

Abstract
Aims and Objectives:
To compare the diagnostic value and accuracy of dry eye scoring system (DESS), conjunctival impression cytology (CIC), tear film breakup time (TBUT), and Schirmer's test in computer users.
Methods:
A case–control study was done at two referral eye centers. Eyes of 344 computer users were compared to 371 eyes of age and sex matched controls. Dry eye questionnaire (DESS) was administered to both groups and they further underwent measurement of TBUT, Schirmer's, and CIC. Correlation analysis was performed between DESS, CIC, TBUT, and Schirmer's test scores. A Pearson's coefficient of the linear expression (R2) of 0.5 or more was statistically significant.
Results:
The mean age in cases (26.05 ± 4.06 years) was comparable to controls (25.67 ± 3.65 years) (P = 0.465). The mean symptom score in computer users was significantly higher as compared to controls (P < 0.001). Mean TBUT, Schirmer's test values, and goblet cell density were significantly reduced in computer users (P < 0.001). TBUT, Schirmer's, and CIC were abnormal in 48.5%, 29.1%, and 38.4% symptomatic computer users respectively as compared to 8%, 6.7%, and 7.3% symptomatic controls respectively. On correlation analysis, there was a significant (inverse) association of dry eye symptoms (DESS) with TBUT and CIC scores (R2 > 0.5), in contrast to Schirmer's scores (R2 < 0.5). Duration of computer usage had a significant effect on dry eye symptoms severity, TBUT, and CIC scores as compared to Schirmer's test.
Conclusion:
DESS should be used in combination with TBUT and CIC for dry eye evaluation in computer users.
Keywords: Computer vision syndrome, conjunctival impression cytology, dry eye scoring system, tear function tests
INTRODUCTION
Gone have those days when computer use was restricted to office work; today, computer usage has extended to teaching at schools and for recreational purpose also.[1] It is needless to say that computers have now become a routine in our day to day life. Excessive use of computers have led to an increase in health-related problems in video display terminal (VDT) users particularly, students and younger age group.[2]
Computer vision syndrome (CVS) refers to ocular and extra-ocular symptoms resulting from prolonged computer usage. Eye-related symptoms are most frequent among VDT users and include eye strain, double vision, fatigue, irritation, redness, burning, and blurring of vision. Non-ocular symptoms include headaches, pain in the shoulders, neck, or back.[3] CVS is increasingly being recognized as a growing public health problem worldwide.[4]
Prolonged visual display terminal tasks reduce blink rate, blink amplitude, and blink quality leading to tear film instability.[5] Therefore, dryness of eyes is common after prolonged computer usage and the prevalence ranges from 30% to 68.5%.[6,7]
Diagnosis of dry eye per se has been a challenging task for ophthalmologists due to poor standardization of routine tear function tests. As a consequence, symptom-based assessment has been a key component of clinical diagnosis in conditions like CVS.[8] Moreover, there is lack of correlation between ocular symptoms and signs observed; patient may not be symptomatic despite abnormal tear function tests and not all symptomatic patients have abnormal tear function tests.[9]
Dryness of the eye is often accompanied by alteration in the morphology of epithelial cells of conjunctiva and reduction in conjunctival goblet cell density (GCD). Conjunctival impression cytology (CIC), a non or minimally invasive technique samples superficial layers of conjunctival and corneal epithelium and has higher sensitivity and specificity, may detect early subtle changes undetected by routine tear function tests; many investigators are of the opinion that it can be the first line investigation for dry eye diagnosis.[10]
Moreover, CVS has essentially been a symptom-based diagnosis and hence the name; role of the tear routine tear functions tests and CIC in diagnosis of CVS related dry eye has not been defined or evaluated extensively. In the present study, we evaluated the significance of dry eye related symptoms following computer use and diagnostic value and accuracy of Schirmer's test, tear film breakup time (TBUT), CIC, and dry eye scoring system (DESS©) in computer users.
METHODS
Patients
A case–control study was done at two referral eye centers from June 2011 to March 2013. The trial was approved by the Institutional Review Boards and the local Ethics Committee. A written informed consent was obtained from all patients willing to participate in the study based on Helsinki protocol.
