAS-FA), and Health-related Quality of Life via Short-Form 36 (SF-36) scores,10,11 were collected for all patients. All patients involved provided informed consent for this report.
Operative technique
A tourniquet inflated to 250 mmHg was placed around the thigh in each case. The surgical incision was made via the anterior approach between the tibialis anterior and the extensor hallucis longus tendons. Bone referencing guides for each manufacturer’s design were used to prepare the tibia and talus. Care was taken to remove any residual bone fragments, followed by meticulous irrigation to remove any soft-tissue or bone debris. In the TPR case, no bone cutting at the tibia was performed because only the talus was replaced. Each prosthesis was inserted with the instrumentation and techniques recommended by the respective device manufacturers. To establish a neutral alignment and correct ligament instability or bony deformity, a variety of additional procedures were performed as necessary. In non-complicated cases with no additional procedures, a short-leg cast was applied for 4 weeks. In cases where additional procedures were required, a short-leg cast was applied for a maximum of 6 weeks. The patients were permitted to gradually resume full weight-bearing and preoperative activities as tolerated. All patients underwent follow-up examinations at 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and annually thereafter.
Clinical evaluation
The preoperative and postoperative clinical assessments included the VAS-FA and SF-36 scores. The active ranges of dorsiflexion and plantarflexion were also measured and recorded with a goniometer by an experienced foot and ankle surgeon. Patient age, sex, diagnosis and cause of arthritis, onset time before the operation, and prosthesis type were documented. The operative time was based on the tourniquet time and was collected from the operative and anesthesia records.
Radiological evaluation
Standardized anteroposterior and lateral radiographs (Figure 1A,B) were taken postoperatively at 6 weeks, 3 months, 6 months, 12 months, and then annually. Ankle radiographs from the most recent follow-up were evaluated for the presence and degree of subsidence, migration, and loosening of the prosthesis by a single orthopedic surgeon.
Figure 1.
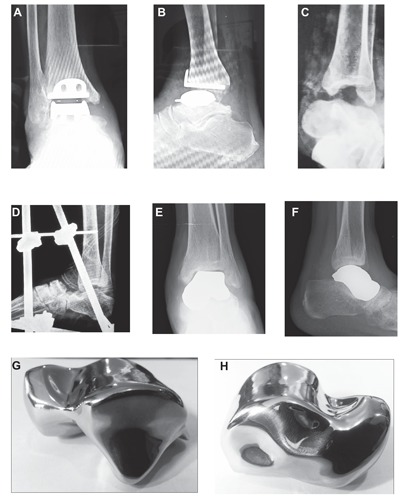
Radiographs of a total right ankle replacement from the anteroposterior (A) and lateral (B) views. Radiographs of a left ankle following severe injury with total talar loss from an anteroposterior view (C), and from a lateral view after temporary external fixation (D). Radiographs of the total left talar prosthesis replacement from the anteroposterior (E) and lateral (F) views. G,H) A custom total talar prosthesis in anatomic-metallic version.
Statistical analysis
Categorical variables were compared using Fisher’s exact test, and continuous variables were compared using the Student’s t-test (for normal distributions) or the Mann-Whitney U-test (for non-normal distributions). Pearson correlation analysis was used to determine the correlation between SF-36 and VAS-FA scores. P<0.05 were considered statistically significant. Data were analyzed using the software package SPSS for Windows version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
The mean age of the patients was 52.8 years, and the mean follow-up time was 7.6 months (range: 4.6-10.6 months). The most common causes of ankle problems were post-traumatic conditions. There were significant improvements in both the VAS-FA and SF-36 scores following the ankle replacements. The total scores of VAS-FA were significantly correlated with total scores of SF-36 in only preoperative phase [Pearson correlation coefficient (r)=0.98, P=0.022]. This correlation was nearly significant at postoperative phase (r=0.94, P=0.058). From preoperative to postoperative, the mean VAS-FA score increased from 40.1±26.1 to 78.6±14.6 (P=0.008), the mean SF-36 score increased from 53.7±25.4 to 92.9±12.8 (P=0.015), the mean plantarflexion increased from 4.3±3.0 to 24.0±10.8 degrees (P=0.031), and the mean total ankle motion increased from 3.0±2.4 to 26.5±9.0 degrees (P=0.009). The preoperative and postoperative mean dorsiflexions were −1.3±2.5 and 2.5±2.1 degrees (P=0.122).
