

Abstract
Sales of caffeine-containing energy drinks (CCEDs) have increased rapidly since their introduction to the marketplace. Despite the health concerns raised about highly caffeinated CCEDs, surprisingly little data are available to estimate the prevalence of use. This paper presents the results of secondary data analyses of a nationally representative dataset of US schoolchildren. Approximately one-third of students are recent CCED users with substantial variation by age, sex, and race/ethnicity. Among the health and safety concerns related to CCED use is the possibility of potentiation of risk-taking behaviors. A review of the research reveals that although there appears to be a strong and consistent positive association between CCED use and risk-taking behavior, all but one study have used cross-sectional designs, limiting their ability to make inferences about the temporal nature of the association. More research is needed to understand the nature of this association and how CCEDs might impact adolescent health and safety, especially given the high prevalence of use among youth.
Keywords: caffeine, energy drinks, energy shots
INTRODUCTION
Although no formal definition has been proposed, beverages labeled and marketed as energy drinks comprise a heterogeneous beverage category, most of which contain caffeine and a variety of other ingredients, including guarana, taurine, and B vitamins.1,2 Several types of caffeine-containing energy drinks (CCEDs) are carbonated and contain sugar,3,4 although sugar-free variations are available.5 Public health concerns have been raised primarily because of the high levels of caffeine in these beverages, both in amount and in concentration. The amount of caffeine varies considerably among CCEDs, ranging from 50 to 500 milligrams per container,6 with some containers containing more than a single serving.7 Energy shots come in smaller-sized containers, typically less than three ounces. The caffeine concentration in energy shots differs by product, with some products containing in excess of 100 milligrams per fluid ounce.6 Currently no maximal limit on caffeine is imposed by the US Food and Drug Administration for either CCEDs or energy shots. In contrast, the maximal limit on caffeine in a cola-type beverage is 71 milligrams per 12 ounce serving.8
CCEDs were first introduced to the US marketplace in the late 1990s, and since then there has been rapid growth in both the number of different types of products available and the varieties within a particular brand.6 Industry data indicate that CCEDs and energy shots constitute one of the fastest growing segments of the beverage market, with sales in the US expected to increase from $12.5 billion in 2012 to $21.5 billion in 2017.9
Along with the rise in popularity of CCEDs has been an increase in reports of emergency department visits related to CCED use. Namely, from 2007 to 2011, there was an estimated two-fold increase in the number of individuals presenting to emergency departments after consuming a CCED, from 10,068 in 2007 to 20,783 in 2011.10 A majority of these individuals were between 18 and 39 years old, with 42% using a substance in addition to a CCED. In 2011, 1,499 adolescents ages 12 to 17 were admitted to the emergency department following consumption of a CCED. Multiple cases in which consumption of CCEDs resulted in hospitalization have been reported voluntarily to the US Food and Drug Administration’s Center for Food Safety and Applied Nutrition Adverse Event Reporting System.11,12 Data on hospitalizations resulting from CCED use are not systematically collected. Recent concerns about possible cardiovascular effects from high levels of caffeine in CCEDs have been raised in the scientific literature.7,13–16 More generally, the American Academy of Pediatrics has raised safety concerns about the inclusion of CCEDs in the diets of children,17 and the American Medical Association issued a resolution to ban the marketing of CCEDs to individuals under the age of 18.18
Data to describe consumption patterns among the US population are scarce. Federally-funded US national epidemiologic surveys that track annual trends in health behaviors and nutritional habits among adults and children have included very few questions about CCED consumption. In 2010, the National Health Interview Survey included a supplement containing one question on CCEDs: “During the past month, how often did you drink sports and energy drinks, such as Gatorade®, Red Bull®, and Vitamin Water®?”19 To our knowledge, there have been no published reports of these data. The National Health and Nutrition Examination Survey accepts entries of CCEDs as part of a 24-hour dietary recall on beverages, and provides example cards of energy beverages, but does not specifically inquire about their consumption.20
One of the most widely used surveys to measure the health-risk behaviors of American school children is the NIH-funded Monitoring the Future (MTF) Survey, which began asking about CCEDs in 2010. Estimates of consuming alcohol containing caffeine are available in the MTF reports since 2011 and indicated that 10.9%, 19.7%, and 26.4% of eighth, tenth, and twelfth graders consumed caffeinated alcoholic beverages during the past year, respectively.21 For college students and young adults ages 19 to 28, these estimates are even higher (33.8% and 36.7%, respectively). Although the data are publicly available, the annual MTF reports have not included estimates of consuming CCEDs and energy shots without alcohol. An analysis of MTF data on CCEDs and energy shots by Terry-McElrath, O’Malley, and Johnston22 found an association between CCED and energy shot frequency and substance use; however, that study analyzed CCED and energy shot use as one variable, rather than analyzing use of the products separately. Additionally, that study did not describe subgroup variation of CCED or energy shot use by race or grade level, and did not report data on quantity of CCEDs consumed.