Inclusion criteria
The target group was software professionals and university/medical students with exposure to VDT and computer-related work during past 6 months in such way that accomplishment of their routine work was not possible without computers. The control group was age and sex matched controls working under similar conditions but their daily work did not involve the use of computers.
Exclusion criteria
Patients using contact lenses, punctual plugs, topical medications such as corticosteroids (6 weeks prior to enrolment), anti-glaucoma drugs and oral anticoagulants were excluded. Pregnant/lactating mothers, postmenopausal women, patients with ocular infection, history of laser in situ keratomileusis, cognitive and psychiatric disorders, lacrimal gland malignancy, and allergy to fluorescein were also excluded.
Ophthalmic examination and measurements
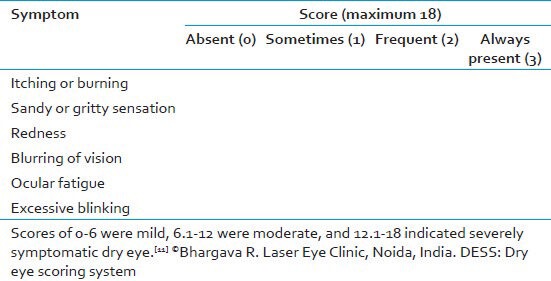
The DESS© was administered to all participants (cases and controls) prior to ophthalmic examination and tests. A score was assigned to common symptoms of dry eye [Table 1]. DESS is assessed on a scale of 0-18 with higher scores representing dry eye severity. A symptom score of 0-6 represents mild, 6.1-12 moderate, and 12.1-18, severe dry eye.[11,12]
Table 1.
Dry eye questionnaire and scoring system (DESS©)
Mean duration of computer usage in cases (computer users) was recorded. Following DESS questionnaire, the subjects had complete ophthalmic examination by an independent investigator (not a study surgeon) and included recording of corrected distance visual acuity, slit-lamp examination; this included an assessment of lid margins, eyelashes, and meibomian gland orifice for any blockage or occlusion.
A single examiner performed all tear function tests including CIC and was masked to information obtained from the questionnaire. One eye was selected at random for examination.
Tear film break up time was first performed as eyelid manipulation may adversely influence the results. Three readings were taken in succession and averaged. A TBUT of <10 s was considered consistent for dry eye.
The subject then waited for 30 min, and Schirmer's test with anesthesia was done with eyes closed. Wetting of the filter paper at 5 min was recorded. Wetting <6 mm was considered consistent with dry eye.
Subjects waited for another 30 min, and CIC was performed after anesthetizing the eye with one drop of 4% Xylocaine. The lacrimal lake at inner canthus was dried with a cotton tip applicator. A circular 0.22 μm filter paper measuring 13 mm in diameter (Sartorius, Germany) was grasped with a blunt tipped forceps and applied over the inferior bulbar conjunctiva. The paper strip was gently pressed with a glass rod held in the other hand. The filter paper was removed in a peeling fashion after 4–10 s and specimen transferred to the lab for staining and fixation. The filter paper was placed on a glass slide with albumin paste for specimen transfer. The slide was labeled and numbered, and then it was stained with periodic acid-Schiff and counterstained with hematoxylin and eosin. The mounted slide was first examined under the microscope with × 10 high power field (HPF). After localization, cells were then analyzed with × 40 HPF magnification. At least 10 HPF were examined for goblet cells and epithelial cells. Grading and scoring were carried out by criteria suggested by Nelson et al.[13] Nelson Grades 0 and 1 were regarded as normal, whereas Grades 2 and 3 were considered to represent abnormal cytology.
Statistical analysis
Statistical analysis was performed using SPSS software for Windows (IBM SPSS Statistics version 18). Means of groups were compared using t-tests. Chi-square tests were used for proportions. A P < 0.05 was considered statistically significant. Correlation analysis was performed between DESS, CIC, TBUT, and Schirmer's test scores. A Pearson's coefficient of the linear expression (R2) of 0.5 or more was statistically significant.
