

Abstract
Background/Aim:
Development of hepatic dysfunction is a well-recognized complication of total parenteral nutrition in preterm infants. Previous studies reported the incidence of total parenteral nutrition–associated cholestasis and described possible contributing factors to its pathogenesis, but little is done trying to determine its possible predictive risk factors. The aims of this study was to determine the incidence of total parenteral nutrition–associated cholestasis and to develop a possible predictive model for its occurrence.
Patients and Methods:
A review of medical records of all very low birth weight infants admitted to neonatal intensive care unit at King Khalid University Hospital, Riyadh, Saudi Arabia, between January 2001 and December 2003 was carried out. The infants were divided into two groups: Cholestasis and noncholestasis, based on direct serum bilirubin level >34 μmol/L. A multivariate logistic regression analysis was performed to calculate the statistical significance of risk factors. Receiver–operating characteristic curve was used to determine the optimal cutoff points for the significant risk factors and to calculate their sensitivity and specificity. The level of significance was set at P ≤ 0.05.
Results:
A total of 307 patients were included in the analysis. The incidence of cholestasis in the whole population was 24.1% (74 patients). Infants with cholestasis had a lower birth weight, 735.4 ± 166.4 g vs. 1185.0 ± 205.6 g for noncholestasis group (P < 0.001), whereas the mean gestational age for the two groups was 25.4 ± 2.1 week and 28.9 ± 2.1 week, respectively (P < 0.001). The significant risk factors for the development of cholestasis were birth weight (P = 0.006) with an odds ratio of 0.99 [95% confidence interval (CI), 0.98, 0.99]; sensitivity of 92%, specificity of 87%; and total parenteral nutrition duration (P < 0.001) with an odds ratio of 1.18 (95% CI, 1.10, 1.27); sensitivity of 96%, specificity of 89%.
Conclusions:
A lower birth weight and longer duration of total parenteral nutrition were strong predictive risk factors for the development of cholestasis in preterm infants.
Keywords: Cholestasis, preterm, total parenteral nutrition
Total parenteral nutrition (TPN) has been widely used in infants and adults since the late 1960s. It represents a major advancement in the care of very low birth weight (VLBW) infants and to neonates who are unable to tolerate enteric nourishment regardless of cause.[1]
The development of significant reversible hepatic dysfunction, TPN-associated cholestasis (TPN-AC), is a well-recognized complication of prolonged TPN in preterm infants.[2] It is characterized by cholestatic jaundice, which is defined as direct serum bilirubin of ≥34 μmol/L with or without liver enzymes abnormalities. In 1971, Peden and co-workers[3] first reported the occurrence of cholestasis in infants receiving TPN, with incidence averaging approximately 30%.[4] The exact etiology of TPN-AC remains obscure, although numerous factors have been cited as contributing to its pathogenesis.[5] The severity of the disease varies from mild to severe, which could lead to significant hepatic injury and end-stage liver disease. Most of clinical studies have described an association between the severity of the histopathological changes and the duration of TPN therapy.[6,7,8] Cohen and Olsen suggested that cholestasis may occur within 2 weeks and cirrhosis may develop within 3-5 months of therapy.[7] A schedule to predict the degree of liver injury based on the duration of therapy has also been proposed by Mullick et al.[9]
Different policies of prevention were proposed to decrease the incidence and the severity of TPN AC, namely, shortened TPN course and early initiation of enteral feeding. The components of TPN also contribute to the pathogenesis of TPN-AC, including taurine and carnitine deficiency, aluminum and manganese toxicity, and oxidant imbalance.[10] Although effective therapeutic strategies for TPN-AC have not been established, limited options are available. Ursodeoxycholic acid (UDCA, 10 − 30 mg/kg/day) is presently the most widely used in the treatment of TPN-AC.[11,12,13]
Although previous studies reported the incidence of TPN-AC and described the potential contributing factors to its pathogenesis, very few tried to look at the predictive risk factors of TPN-AC for possible prevention. The present study was carried out to determine the incidence of TPN-AC in VLBW infants, and to develop a possible predictive model for its occurrence.
