

Abstract
Coracoid process fractures are rare and often associated with dislocations of the acromioclavicular (AC) joint. There is little evidence about the treatment of these injuries in adolescents, but the few case reports published recommend surgery. We report a case of a dislocated epiphyseal fracture to the base of the coracoid process with AC joint dislocation in a 14-year-old ice-hockey player following direct impact to his left shoulder. Since magnetic resonance tomography revealed intact AC and coracoclavicular ligaments, we initiated non-operative treatment with immobilization and unloading of the shoulder by an abduction brace allowing limited rotation for 6 weeks. This treatment resulted in complete recovery after 8 weeks and return to full sports on first league level after 3 month. In conclusion, non-operative treatment of coracoid base fractures with concomitant AC-joint injury in the adolescent can result in excellent functional results and early recovery.
Key words: coracoid fracture, acromioclavicular joint dislocation, treatment
Case Report
A 14-year-old boy sustained a direct impact to his left shoulder due to an ice-hockey body-check. He complained acute pain and loss of function of his left shoulder. Initially the shoulder was immobilized in a shoulder sling and the patient was introduced to our department for shoulder and elbow surgery 10 days after the injury. Clinically, he presented with a prominent left acromioclavicular (AC) joint with pain on horizontal and vertical manipulation of the lateral clavicle, as well as marked tenderness over the coracoid process. Functional evaluation of the AC joint revealed a moderate superoinferior (3-5 mm) but no anteroposterior instability. Active range of motion (ROM) was restricted in every direction [ab-/adduction (Abd/Add): 50-0-10°; flexion/extension (F/E): 60-0-30°; external/internal rotation (ER/IR): 40-0-85°], passive ROM was normal. There was no evidence for an injury of brachial plexus or vascular compromise. The patient’s demands were complete and fast recovery with return to full sports as soon as possible, since he was playing ice-hockey in a first league team.
Computed tomography (CT) showed an AC joint separation with elevation of the lateral clavicle of 5 mm (Figure 1A) and a fracture at the epiphysis of the coracoid base with 3 mm dislocation medially (Figure 1B-D). The magnetic resonance imaging (MRI) revealed an AC joint sprain with intact AC capsule and ligaments as well as intact coracoclavicular ligaments (CCL) (Figure 1E).
Figure 1.
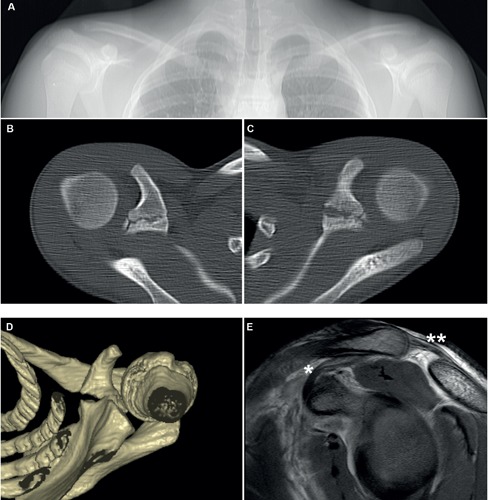
Initial computed tomography (CT) and magnetic resonance imaging (MRI). An AC joint separation with 5mm elevation of the lateral clavicle was diagnosed in the CT topography (A). Axial views of right (B) and left (C) shoulder showed an epiphyseal fracture at the left coracoid base with a medial dislocation of 3mm. Three-dimensional reconstruction of the left shoulder with view from inferior (D). MRI scan revealed intact CCL, (*) accessory epiphysis and superior AC ligament (**) (E).
We started non-operative treatment on first presentation with immobilization in a Camo®Shoulder brace (OPED, Valley/Oberlaindern, Germany). This device allows resting of the 90° flexed elbow on a pad, thereby partially unloading the shoulder girdle, with fixed abduction of 15° and internal rotation of 45° (Figure 2A). At clinical and radiological follow-up 2 weeks later, the patient presented with persisting tenderness over the coracoid process but less tenderness over the AC joint. Active ROM was still markedly restricted (Abd/Add: 60-0-10°; F/E: 60-0-30°; ER/IR: 40-0-80°). The radiographs ruled out a secondary dislocation of the coracoid process. Passive rotation of the shoulder within the dynamic brace was allowed between 30 and 60° IR from week 4 and between 20 to 80° IR from week 5 (Figure 2B). At 8 weeks follow-up the patient presented completely pain-free with full ROM (Figure 3A-D) and without tenderness on palpation over the coracoid or the AC joint. Clinical tests for the AC joint, rotator cuff and long biceps tendon revealed to be normal. After week 8 the patient resumed ice-hockey training and regained sports activity on first league level after 12 weeks. After 5 months he presented with mild symptoms of subcoracoid impingement which was successfully treated with physiotherapy within 6 weeks. A MRI confirmed complete bony healing of the coracoid fracture without malalignement, a coracohumeral distance of 13mm and signs of a mild subcoracoid bursitis (Figure 3F,G).