RESULTS
A total of 750 subjects participated in the study. After discarding the poorly stained slides (n = 35), eyes of 344 VDT's and 371 controls were evaluated. The mean age in cases (26.05 ± 4.06 years) was comparable to controls (25.67 ± 3.65 years) (P = 0.465). Overall, there were 354 males and 361 females in both groups combined. The difference between males and females in cases and controls was not significant (P = 0.364 and 0.296, respectively). The mean duration of computer usage was 6.7 ± 2.1 years (range 14 months to 9 years), and mean daily usage was 7.24 ± 2.76 h (range 3-10 h). There was no gender difference between the mean duration of computer use (P = 0.678).
In cases, 93 (27%) were severely symptomatic, 156 (45.3%) moderately, 35 (10.2%) mildly symptomatic, and 60 (17.4%) symptom free. In controls, 15 (4%) were severely symptomatic, 20 (5.4%) moderately symptomatic, 71 (19.1%) mildly symptomatic and 265 (71.4%) symptom free. The mean symptom score in cases and controls was 8.47 ± 3.24 and 2.34 ± 1.24, respectively (P < 0.001). DESS score was significantly higher when daily computer usage was more (P < 0.001).
The mean TBUT in cases and controls [Table 2] was 11.26 ± 1.68 (range 4-14) and 15.68 2.62 (range 8-18) s, respectively (P < 0.001). Mean TBUT scores were significantly less when time spent on computers daily was more (P < 0.001).
Table 2.
Mean characteristics of patients in cases and controls
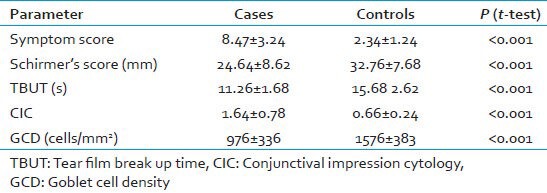
The mean Schirmer's score in cases and controls was 24.64 ± 8.62 (range 5-28) and 32.76 ± 7.68 (range 6-35) mm, respectively (P < 0.001). Mean Schirmer's scores did not correlate significantly with time spent on computers daily amongst cases (P = 0.364).
The mean CIC scores in cases and controls were 1.64 ± 0.78 and 0.66 ± 0.24, respectively (P < 0.001). There was a significant correlation between daily computer usage and mean CIC scores (P = 0.005) among cases. Most computer users had normal (Nelson Grades 0 and 1) CIC (61.6%) after prolonged usage [Figures 1 and 2]. Nelson Grade 2 changes with reduction of GCD and altered epithelial cell morphology predominated (32%) among those having abnormal CIC [Figure 3]. Table 3 shows grade-wise CIC scores in cases and controls.
Figure 1.
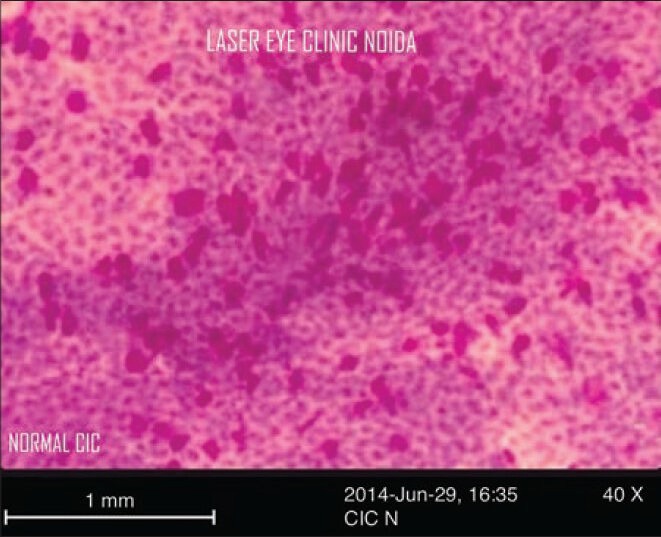
Nelson Grade 0 conjunctival impression cytology specimen showing normal epithelial cells and abundant goblet cells
Figure 2.