PATIENTS AND METHODS
Patients and clinical variables
This is a retrospective analysis of medical records of all VLBW infants admitted to the neonatal intensive care unit (NICU) at King Khalid University Hospital, King Saud University, Riyadh, Saudi Arabia, between January 2001 and December 2003. Excluded were infants who had significant congenital malformations, died in the first 10 days of life or had other confirmed causes of cholestasis other than TPN-AC. Significant cholestatic jaundice was defined as direct serum bilirubin > 34 μmol/L. TPN formula used during the study period was Vaminolact (Fresenius Kabi, Homburg, Germany). The components of TPN were adjusted and individualized according to the patient's clinical condition. A total of 3 g/kg/day of amino acids and 3 g/kg/day of intralipid were infused continuously over 24 h via peripheral or central line. For the sake of analysis, the patients were divided into two groups: Cholestasis and noncholestasis groups, based on the value of direct serum bilirubin.
The possible risk factors collected were gestational age (GA), birth weight (Bwt), gender, Apgar score (AS), TPN duration, age at initial feeding, age at full feeds, episodes of culture-confirmed sepsis, umbilical arterial and venous catheterization, bronchopulmonary dysplasia (BPD), patent ductus arteriosus (PDA), and necrotizing enterocolitis (NEC). Bacterial sepsis was defined as positive blood, cerebrospinal fluid, or urine culture. The age at initial feeding was defined as the age of the first enteral feed.
Statistical analysis
Statistical analysis was performed using SPSS version 16.0 (SPSS Inc, Chicago, IL, USA). All continuous variables represented by mean ± standard deviation and categorical variables by frequencies and percentages. Chi-square analysis was used to compare categorical variables, whereas independent sample t test was used to compare continuous variables among the two groups. Multivariate logistic regression analysis was performed to calculate statistical significance of the risk factors as covariates. Receiver–operating characteristic (ROC) curve was used to determine optimal cutoff points for the significant risk factors and to calculate their sensitivity and specificity. Level of significance was set at P ≤ 0.05.
RESULTS
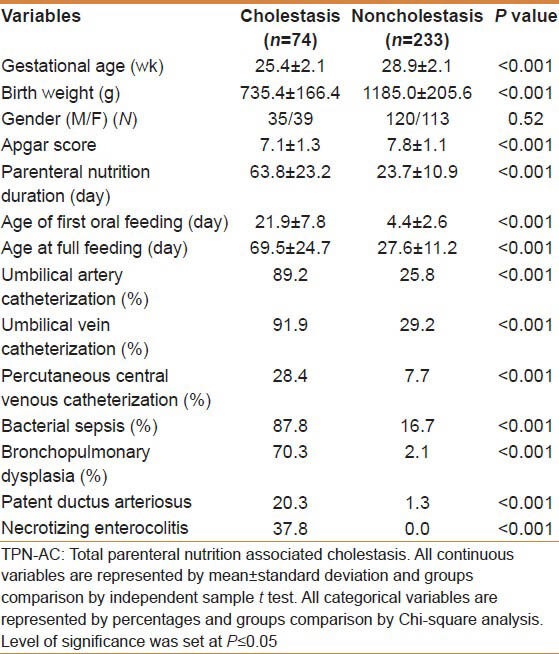
A total of 349 preterm infants were admitted to NICU and received TPN during the study period. Forty-two patients were excluded; 37 subjects expired in the first 10 days of life, 2 patients for missing charts and 3 neonates with significant congenital malformations. The remaining 307 patients were included and their medical records were reviewed. The incidence of cholestasis in the whole population was 24.1% (74 neonates). None of the infants with cholestasis developed end-stage liver disease. The potential risk factors for cholestasis in preterm infants with and without TPN-AC are shown in table 1. The mean GA was 25.4 ± 2.1 week for cholestasis group vs. 28.9 ± 2.1 week for noncholestasis group (P < 0.001), whereas mean Bwt for the two groups were 735.4 ± 166.4 g and 1185.0 ± 205.6 g, respectively (P < 0.001). In the whole cohort, 120 (39%) infants had Bwt <1000 g; 69 (93%) infants were in the the cholestasis group and 51 (22%) infants were in noncholestasis group. The sex ratio did not differ significantly between the two groups (P = 0.52), whereas longer TPN duration, lower AS, higher bacterial septic episodes, delay of first enteral feeding, higher age at full feeds, presence of BPD, PDA, and NEC, and increase in percentage of arterial and venous catheterization were significantly different between the two groups [Table 1].