It is important to understand the extent to which CCEDs are becoming a part of the adolescent and young adult diet. The nutritional requirements of adolescence, defined as the period between the ages of 13 and 18, is marked by complex hormonal changes that result in pubertal development and growth. The rapid physical growth that occurs during this period requires the increased intake of calories, protein, vitamins, and minerals.23 Future eating patterns are often established during adolescence, making this a critical period with lifelong nutritional implications.24
To our knowledge, no research has specifically focused on the potential effects of caffeine consumption on physical growth and development during childhood and adolescence. However, the effects of caffeine use on disrupted sleep patterns are well recognized.25 Interestingly, daytime sleepiness related to caffeine and other substance use has been shown to be related to poor academic performance among a large sample of adolescents.26 A laboratory study of caffeine use during a critical developmental period has shown a relationship between caffeine administration and decreases in sleep quality and brain maturation.27
In addition to the attention raised about possible cardiovascular effects of consuming high levels of caffeine in CCEDs,7,13–16 other research studies have pointed to an association between CCED consumption and different types of risk-taking behavior among adolescents and young adults. Adolescence is a peak developmental period for risk-taking, which many believe is normative and biologically-driven.28 New research in the field of developmental neuroscience has shed light on the complex structural and functional changes that take place in the brain from adolescence through the early 20s.29–35 These changes might explain why adolescents are more likely than older individuals to take risks without regard for possible consequences and why there might be an inherent reliance on peers when making decisions.
Because of the pharmacologic stimulating properties of caffeine, it is possible that CCEDs might potentiate the risk-taking behavior that is normative to adolescent development. At least two non-mutually exclusive mechanisms have been suggested to explain the relationship between energy drinks and substance use. First, from a biological perspective, through its interaction with dopamine, early caffeine use could potentially prime neural reward circuitry such that the individual experiences a more positive response to other drugs.36,37 Supporting this hypothesis is evidence suggesting cross-sensitization between caffeine and nicotine.38 Second, consumers of energy drinks might be more likely to use other drugs because of an underlying general propensity for risk-taking.
In this paper, we report prevalence estimates of CCED and energy shot use by grade, gender, and race/ethnicity from secondary data analyses of the MTF dataset. We complement these findings with a summary of results from studies utilizing college student and adult samples. The second purpose of this paper is to summarize research on the link between CCED use and various forms of risk-taking behavior.
CCED USE DURING ADOLESCENCE: FINDINGS FROM THE MONITORING THE FUTURE (MTF) SURVEY
Data from MTF are available for public use via the National Addiction and HIV Data Archive Program.39 To estimate the prevalence of CCED consumption, we analyzed data from the 2010 and 2011 surveys, the most recent data available. These secondary data analyses were approved by the University of Maryland Institutional Review Board. MTF is a cross-sectional paper-and-pencil survey administered annually to eighth, tenth, and twelfth graders attending more than 100 public and private schools across the 48 contiguous states.40 Multistage random sampling occurs first at the level of geographic areas, or “primary sampling units”; next at the school level within each selected geographic area; and finally at the class level within each selected school. Surveys are then self-administered to all students in selected classrooms (or the entire school, for smaller schools). Due to the large number of topics assessed, several alternative forms of the MTF questionnaire are developed each year (i.e., six for twelfth graders; four for eighth and tenth graders), with each form containing only a subset of all possible questionnaire items. Forms are distributed randomly, and the resulting subsamples show no significant differences.
Response rates for the 2011 survey ranged from 83% for twelfth graders to 91% for eighth graders.40 Data were downloaded from the National Addiction and HIV Data Archive Program and analyzed in SPSS41 to estimate the prevalence of CCED use and examine variation in prevalence estimates by grade, gender, and race/ethnicity. Standard weighting procedures were used to adjust for differences in selection probabilities at each level of the sampling design (i.e., students, schools, and geographic areas) by assigning a sampling weight, provided in the dataset, for each respondent.42 Valid data from 2011 on CCEDs and/or energy shots were available for 5,207 eighth graders, 4,965 tenth graders, and 2,209 twelfth graders (weighted sample sizes). Analyses were replicated using data collected in 2010 from separate samples of comparable size (5,036 eighth graders, 5,089 tenth graders, and 2,142 twelfth graders); however, for ease of presentation, comparisons across demographic subgroups are presented herein for 2011 data only.