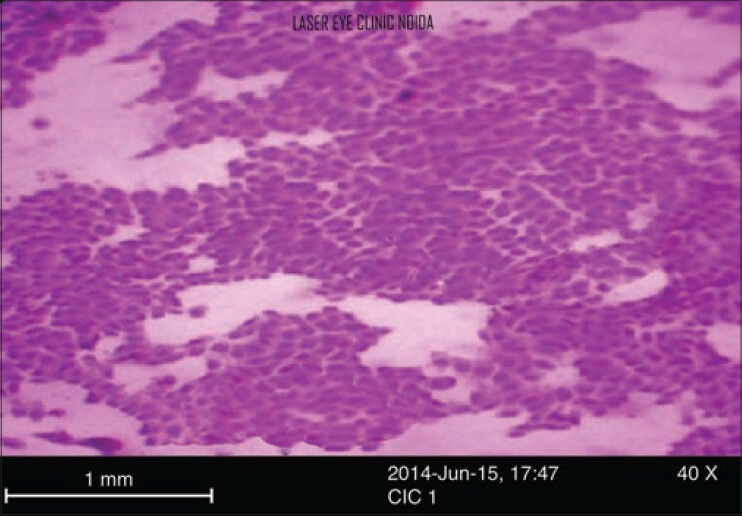
Nelson Grade 1 conjunctival impression cytology specimen with reduced nucleus cytoplasmic ratio and decrease in goblet cell density in dry eye
Figure 3.
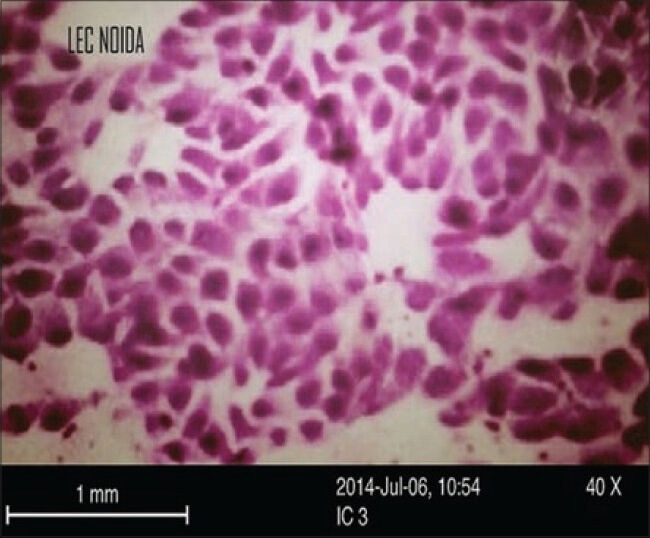
Nelson Grade 2 conjunctival impression cytology specimen, with small nucleus, reduced nucleus cytoplasmic ratio and mild squamous metaplasia in dry eye
Table 3.
Grade wise CIC scores
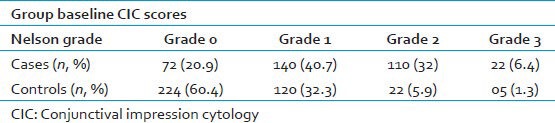
Table 4 shows the percentage of patients with abnormal symptomatology and abnormal tear function tests amongst cases and controls.
Table 4.
Patients with abnormal symptoms and tear function tests in cases and controls

On correlation analysis, DESS correlated significantly (inversely) with TBUT, CIC scores, GCD (R2 > 0.5) and less so with Schirmer's scores (R2 < 0.5) among cases. The correlation was not significant among controls [Table 5, Figures 4–7].
Table 5.
Correlation between symptoms scores and test values in cases and controls
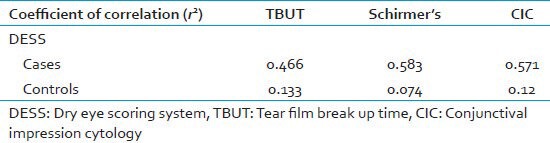
Figure 4.