Table 1.
Clinical characteristics and potential risk factors in preterm infants with and without TPN AC
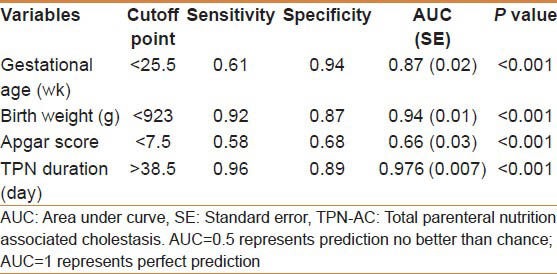
The potential risk factors were then fed into a multivariate logistic regression model. After adjusting for these variables, only the duration of TPN (P < 0.001) and Bwt (P < 0.006) were significantly related to the development of TPN-AC in the study population [Table 2]. The ROC curve analysis was performed to determine the best cutoff values to predict the development of TPN-AC [Table 3]. Receiving TPN for more than the cutoff point of 38.5 days had a sensitivity of 96% and a specificity of 89%, whereas Bwt <923 g had a sensitivity of 92% and a specificity of 87%, which were better than any of the other tested variables.
Table 2.
Multivariate logistic regression analysis for possible predictive risk factors of TPN-AC
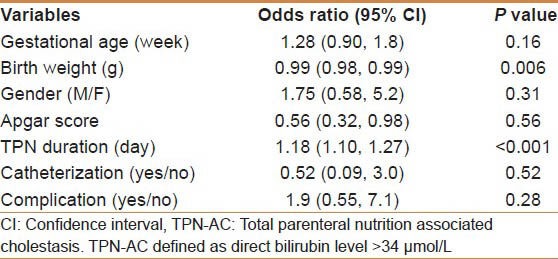
Table 3.
Cutoff points; sensitivity and specificity, for the predictive risk factors of TPN-AC
DISCUSSION
In the present study, we assessed the incidence of TPN-AC and the risk factors for its development. The incidence of cholestasis in the study population was found to be 24.1% when compared with 17.7% previously reported.[14,15] This slight difference in the incidence might be attributed to large number of smaller infants (39%) included in our study in comparison to previous reports.
The Bwt and duration of TPN course were strong predictive risk factors for the occurrence of TPN-AC as previously reported.[4,5,13,14,15,16] However our study, reports for the first time sensitivity and specificity of these predictive risk factors. The ROC curve analysis showed that the duration of TPN >38.5 days and Bwt <923 g were the most significant cutoff values for the development of TPN-AC, which were associated with highest sensitivity and specificity.
The incidence of cholestasis was also affected to a lesser extent by gestational age and AS [Table 3]. These findings are supported by an earlier study, which has shown that the younger the gestational age, the higher is the direct bilirubin concentration.[16] The explanation of this association might be due to the physiological immaturity of the neonatal liver, leading to impaired hepatic transportation and metabolism of bile acids.[12]
There are some limitations of our study. It is an uncontrolled retrospective study with all its known drawbacks. Also, the study had been performed on a cohort of patients approximately 10 years old. Although no significant advances have been made in this period with regard to TPN-AC and its causation, it is difficult to rule out any possible time effects.