Total talar prosthesis replacement or hemi-ankle replacement
There was only one subject, who was male, in the total talar prosthesis replacement (TPR) group. The patient age was 25 years. The cause of his ankle problem was severe traumatic loss of the entire talus (Figure 1C,D). The duration of symptoms before the definitive treatment was approximately 3 months and the follow-up time was 4.6 months. A custom iTalar-M prosthesis was implanted in this patient. This prosthesis was manufactured as a custom-made implant for this patient by the author and colleagues using three-dimensional computed tomography imaging of the contralateral talus with computer graphics, and development with medical grade (stainless steel) (Figure 1G,H). The custom prosthesis in the current study consisted of: i) trochlea tali central arc length (TaALc: a distance between the most anterior and posterior and proximal points of the trochlea tali, as seen in the sagittal projection of the talus or our talar prosthesis) as 35.1 mm; ii) trochlea tali width [TaWc: a width between medial and lateral crests of the talar dome at central location along mediolateral (M/L) axis] as 27.8 mm. These distances were in the ranges of same parameters in the previous studies.12-14 The three-dimensional computer graphics-based talar morphometry with computed tomography was analyzed and compared with the previous studies (Figure 2).12-14 The mean ratio of the anteroposterior (length) and medio-lateral (width) dimensions of the trochlea tali (TaALc/TaWc) of a custom prosthesis in the current study was in the range among the same ratios of previous studies.13,14 These evidences confirmed the anatomic design of total talar prosthesis in the current study. For the operation, the surgical findings revealed that the ankle joint and subtalar joint of this patient had no significant arthritic changes. Then, the author decided to perform the total talar prosthesis replacement for him. The operative time was 230 minutes. From preoperative to postoperative, the VAS-FA score increased from 6.0 to 57.5, the SF-36 score increased from 19.3 to 73.7, the dorsiflexion increased from 0 to 5 degrees, the plan-tarflexion increased from 0 to 16 degrees, and the total ankle motion increased from 0 to 21 degrees. The preoperative and postoperative inversions were 0 and 10 degrees, and the eversions were 0 and 13 degrees. There were no intraoperative or postoperative complications. There was no sign of prosthesis migration at the last follow-up visit for this patient (Figure 1E,F). The patient was able to return to stand and walk as full-weight bearing without gait aid (Figure 3A-E). He was able to mobilize and perform his activity-daily living by himself with more convenience. His quality of life was substantially improved at the latest follow-up period.
Figure 2.
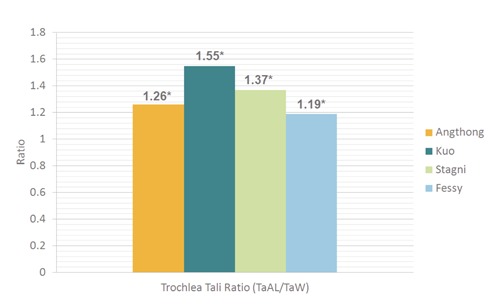
Mean ratios (*) of the anteroposterior (length) and medio-lateral (width) dimensions of the trochlea tali (TaALc/TaWc) in the current study (talar prosthesis), and the ratios of the means of the same dimensions reported in Fessy et al. 14 and Stagni et al. 13 and Kuo et al. 12 Mean ratios of the individual dimensions are also given above the bars. Abbreviations: TaALc, Trochlea tali central arc length: distance between the most anterior and posterior and proximal points of the trochlea tali, as seen in the sagittal projection of the talus or talar prosthesis (current study); TaWc, Trochlea tali width: width between medial and lateral crests of the talar dome at central location along mediolateral (M/L) axis).
Figure 3.