Figure 2.

Non-operative treatment using an abduction brace allowing partial unloading in 15° shoulder abduction and 45° internal rotation. Furthermore, mobilization with passive rotation can be conducted from week 4 within the brace.
Figure 3.
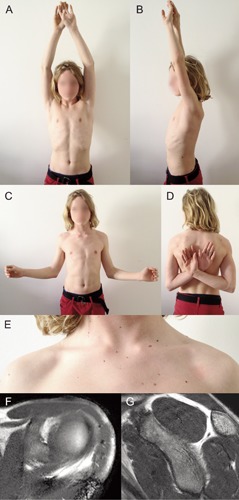
Functional, cosmetic and radiographic outcome 8 weeks after trauma. Full pain free range of motion was achieved as shown in A-D. A slight prominence is seen at the left lateral clavicle (E). Complete bony healing was confirmed by magnetic resonance imaging 6 month after trauma (F-G).
Discussion
Fractures of the coracoid process are uncommon and account for only 2-13% of scapular fractures.1-3 Ogawa et al. classified these fracture according to their relationship to the CCL: type I fractures occur proximally and type II fractures distally to the attachment of the CCL.4 Both fractures are suggested to be avulsion fractures. Type I fractures are caused by pulling force of the CCL and type II by muscular violence of the short head of biceps, the coracobrachialis and the pectoralis minor.2,5-7 The coracoid has two ossification centers, where fractures preferably occur in children and adolescent. One is located at the base of the coracoid process and the other is an accessory ossification center over its tip.8 This accessory epiphysis is the insertion site of the CCL. It is assumed that in the immature skeleton, the epiphyses are weaker than the actual CCL, therefore contributing to type I fractures or fractures of the accessory epiphysis.8,9
In adults, type I coracoid fractures are usually non- or minimally displaced and can be treated non-operatively, unless there is an associated ipsilateral AC joint separation.10,11 Associated AC joint dislocations are reported in more than 50% of coracoid fractures.4 The few studies suggest a difference between adolescent and skeletally mature patients with regard to this injury pattern. Since in adolescent the CCL are stronger than the attachment of the epiphyseal plates, the forces will result in an avulsion of the coracoid process,12 whereas in the mature skeleton, the coracoid process and the clavicle are stronger than the CCL complex, resulting in an AC dislocation without coracoid fracture, but with CCL disruption.8
In our case MRI and CT revealed a moderately displaced epiphyseal fracture at the base of the coracoid (type I) in association with an AC joint dislocation with 5 mm elevation of the clavicle (Figure 1A-D). The AC ligaments, the accessory epiphysis and CCL were shown to be intact (Figure 1E). These findings support the mechanism of avulsion of the base of coracoid process by the CCL as suggested by Protass et al.12 The classification of the associated AC joint dislocation is difficult in these cases, since the popular classification systems are based on the extent of the AC ligament and CCL disruption. These classifications imply an intact coracoid process.13,14 Therefore, we here preferred to describe the AC dislocation by the distance of elevation of the lateral clavicle in comparison to the contralateral site.
The evidence for treating these injuries in adults is low, as it is only based on case reports, case series and retrospective analyses.6-8,11 The most recent treatment recommendations support surgery according to the grade of disruption of the superior shoulder suspensory complex (SSSC). The SSSC is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts from which the upper extremity is suspended.15,16 The ring is composed of the glenoid process, coracoid process, CCL, distal clavicle, AC joint, and acromial process. The SSSC is biomechanically extremely important. Rupture of any two parts of SSSC is defined as a floating shoulder and requires surgery according to the authors.15,16
We report a case of non-operative treatment of an epiphyseal base fracture of the coracoid process combined with a 5 mm dislocation of the AC joint in a 14-year-old ice-hockey player. Pain free full ROM was achieved after 8 weeks and the patient was able to return to full sports after 3 months. To our knowledge there is only one similar case described by Jettoo et al. for the immature skeleton in a case of a 12-year-old boy. 17 The authors performed operative treatment with lag screw osteosynthesis of the coracoid process and k-wire fixation of the AC joint. After uneventful healing, pain free full ROM was not achieved before 5 months and the patient was discharged after 9 months. The exact grade of AC dislocation was not evaluated, but the authors report on a complete rupture of the AC joint intraoperative. In comparison, our non-operative treatment led to a faster recovery.