Scatter diagram showing correlation analysis between dry eye symptoms score and Schirmer's test
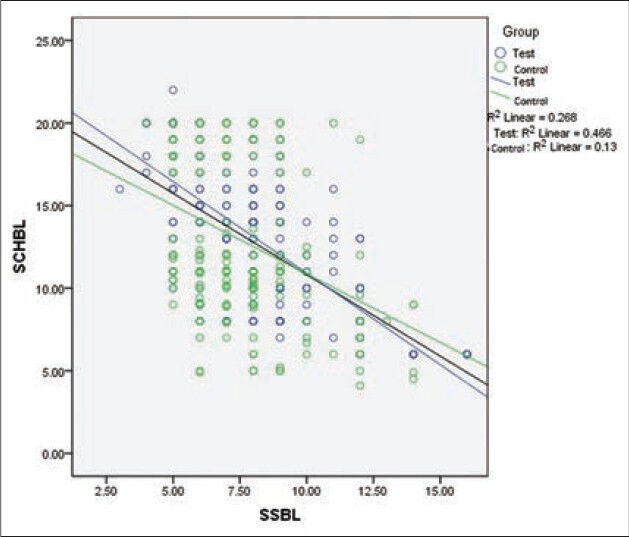
Figure 7.
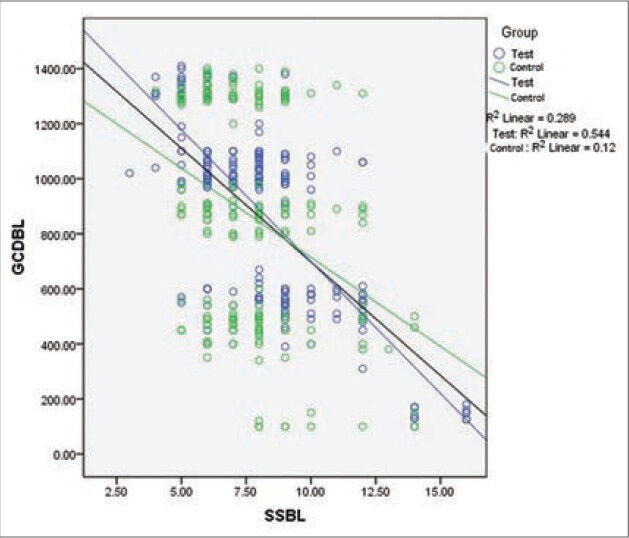
Scatter diagram showing correlation analysis between dry eye symptoms score and goblet cell density
Figure 6.
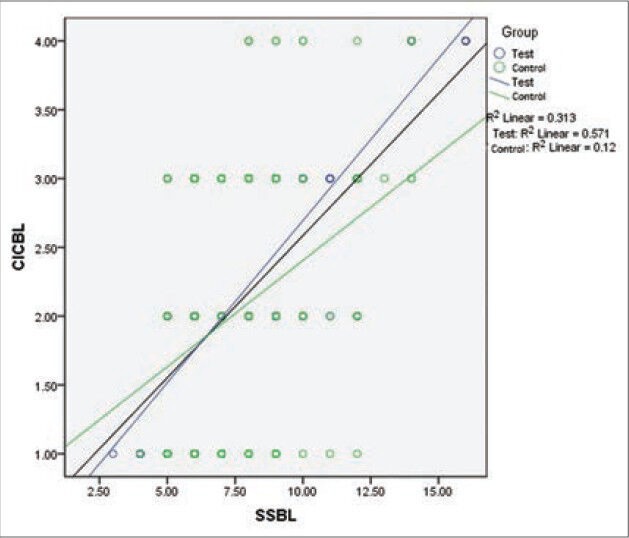
Scatter diagram showing correlation analysis between dry eye symptoms score and conjunctival impression cytology
DISCUSSION
Dryness of eyes is a common problem worldwide and one of the frequent reasons for ophthalmic consultations. The role of personal computers and internet has increased tremendously in our day to day life. Most jobs are now computer dependent, and people have begun to spend more time in front of the computers at work, home, and even at school. Prolonged computer usage is often accompanied by dryness of eyes.[14] CVS adds to the overall burden of dry eye in the community and has now become a significant public health problem.
The aim of the present study was to evaluate the diagnostic value and accuracy of DESS, CIC, and tear function tests such as Schirmer's and TBUT in computer users as compared to controls, for CVS-related dry eye.