Cholestasis and its associated liver dysfunction with prolonged TPN administration is well known, but its pathogenesis is still poorly understood.[17] The development of TPN-AC might be the direct association between the duration of TPN and liver toxicity.[18] The absence of physiological enteral intake may enhance liver damage.[19] Earlier enteral feeding can reserve intestinal integrity, maintain intestinal hormones and enzymes secretion, prevent bacterial translocation, and interrupt the beginning of liver dysfunction that leads to cholestasis.[20]
Several studies have shown that TPN components including lipids are involved in the pathogenesis of both hepatic steatosis and TPN-AC; amino acids were also assumed to be a possible factor responsible for inducing liver dysfunction.[19,21,22] Stigmasterol, a phytosterol that is predominant in soy-derived TPN lipid solutions, suppressed the expression of bile acid homeostatic proteins such as bile salt export pump, fibroblast growth factor,[13] and organic solute transporter α/β.[21] Vileisis et al.[22] have reported that preterm infants who received TPN formulations with higher protein content (3.6 g/kg/day) developed cholestasis earlier than those who received lower protein content (2.5 g/kg/day). Sepsis, a common complication during TPN infusion, may be associated with cholestasis, as previously reported.[15,23] The direct hepatotoxicity caused by endotoxins, as a result of intestinal bacterial overgrowth, might be a possible mechanism of injury. The current data are also in accordance with this notion as the incidence of sepsis was 87.8% in the cholestasis group compared with 16.7% in the noncholestasis group (P < 0.001); however, it did not serve as a predictive risk factor of cholestasis development in our study population.
CONCLUSION
In conclusion, a lower Bwt and longer duration of total parenteral nutrition are strong predictive risk factors for the development of TPN-associated cholestasis in preterm infants.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Naini BV, Lassman CR. Total parenteral nutrition therapy and liver injury: A histopathologic study with clinical correlation. Hum Pathol. 2012;43:826–33. doi: 10.1016/j.humpath.2011.07.008. [DOI] [PubMed] [Google Scholar]
- 2.Buchman AL, Iyer K, Fryer J. Parenteral nutrition-associated liver disease and the role for isolated intestine and intestine/liver transplantation. Hepatology. 2006;43:9–19. doi: 10.1002/hep.20997. [DOI] [PubMed] [Google Scholar]
- 3.Peden VH, Witzleben CL, Skelton MA. Total parenteral nutrition. J Pediatr. 1971;78:180–1. doi: 10.1016/s0022-3476(71)80289-5. [DOI] [PubMed] [Google Scholar]
- 4.Lauriti G, Zani A, Aufieri R, Cananzi M, Chiesa PL, Eaton S, et al. Incidence, prevention, and treatment of parenteral nutrition–associated cholestasis and intestinal failure–associated liver disease in infants and children. A systematic review. JPEN J Parenter Enteral Nutr. 2014;38:70–85. doi: 10.1177/0148607113496280. [DOI] [PubMed] [Google Scholar]
- 5.Spencer AU, Yu S, Tracy TF, Aouthmany MM, Llanos A, Brown MB, et al. Parenteral nutrition-associated cholestasis in neonates: Multivariate analysis of the potential protective effect of taurine. JPEN J Parenter Enteral Nutr. 2005;29:337–44. doi: 10.1177/0148607105029005337. [DOI] [PubMed] [Google Scholar]
- 6.Balistreri WF, Bove KE. Hepatobiliary consequences of parenteral alimentation. Prog Liver Dis. 1990;9:567–601. [PubMed] [Google Scholar]
- 7.Cohen C, Olsen MM. Pediatric total parenteral nutrition. Liver histopathology. Arch Pathol Lab Med. 1981;105:152–6. [PubMed] [Google Scholar]
- 8.Zambrano E, El-Hennawy M, Ehrenkranz RA, Zelterman D, Reyes-Mugica M. Total parenteral nutrition induced liver pathology: An autopsy series of 24 newborn cases. Pediatr Dev Pathol. 2004;7:425–32. doi: 10.1007/s10024-001-0154-7. [DOI] [PubMed] [Google Scholar]