Standing and walking appearance included ankle dorsiflexion/plantarflexion around three months after an implantation of a prosthesis in a left ankle.
Total ankle replacement
There were two females (66.7%) and one male (33.3%) in the total ankle replacement (TAR) group. The mean age was 63 years. The causes of ankle arthritis were post-traumatic arthritis (in two patients; 66.7%) and rheumatoid arthritis (in one patient; 33.3%). The mean duration of symptoms before the definitive treatment was 39.3 months, and the mean follow-up time was 8.5 months. HINTEGRA® prostheses (Newdeal SA, Lyon, France) were implanted in all patients.15 The mean operative time was 220 minutes. From preoperative to postoperative, the mean VAS-FA scores increased from 51.5±15.6 to 85.7±4.7 (P=0.032), and mean SF-36 scores tended to increase from 65.2±13.3 to 99.3±1.2 (P=0.055). The mean dorsiflexion insignificantly increased from −1.7±2.9 to 1.7±1.5 degrees (P=0.30), the mean plantarflexion insignificantly increased from 5.7±1.2 to 26.7±11.5 degrees (P=0.096), and the mean total ankle motion significantly increased from 4.0±1.7 to 28.3±10.1 degrees (P=0.047). There were no occurrences of intraoperative or postoperative complications, and no signs of loosening, subsidence, or migration of any of the prostheses at the last follow-up visit for all patients (Figure 1A,B).
Discussion
The present study is the first report in current literature to present the early results and experiences of the anatomic total talar replacement surgery with a custom prosthesis based on the three-dimensional computer graphics-based talar morphometry with computed tomography. This study is also the first report which presented the early results of total ankle replacements in Southeast Asia. Anatomic TPR provided satisfactory outcomes for the treatment of traumatic total talar loss at the short-term follow-up. TAR also provides acceptable results for treatment of ankle arthritis. These treatments were able to significantly improve the functional outcomes of patients as assessed by VAS-FA score, and a nearly significant improvement in quality of life as assessed by the SF-36 score. The patients who received these treatments achieved improvements in their ankle ranges of motion, particularly in the total ankle motion. For the total talar prosthesis replacement (TPR) case, the present study was the first report in the English literature to present the results of a total talar prosthesis replacement with a custom anatomic metallic design (the iTalar-M prosthesis) in a patient with traumatic total talar loss. The talar profiles as TaALc and TaWc were analyzed and found that they were in the ranges of same parameters in the previous studies.12-14 The mean ratio of the TaALc/TaWc of a custom prosthesis in the current study was in the range among the same ratios of previous studies (Figure 2).13,14 These evidences confirmed the anatomic design of total talar prosthesis in the current study. For the results of talar prosthesis replacement, the previous studies of this type of replacement were mainly from Harnroongroj and Harnroongroj, and Taniguchi et al.16,17 Harnroongroj and Harnroongroj reported the outcomes of metallic talar body prosthesis replacement at ten to thirty-six years of follow-up which provided satisfactory function of the foot and ankle.16 Taniguchi et al. reported the results of ceramic talar body prosthesis replacement in 22 patients.17 They proposed the concerns about loosening and sinking between the talar body prosthesis and talar neck.17 They were not able to recommend the uses of talar body prosthesis regarding the results in their studies; however, they recommend the use of a total talar implant instead.17 The results of both studies are still controversial. Moreover, both previous studies16,17 used American Orthopedic Foot and Ankle Society (AOFAS) ankle/hindfoot scoring system,18 which was inadequately validated scoring system.19 The comparisons between the results in previous studies and the current study were summarized in Table 1. The patient with an anatomic metallic prosthesis in the current study achieved improvement in functional outcomes and quality of life, and regained significant ankle and subtalar motions in the short-term period after the operation. Additional follow-up over a longer period is needed to determine the medium- to long-term results of anatomic TPR. Based on these results, the author believes that anatomic TPR may be used to replace the entire talus after traumatic total talar loss or severe crush injury of the talus, thus maintaining the clinical function of the ankle and hindfoot over the medium to long term. For the TAR, a previous study in an Asian population found improvements in ankle scores 5.2 years after TAR.20 The results of the present study are consistent with the previous report. However, the mean follow-up time in the present study was still during the short-term period. Additional follow-up at later time points is necessary to determine the medium- to long-term results of TAR. Regarding the improvement in ankle motions, Dyrby et al.21 evaluated ankle joint function during walking before and after TAR with the STAR design, and reported a significant improvement in postoperative ankle motion, but decreased ankle motion compared with normal controls. The results of the present study were also consistent with this previous report. The patients with TAR achieved improvements in their ankle ranges of motion, particularly in the total ankle motion. Although the total ankle motion may be less than normal ankle motion, the magnitude of this motion (28.3 degrees) was greater than in a previous report (26.8 degrees).22
Table 1.