Clinical diagnosis of dry eye per se has been a challenging task for ophthalmologists due to poor standardization, unrepeatability, and inaccuracy of routine tear function tests.[15] CIC has not yet become the first-line investigation in dry eye as it is time-consuming and may cause discomfort to some patients. Therefore, symptom-based assessment is a key diagnostic component in CVS and questionnaire-based studies have found a higher prevalence rate of dry eye in computer users. The ocular surface disease index (OSDI) and DESS© are simple and effective tools for symptom-based assessment.[10,16]
In the present study, of 82.5% symptomatic cases, 48.5% had abnormal TBUT, 29.1% abnormal Schirmer's and 38.4% abnormal impression cytology; whereas among 28.5% symptomatic controls, 8% had abnormal TBUT, 6.7% abnormal Schirmer's and 7.3% abnormal cytology; symptom-based assessment may thus be useful for dry eye screening in computer users. A study by Biswas et al. found that TBUT and Schirmer's was abnormal in 40% computer users and was significantly more than the control group. In another study, Schirmer's test was positive in 38.5% computer users as compared to 10.7% controls.[17]
Although the results of the present study sustain the usefulness of questionnaire-based screening for CVS-related dry eye, one important limitation, however, of symptom base screening is that it does not predict the extent of cytological changes in ocular surface and resolution of symptoms alone after dry eye therapy cannot be used as an outcome measure. Thus, symptom-based assessment need be combined with tests like CIC to increase diagnostic accuracy and to effectively monitor response to treatment. For example, a severely symptomatic computer user may have a normal Schirmer's tear and TBUT; but may show early cytological changes in the conjunctiva and cornea on impression cytology. On the contrary, ocular symptoms might not occur despite reduction of tear production. Thus, CIC may be useful under such circumstances and may predict early dry eye changes (undetected by routine tear function tests), so that appropriate measures may be instituted, and development of squamous metaplasia prevented.
In a recent case–control study, Kumar et al. found that with CIC as the gold standard, routine tear function tests like Schirmer's, TBUT and ocular surface staining with dyes like Rose Bengal, were less specific, sensitive and had a lower positive predictive value for diagnosing dry eye; this was further substantiated by the observation that there was a significant reduction in GCD in cases as compared to controls; an observation similar to the present study, with significant reduction in GCD in computer users.[10]
Correlation analysis suggests that symptom-based screening (DESS) correlates well with TBUT, CIC, and GCD but not with Schirmer's test [Figures 2–5]. Second, the present also study suggests that dry eye symptoms may be more severe when duration of daily computer usage was higher. Second, increased mean computer usage was associated with significantly lower TBUT and worst CIC scores (P < 0.001); tear production (Schirmer's), however, was less significantly affected.
Figure 5.
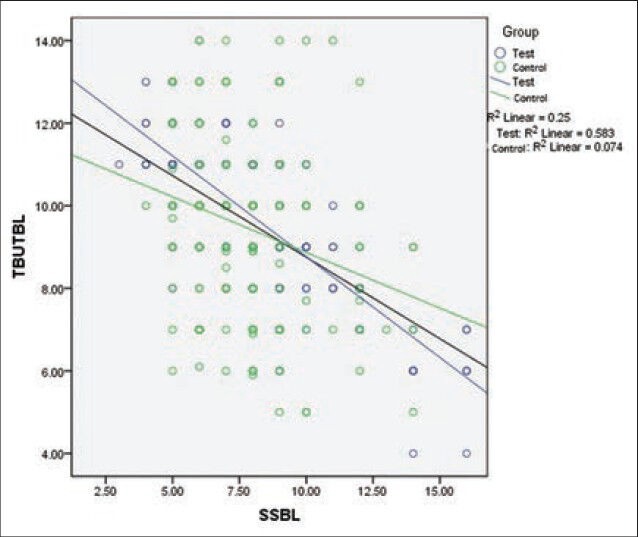
Scatter diagram showing correlation analysis between dry eye symptoms score and tear film break up time
Unlό et al. compared the diagnostic value of Schirmer's test, TBUT and dry eye questionnaire (OSDI) in computer users with dry eye. The authors found that the correlation between OSDI scores and Schirmer's scores was not significant, but there was a significant correlation between OSDI and TBUT scores. The authors also suggested that to strengthen the diagnosis of dry eye, questionnaire-based evaluations should be used and interpreted along with TBUT, an inference similar to the present study.[18] In another study, on 68 eyes with dry eye, Ozcura et al. found a significant inverse correlation of symptom-based screening and TBUT.[19]
Most investigators are of the opinion that the duration of computer usage is directly proportional to dry eye symptoms severity and abnormal tear function tests. In a cross-sectional prevalence study in middle-aged office workers, Uchino, et al. found that >4 h of VDT use was associated with a significantly higher risk of dry eye; an observation, similar to that of the present study.[20] Another cross-sectional study estimating prevalence of dry eye disease in VDT users, using logistic regression analysis found increased dry eye risk in workers using a VDT >8 h/day (OR = 1.94; 95% CI, 1.22-3.09).[21] Tear function tests revealed short TBUT and corneal staining; however, Schirmer test values were normal (78.6% of study participants had TBUT ≤ 5 s).