The questionnaire provided participants with the following background information: “‘Energy drinks’ are non-alcoholic beverages that usually contain high amounts of caffeine, including such drinks as Red Bull®, Full Throttle®, Monster®, and Rockstar®. They are usually sold in 8- or 16-ounce cans or bottles” and “Energy drinks are also sold as small ‘shots’ that usually contain just 2 or 3 ounces.” The questionnaire did not differentiate between sugar-containing and sugar-free CCEDs. Ordinal responses to the original survey question, “About how many (if any) energy drinks do you drink per day on average?” were recoded into a three-level categorical variable representing daily use (“One”, “Two”, “Three”, “Four”, “Five or six”, and “Seven or more” per day), less than daily use (“Less than one” per day), and non-use (“None”). No time frame was specified in the original question; therefore, we operationalized current use as encompassing both daily use and less than daily use. Similar procedures were used for energy shots.
Figure 1a displays the 2011 prevalence estimates of CCED use by gender and race/ethnicity for eighth, tenth, and twelfth graders. Overall, 35% of eighth graders and 29% of both tenth and twelfth graders indicated that they used CCEDs. One striking observation is that eighth graders were more likely to consume CCEDs compared with tenth and twelfth graders. For every grade, males were more likely than females to use CCEDs. Black individuals had the lowest prevalence of CCED use regardless of grade. The highest prevalence was observed among Hispanic eighth graders (43%), and the lowest among Black twelfth graders (19%).
Figure 1.

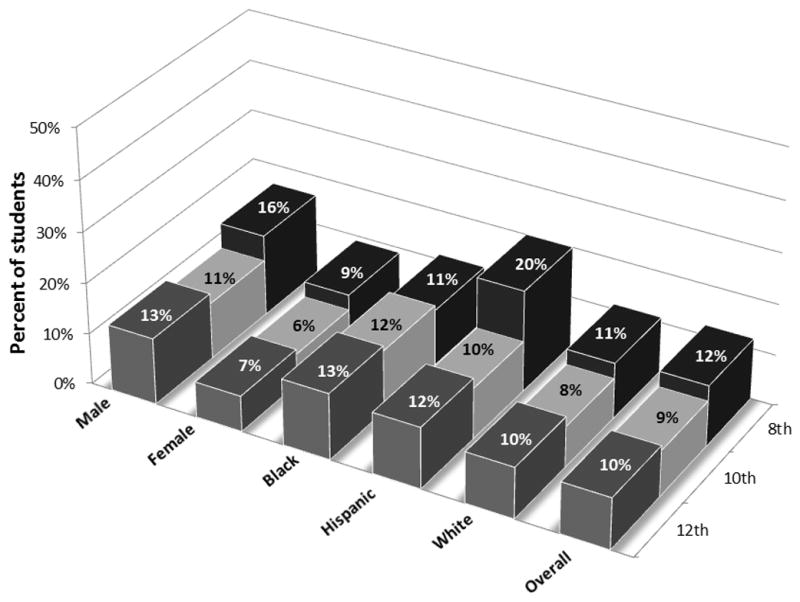
Figure 1a Prevalence of recent CCED use, by gender, race/ethnicity, and grade.
Figure 1b Prevalence of recent energy shot use, by gender, race/ethnicity, and grade.
Figure 1b presents similar data related to energy shot consumption. Overall, the consumption of energy shots was less prevalent than for CCEDs, with 12%, 9%, and 10% of eighth, tenth, and twelfth graders using energy shots, respectively. While gender differences were similar to what was observed for CCEDs, racial/ethnic variations were less apparent. However, Hispanic eighth graders stood out as having a particularly high prevalence (20%) relative to all other subgroups.
Because questions on CCEDs and energy shots were asked separately, it was possible to examine what proportion of students consumed both types of products. As shown in the lowest layer of bars in Figure 2, between 8% and 12% of students consumed both CCEDs and energy shots. Interestingly, almost all energy shot users also consumed CCEDs. Between 20% and 24% consumed CCEDs, but not energy shots, as shown in the highest layer of bars. It is also noteworthy that there is considerable consistency in the results from 2010 to 2011.