The comparisons between the results in previous studies and the current study.
| Author | Prosthesis type | Prosthesis design | Scoring system | Validity of scoring system | Overall results | Subtalar motion after implantation |
|---|---|---|---|---|---|---|
| Angthong10 | Total talus | Anatomic* | VAS-FA SF-36 | Adequatea | Satisfactory | Excellent |
| Harnroongroj et al. 16 | Talar body | Non-anatomic° | AOFASb | Inadequate§ | Satisfactory | Restriction^ |
| Taniguchi et al.17 | Talar body | Anatomic# | AOFAS | Inadequate§ | Mixed | N/A |
VAS-FA, Visual Analog Scale Foot and Ankle; SF-36, Health-related Quality of Life via Short-Form 36 score; AOFAS, American Orthopedic Foot and Ankle Society ankle/hindfoot scoring system; N/A, not applicable
*Anaomic design using three-dimensional computed tomography imaging of the contralateral talus with computer graphics and talar profiles was shown anatomically.
°No data was shown about the processing of talar shape using special imaging or computed tomography.
#Anaomic design using three-dimensional computed tomography imaging of the contralateral talus with a stereolithographic model but no data was shown about anatomic talar profiles.
§SooHoo et al.19
^Restriction of subtalar joint motion with no goniometer used.
bNo preoperative AOFAS scores were mentioned.
Conclusions
Anatomic TPR provided satisfactory outcomes for the treatment of talar loss in a short-term follow-up. This treatment was able to satisfactorily improve the functional outcomes and quality of life in a patient of the current study. TAR also provides acceptable results for treatment of ankle arthritis at this point. The treated patients also achieved improvements in their ankle function and total ankle motion. Additional follow-up at later time points is necessary to determine the medium- to long-term outcomes of anatomic TPR and TAR.
Acknowledgments
The author would like to give special thanks to Mr. Apitan Lee and Mr. Kittipat Chirungsarpsook for their supports of the iTalar prosthesis.
References
- 1.Takakura Y, Tanaka Y, Kumai T, et al. Ankle arthroplasty using three generations of metal and ceramic prostheses. Clin Orthop Relat Res 2004:130-6 [DOI] [PubMed] [Google Scholar]
- 2.Chou LB, Coughlin MT, Hansen S, Jr, et al. Osteoarthritis of the ankle: the role of arthroplasty. J Am Acad Orthop Surg 2008;16:249-59 [DOI] [PubMed] [Google Scholar]
- 3.Giannini S, Leardini A, O’Connor JJ.Total ankle replacement: review of the designs and of the current status. Foot Ankle Surg 2000;6:77-88 [Google Scholar]
- 4.Gougoulias NE, Khanna A, Maffulli N.History and evolution in total ankle arthroplasty. Br Med Bull 2009;89:111-51 [DOI] [PubMed] [Google Scholar]
- 5.Buechel FF, Sr, Buechel FF, Jr, Pappas MJ.Twenty-year evaluation of cementless mobile-bearing total ankle replacements. Clin Orthop Relat Res 2004;424:19-26 [DOI] [PubMed] [Google Scholar]
- 6.Cracchiolo A, III, Deorio JK.Design features of current total ankle replacements: implants and instrumentation. J Am Acad Orthop Surg 2008;16:530-40 [PubMed] [Google Scholar]
- 7.Guyer AJ, Richardson G.Current concepts review: total ankle arthroplasty. Foot Ankle Int 2008;29:256-64 [DOI] [PubMed] [Google Scholar]