Although dryness of the eye has been more prevalent elderly women, preponderance of dry eye in young patients in present study highlights the increasing impact of computers on dry eye related symptoms.[22] In a study to estimate the prevalence of CVS among university students in Malaysia, Reddy et al. found that 90% of students were symptomatic when computer usage was more than 2 h/day.[23]
Thus, duration of computer usage per day may be significantly associated with increased dry eye symptoms severity and deranged TBUT an (indirect measure of tear film stability) and CIC scores, despite relatively normal Schirmer's test (a measure of tear production). Due to these challenges in diagnosing computer use related dry eye, clinician should evaluate ocular symptoms, signs, and tests results together. Thus, it is important that the questionnaire-based dry eye evaluation (DESS) in patients with CVS may be used in combination with TBUT and CIC for diagnosis of CVS associated dry eye.
CONCLUSION
Dry eye scoring system, CIC, and TBUT correlate well and may hold good diagnostic accuracy, may detect early dry eye changes, when used in combination for diagnosis of dry eye in computer users.
ACKNOWLEDGMENT
The authors would like to thank Dr. Puneet Gupta for statistical analysis.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.United States Census Bureau. 2014. [Last accessed on 2014 Jun 26]. Available from: http://www.census.gov/cps/methodology/techdocs.html .
- 2.Portello JK, Rosenfield M, Chu CA. Blink rate, incomplete blinks and computer vision syndrome. Optom Vis Sci. 2013;90:482–7. doi: 10.1097/OPX.0b013e31828f09a7. [DOI] [PubMed] [Google Scholar]
- 3.Blehm C, Vishnu S, Khattak A, Mitra S, Yee RW. Computer vision syndrome: A review. Surv Ophthalmol. 2005;50:253–62. doi: 10.1016/j.survophthal.2005.02.008. [DOI] [PubMed] [Google Scholar]
- 4.Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Impact of dry eye syndrome on vision-related quality of life. Am J Ophthalmol. 2007;143:409–15. doi: 10.1016/j.ajo.2006.11.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cardona G, García C, Serés C, Vilaseca M, Gispets J. Blink rate, blink amplitude, and tear film integrity during dynamic visual display terminal tasks. Curr Eye Res. 2011;36:190–7. doi: 10.3109/02713683.2010.544442. [DOI] [PubMed] [Google Scholar]
- 6.Apostol S, Filip M, Dragne C, Filip A. Dry eye syndrome. Etiological and therapeutic aspects. Oftalmologia. 2003;59:28–31. [PubMed] [Google Scholar]
- 7.Uchino M, Schaumberg DA, Dogru M, Uchino Y, Fukagawa K, Shimmura S, et al. Prevalence of dry eye disease among Japanese visual display terminal users. Ophthalmology. 2008;115:1982–8. doi: 10.1016/j.ophtha.2008.06.022. [DOI] [PubMed] [Google Scholar]
- 8.Nakaishi H, Yamada Y. Abnormal tear dynamics and symptoms of eyestrain in operators of visual display terminals. Occup Environ Med. 1999;56:6–9. doi: 10.1136/oem.56.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23:762–70. doi: 10.1097/01.ico.0000133997.07144.9e. [DOI] [PubMed] [Google Scholar]