Black et al. reported that traumatic AC separations in the skeletally immature patient are frequently overdiagnosed and overtreated, since in most cases the AC joint is suggested not to be ruptured, but only widened. Therefore, long-term follow-ups of these patients demonstrate excellent results after non-operative treatment.18 In our case we performed MRI in order to exactly determine the injury to the AC joint and to indicate the treatment accordingly. Our non-operative treatment was carried out with a modern abduction brace ensuring partial unloading of the shoulder as suggested by Ogawa et al. in order prevent secondary dislocation.4 So far, immobilization devices described by authors favoring nonoperative management include broad arm slings,10,19 Desault-, Velpeau-, Watson-Jones-or collar-and-cuff-bandages.11 All these devices provide a fixation of the shoulder girdle in 0° abduction and fixed internal rotation at 90°. In contrast, the brace used in our case allows early passive and active shoulder rotation to prevent shoulder stiffness. These advantages might contribute to the excellent functional outcome and fast recovery.
Conclusions
Non-operative treatment of type I fractures of the coracoid process in association with AC dislocation in the adolescent can result in excellent functional outcome and early return to full sports, even in young athletes with high functional demands. We recommend performing an MRI scan of the shoulder in order to exactly assess the injury to the AC joint with special regards to the AC ligaments. Modern shoulder braces allowing unloading of the shoulder girdle and early passive rotation can contribute to early recovery.
References
- 1.Eyres KS, Brooks A, Stanley D.Fractures of the coracoid process. J Bone Joint Surg Br 1995;77:425-8 [PubMed] [Google Scholar]
- 2.Ogawa K, Yoshida A, Takahashi M, Ui M.Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17-9 [DOI] [PubMed] [Google Scholar]
- 3.Ada JR, Miller ME.Scapular fractures. Analysis of 113 cases. Clin Orthop Relat Res 1991:174-80 [PubMed] [Google Scholar]
- 4.Ogawa K, Ikegami H, Takeda T, Watanabe A.Defining impairment and treatment of subacute and chronic fractures of the coracoid process. J Trauma 2009;67:1040-5 [DOI] [PubMed] [Google Scholar]
- 5.Goss TP.Scapular fractures and dislocations: diagnosis and treatment. J Am Acad Orthop Surg 1995;3:22-33 [DOI] [PubMed] [Google Scholar]
- 6.Wang KC, Hsu KY, Shih CH.Coracoid process fracture combined with acromioclavicular dislocation and coracoclavicular ligament rupture. A case report and review of the literature. Clin Orthop Relat Res 1994:120-2 [PubMed] [Google Scholar]
- 7.Wilson KM, Colwill JC.Combined acromioclavicular dislocation with coracoclavicular ligament disruption and coracoid process fracture. Am J Sports Med 1989;17: 697-8 [DOI] [PubMed] [Google Scholar]
- 8.Montgomery SP, Loyd RD.Avulsion fracture of the coracoid epiphysis with acromioclavicular separation. Report of two cases in adolescents and review of the literature. J Bone Joint Surg Am 1977;59: 963-5 [PubMed] [Google Scholar]
- 9.Green NE, Swiotkowski MF.Fractures and dislocations about the shoulder. Skel Trauma Child 2008;4:292 [Google Scholar]
- 10.Carr AJ, Broughton NS.Acromioclavicular dislocation associated with fracture of the coracoid process. J Trauma 1989;29:125-6 [DOI] [PubMed] [Google Scholar]
- 11.Martin-Herrero T, Rodriguez-Merchan C, Munuera-Martinez L.Fractures of the coracoid process: presentation of seven cases and review of the literature. J Trauma 1990;30:1597-9 [PubMed] [Google Scholar]
- 12.Protass JJ, Stampfli FV, Osmer JC.Coracoid process fracture diagnosis in acromioclavicular separation. Radiology 1975;116:61-4 [DOI] [PubMed] [Google Scholar]
- 13.Tossy JD, Mead NC, Sigmond HM.Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop Relat Res 1963;28:111-9 [PubMed] [Google Scholar]
- 14.Goss TP, Rockwood CA, Jr, Matsen FA, et al., Fractures of the scapula. The shoulder. 3rd edn. Philadelphia: Saunders; 2004. pp 413-54 [Google Scholar]
- 15.Goss TP.Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106 [DOI] [PubMed] [Google Scholar]
- 16.Owens BD, Goss TP.The floating shoulder. J Bone Joint Surg Br 2006;88:1419-24 [DOI] [PubMed] [Google Scholar]
- 17.Jettoo P, de Kiewiet G, England S.Base of coracoid process fracture with acromioclavicular dislocation in a child. J Orthop Surg Res 2010;5:77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Black GB, McPherson JA, Reed MH.Traumatic pseudodislocation of the acromioclavicular joint in children. A fifteen year review. Am J Sports Med 1991; 19:644-6 [DOI] [PubMed] [Google Scholar]
- 19.Hak DJ, Johnson EE.Avulsion fracture of the coracoid associated with acromioclavicular dislocation. J Orthop Trauma 1993; 7:381-3 [PubMed] [Google Scholar]