- 8.Hintermann B, Valderrabano V, Dereymaeker G, Dick W.The HINTEGRA ankle: rationale and short-term results of 122 consecutive ankles. Clin Orthop Relat Res 2004;424:57-68 [DOI] [PubMed] [Google Scholar]
- 9.Haddad SL, Coetzee JC, Estok R, et al. Intermediate and long-term outcomes of total ankle arthroplasty and ankle arthrodesis: a systematic review of the literature. J Bone Joint Surg 2007;89:1899-905 [DOI] [PubMed] [Google Scholar]
- 10.Angthong C, Chernchujit B, Suntharapa T, Harnroongroj T.Visual analogue scale foot and ankle: validity and reliability of Thai version of the new outcome score in subjective form. J Med Assoc Thai 2011; 94:952-7 [PubMed] [Google Scholar]
- 11.Jirarattanaphochai K, Jung S, Sumananont C, Saengnipanthkul S.Reliability of the medical outcomes study short-form survey version 2.0 (Thai version) for the evaluation of low back pain patients. J Med Assoc Thai 2005;88:1355-61 [PubMed] [Google Scholar]
- 12.Kuo CC, Lu HL, Leardini A, et al. Three-dimensional computer graphics-based ankle morphometry with computerized tomography for total ankle replacement design and positioning. Clin Anat 2014;27:659-68 [DOI] [PubMed] [Google Scholar]
- 13.Stagni R, Leardini A, Ensini A, Cappello A.Ankle morphometry evaluated using a new semi-automated technique based on X-ray pictures. Clin Biomech 2005;20:307-11 [DOI] [PubMed] [Google Scholar]
- 14.Fessy MH, Carret JP, Bejui J.Morphometry of the talocrural joint. Surg Radiol Anat 1997;19:299-302 [DOI] [PubMed] [Google Scholar]
- 15.Angthong C, Chumchuen S, Khadsongkram A.Total ankle arthroplasty with ceramic prostheses: a systematic review of medium-term outcomes and failure rates. Hard Tissue 2013;2:15. [DOI] [PubMed] [Google Scholar]
- 16.Harnroongroj T, Harnroongroj T.The talar body prosthesis: results at ten to thirty-six years of follow-up. J Bone Joint Surg Am 2014;96:1211-8 [DOI] [PubMed] [Google Scholar]
- 17.Taniguchi A, Takakura Y, Sugimoto K, et al. The use of a ceramic talar body prosthesis in patients with aseptic necrosis of the talus. J Bone Joint Surg Br 2012;94:1529-33 [DOI] [PubMed] [Google Scholar]
- 18.Kitaoka HB, Alexander IJ, Adelaar RS, et al. Clinical rating systems for the anklehindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1994;15:349-53 [DOI] [PubMed] [Google Scholar]
- 19.SooHoo NF, Shuler M, Fleming LL.Evaluation of the validity of the AOFAS clinical rating systems by correlation to the SF-36. Foot Ankle Int 2003;24:50-5 [DOI] [PubMed] [Google Scholar]
- 20.Angthong C, Chumchuen S, Khadsongkram A.A systematic review of intermediate-term outcomes and failure rates for total ankle replacements: an Asian perspective. Foot Ankle Surg 2013;19:148-54 [DOI] [PubMed] [Google Scholar]
- 21.Dyrby C, Chou LB, Andriacchi TP, Mann RA.Functional evaluation of the Scandinavian total ankle replacement. Foot ankle Int 2004;25:377-81 [DOI] [PubMed] [Google Scholar]
- 22.Zhao H, Yang Y, Yu G, Zhou J.A systematic review of outcome and failure rate of uncemented Scandinavian total ankle replacement. Int Orthop 2011;35:1751-8 [DOI] [PMC free article] [PubMed] [Google Scholar]