- 10.Kumar P, Bhargava R, Kumar M, Ranjan S, Kumar M, Verma P. The correlation of routine tear function tests and conjunctival impression cytology in dry eye syndrome. Korean J Ophthalmol. 2014;28:122–9. doi: 10.3341/kjo.2014.28.2.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhargava R, Kumar P, Kumar M, Mehra N, Mishra A. A randomized controlled trial of omega-3 fatty acids in dry eye syndrome. Int J Ophthalmol. 2013;6:811–6. doi: 10.3980/j.issn.2222-3959.2013.06.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kumar P, Bhargava R, Kumar M, et al. Dry Eye Syndrome: A diagnostic enigma. International Journal of Contemporary Surgery. 2013;1(2):72–77. [Google Scholar]
- 13.Nelson JD, Havener VR, Cameron JD. Cellulose acetate impressions of the ocular surface. Dry eye states. Arch Ophthalmol. 1983;101:1869–72. doi: 10.1001/archopht.1983.01040020871007. [DOI] [PubMed] [Google Scholar]
- 14.Shantakumari N, Eldeeb R, Sreedharan J, Gopal K. Computer use and vision-related problems among university students in Ajman, United Arab emirate. Ann Med Health Sci Res. 2014;4:258–63. doi: 10.4103/2141-9248.129058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fuentes-Páez G, Herreras JM, Cordero Y, Almaraz A, González MJ, Calonge M. Lack of concordance between dry eye syndrome questionnaires and diagnostic tests. Arch Soc Esp Oftalmol. 2011;86:3–7. doi: 10.1016/j.oftal.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 16.Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118:615–21. doi: 10.1001/archopht.118.5.615. [DOI] [PubMed] [Google Scholar]
- 17.Biswas NR, Nainiwal SK, Das GK, Langan U, Dadeya SC, Mongre PK, et al. Comparative randomized controlled clinical trial of a herbal eye drop with artificial tear and placebo in computer vision syndrome. J Indian Med Assoc. 2003;101:208–9. 212. [PubMed] [Google Scholar]
- 18.Unlü C, Güney E, Akçay Bİ, Akçalı G, Erdoğan G, Bayramlar H. Comparison of ocular-surface disease index questionnaire, tear film break-up time, and Schirmer tests for the evaluation of the tear film in computer users with and without dry-eye symptomatology. Clin Ophthalmol. 2012;6:1303–6. doi: 10.2147/OPTH.S33588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ozcura F, Aydin S, Helvaci MR. Ocular surface disease index for the diagnosis of dry eye syndrome. Ocul Immunol Inflamm. 2007;15:389–93. doi: 10.1080/09273940701486803. [DOI] [PubMed] [Google Scholar]
- 20.Uchino M, Yokoi N, Uchino Y, Dogru M, Kawashima M, Komuro A, et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The Osaka study. Am J Ophthalmol. 2013;156:759–66. doi: 10.1016/j.ajo.2013.05.040. [DOI] [PubMed] [Google Scholar]
- 21.Dehghani A, Tavakoli M, Akhlaghi M, Naderi A, Eslami F. Prevalence of ocular symptoms and signs among professional computer users in Isfahan, Iran. J Res Med Sci. 2008;13:303–7. [Google Scholar]
- 22.Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry eye syndrome among US women. Am J Ophthalmol. 2003;136:318–26. doi: 10.1016/s0002-9394(03)00218-6. [DOI] [PubMed] [Google Scholar]
- 23.Reddy SC, Low CK, Lim YP, Low LL, Mardina F, Nursaleha MP. Computer vision syndrome: A study of knowledge and practices in university students. Nepal J Ophthalmol. 2013;5:161–8. doi: 10.3126/nepjoph.v5i2.8707. [DOI] [PubMed] [Google Scholar]