- 9.Mullick FG, Moran CA, Ishak KG. Total parenteral nutrition: A histopathologic analysis of the liver changes in 20 children. Mod Pathol. 1994;7:190–4. [PubMed] [Google Scholar]
- 10.Carter BA, Shulman RJ. Mechanisms of disease: Update on the molecular etiology and fundamentals of parenteral nutrition associated cholestasis. Nat Clin Pract Gastroenterol Hepatol. 2007;4:277–87. doi: 10.1038/ncpgasthep0796. [DOI] [PubMed] [Google Scholar]
- 11.Spagnuolo MI, Iorio R, Vegnente A, Guarino A. Ursodeoxycholic acid for treatment of cholestasis in children on long-term total parenteral nutrition: A pilot study. Gastroenterology. 1996;111:716–9. doi: 10.1053/gast.1996.v111.pm8780577. [DOI] [PubMed] [Google Scholar]
- 12.Chen HL, Chen HL, Liu YJ, Feng CH, Wu CY, Shyu MK, et al. Developmental expression of canalicular transporter genes in human liver. J Hepatol. 2005;43:472–7. doi: 10.1016/j.jhep.2005.02.030. [DOI] [PubMed] [Google Scholar]
- 13.Levine A, Maayan A, Shamir R, Dinari G, Sulkes J, Sirotta L. Parenteral nutrition-associated cholestasis in preterm neonates: Evaluation of ursodeoxycholic acid treatment. J Pediatr Endocrinol Metab. 1999;12:549–53. doi: 10.1515/jpem.1999.12.4.549. [DOI] [PubMed] [Google Scholar]
- 14.Hsieh MH, Pai W, Tseng HI, Yang SN, Lu CC, Chen HL. Parenteral nutrition-associated cholestasis in premature babies: Risk factors and predictors. Pediatr Neonatol. 2009;50:202–7. doi: 10.1016/S1875-9572(09)60064-4. [DOI] [PubMed] [Google Scholar]
- 15.Wu TJ, Teng RJ, Yau KI. Risk factors of cholestasis in very low birth weight infants. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1996;37:278–82. [PubMed] [Google Scholar]
- 16.Beath SV, Davies P, Papadopoulou A, Khan AR, Buick RG, Corkery JJ, et al. Parenteral nutrition-related cholestasis in postsurgical neonates: Multivariate analysis of risk factors. J Pediatr Surg. 1996;31:604–6. doi: 10.1016/s0022-3468(96)90507-2. [DOI] [PubMed] [Google Scholar]
- 17.Suita S, Ikeda K, Nagasaki A, Hayashida Y, Kaneko T, Hamano Y, et al. Follow-up studies of children treated with a long-term intravenous nutrition (IVN) during the neonatal period. J Pediatr Surg. 1982;17:37–42. doi: 10.1016/s0022-3468(82)80322-9. [DOI] [PubMed] [Google Scholar]
- 18.Btaiche IF, Khalidi N. Parenteral nutrition-associated liver complications in children. Pharmacotherapy. 2002;22:188–211. doi: 10.1592/phco.22.3.188.33553. [DOI] [PubMed] [Google Scholar]
- 19.Guglielmi FW, Boggio-Bertinet D, Federico A, Forte GB, Guglielmi A, Loguercio C, et al. Total parenteral nutrition-related gastroenterological complications. Dig Liver Dis. 2006;38:623–42. doi: 10.1016/j.dld.2006.04.002. [DOI] [PubMed] [Google Scholar]
- 20.Takagi K, Yamamori H, Toyoda Y, Nakajima N, Tashiro T. Modulating effects of the feeding route on stress response and endotoxin translocation in severely stressed patients receiving thoracic esophagectomy. Nutrition. 2000;16:355–60. doi: 10.1016/s0899-9007(00)00231-8. [DOI] [PubMed] [Google Scholar]
- 21.Carter BA, Taylor OA, Prendergast DR, Zimmerman TL, Von Furstenberg R, Moore DD, et al. Stigmasterol a soy lipid-derived phytosterol is an antagonist of the bile acid nuclear receptor FXR. Pediatr Res. 2007;62:301–6. doi: 10.1203/PDR.0b013e3181256492. [DOI] [PubMed] [Google Scholar]
- 22.Vileisis RA, Inwood RJ, Hunt CE. Prospective controlled study of parenteral nutrition-associated cholestatic jaundice: Effect of protein intake. J Pediatr. 1980;96:893–7. doi: 10.1016/s0022-3476(80)80573-7. [DOI] [PubMed] [Google Scholar]
- 23.Sondheimer JM, Asturias E, Cadnapaphornchai M. Infection and cholestasis in neonates with intestinal resection and long-term parenteral nutrition. J Pediatr Gastroenterol Nutr. 1998;27:131–7. doi: 10.1097/00005176-199808000-00001. [DOI] [PubMed] [Google Scholar]