Figure 2.
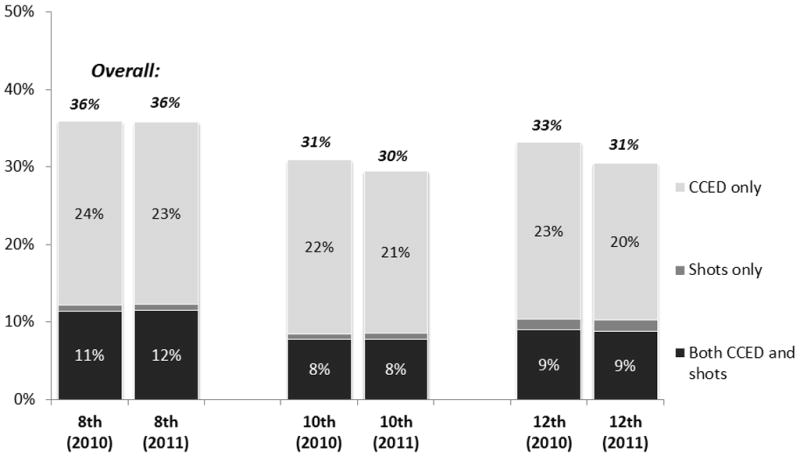
Prevalence of recent use of CCEDs and/or shots, by grade and year.
Table 1 shows data on the daily use of CCEDs and energy shots. Eighth graders showed the highest prevalence of daily use for both CCEDs (18%) and energy shots (7%). Consistent with results from Figures 1a and 1b, Hispanic eighth graders stood out again as the subgroup with the highest prevalence of daily use of CCEDs (22%) and energy shots (11%).
Table 1.
Prevalence of daily use of CCEDsa and energy shots by grade.
| CCED | Energy shots | |||
|---|---|---|---|---|
| 2010 | 2011 | 2010 | 2011 | |
| Eighth graders | 18.5 | 17.7 | 6.4 | 6.9 |
| Males | 22.5 | 20.1 | 7.6 | 8.5 |
| Females | 15.1 | 15.2 | 5.1 | 5.3 |
| White | 17.2 | 15.7 | 4.9 | 5.5 |
| Black | 17.3 | 21.1 | 6.1 | 7.7 |
| Hispanic | 22.4 | 22.3 | 9.5 | 11.0 |
| Tenth graders | 13.6 | 11.5 | 4.2 | 4.5 |
| Males | 16.9 | 14.1 | 5.6 | 5.7 |
| Females | 10.0 | 9.1 | 2.8 | 3.4 |
| White | 12.5 | 11.0 | 3.3 | 3.7 |
| Black | 14.6 | 12.8 | 7.4 | 7.6 |
| Hispanic | 16.1 | 12.5 | 4.8 | 5.5 |
| Twelfth graders | 12.2 | 9.6 | 4.3 | 4.2 |
| Males | 14.8 | 11.6 | 6.0 | 4.7 |
| Females | 8.7 | 7.7 | 2.2 | 3.6 |
| White | 12.1 | 8.6 | 2.8 | 3.7 |
| Black | 9.6 | 7.8 | 5.6 | 7.5 |
| Hispanic | 10.2 | 13.9 | 6.9 | 4.7 |
Caffeine-containing energy drink
Among individuals who consumed these products, most drank only one or less than one per day (see Table 2). Although individuals who drank two or more per day were in the minority, their proportion decreased with age, similar to the trends observed in prevalence of use and daily use. For instance, 24% of CCED consumers in the eighth grade were drinking two or more per day, compared with 16% and 13% of their counterparts in tenth and twelfth grade, respectively. This trend was evident in all six of the subgroups we examined, but was perhaps most pronounced among Hispanics, with nearly a three-fold difference in two-a-day use between eighth and twelfth graders (30% vs. 11% drinking two or more CCEDs per day). On the other hand, two-a-day use was most prevalent among Black eighth graders (33%). The age-related decrease in quantity consumed was less consistent for energy shot users. In at least two subgroups—namely, females and Blacks—the proportion of energy shot users drinking two or more shots per day changed very little with age.
Table 2.
Number of CCEDsa and energy shots consumed per day, among users, by sex, race, and grade.
| Male | Female | Black | White | Hispanic | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 8th | 10th | 12th | 8th | 10th | 12th | 8th | 10th | 12th | 8th | 10th | 12th | 8th | 10th | 12th | 8th | 10th | 12th | |
| Number of CCEDsa/day | ||||||||||||||||||
| <1 | 48.9 | 58.7 | 66.8 | 50.7 | 61.3 | 67.2 | 35.9 | 47.4 | 57.8 | 53.8 | 64.1 | 71.3 | 47.6 | 53.6 | 56.5 | 50.1 | 60.6 | 67.5 |
| 1 | 26.3 | 24.0 | 19.9 | 25.1 | 22.7 | 17.6 | 31.2 | 26.2 | 21.1 | 25.8 | 22.0 | 16.9 | 22.8 | 26.6 | 32.1 | 25.8 | 23.2 | 19.9 |
| 2 or more | 24.8 | 17.3 | 13.3 | 24.2 | 16.0 | 15.2 | 33.0 | 26.4 | 21.2 | 20.4 | 13.9 | 11.7 | 29.5 | 19.8 | 11.4 | 24.1 | 16.2 | 12.5 |
| Number of energy shots/day | ||||||||||||||||||
| <1 | 45.4 | 49.1 | 64.9 | 43.1 | 44.5 | 50.3 | 33.1 | 34.5 | 42.8 | 47.5 | 53.3 | 63.2 | 44.8 | 43.7 | 60.7 | 44.8 | 48.2 | 59.3 |
| 1 | 21.5 | 21.6 | 18.3 | 26.1 | 25.1 | 18.4 | 20.1 | 24.3 | 15.8 | 26.1 | 26.6 | 20.4 | 20.2 | 8.5 | 17.5 | 23.5 | 22.7 | 19.1 |
| 2 or more | 33.0 | 29.3 | 16.8 | 30.8 | 30.4 | 31.3 | 46.8 | 41.2 | 41.4 | 26.4 | 20.0 | 16.4 | 35.0 | 47.8 | 21.8 | 31.6 | 29.0 | 21.6 |
Caffeine-containing energy drink
PREVALENCE AMONG COLLEGE STUDENTS
The prevalence of CCED use among college students is presented in Table 3. As can be seen, CCED use varies substantially among the samples studied, primarily because of the different time frames used to assess consumption. Both Arria et al.43 and Miller44 reported that 10% of college students in their samples were “weekly” consumers. Others reported higher estimates for weekly consumption.45 In a study about CCED consumption patterns Malinauskas et al.5 found that 51% of college students consumed more than one CCED each month in an average month during the past semester. Across the various studies, even with the differences in methodology, CCED use appears to be even more common among college students than younger adolescents.
Table 3.
Summary of studies on the relationship between CCEDa use and risk behaviors.
| Authors | Sample | Study design | CCED prevalence | Risk behaviors studied | Results |
|---|---|---|---|---|---|
| Arria et al. (2010)39 | n=1,060 college students | Prospective | Typical use: 23% (Year 2), 36.5% (Year 3) | Incident use of eight drugs | CCED use associated with incident nonmedical prescription drug use and frequency of tobacco smoking.* |
| Arria et al. (2011)34 | n=975 college students | Cross-sectional | Past-year use: 51% less than weekly 10% weekly use | Alcohol use and related problems, alcohol dependence | CCED use associated with alcohol dependence.* |
| Miller (2008)35 | n=602 college students | Cross-sectional | Past-month use: 38% | Marijuana, tobacco, alcohol, and prescription drug use, sexual risk- taking, seat belt omission | CCED use associated with risk-taking; race/ethnicity difference existed. |
| Miller et al. (2011)38 | n=226 musicians ages18 to 45 | Cross-sectional | Past-year use: 57% | Marijuana, psychedelic drug, cocaine, prescription drug, and tobacco use, binge drinking, and alcohol-related problems | CCED use associated with prescription drug misuse, binge drinking, and social problems related to alcohol use.* |
| Peacock et al. (2013)42 | n=28 young adults ages 18 to 25 | Experimental, within subjects | N/A | Laboratory measure of risk-taking | Small but significant relationship between CCED condition and risk- taking task. |
| Skewes et al. (2013)36 | n=298 college students | Cross-sectional | 39% weekly use | Hazardous alcohol use, alcohol-related problems, symptoms of alcohol dependence, alcohol use motives | CCED use associated with hazardous alcohol use, alcohol-related problems, alcohol dependence, and coping and enhancement motives. |
| Spierer et al. (2014)52 | n=407 college and graduate students | Cross-sectional | 21% high users (at least three times a week) | Risky driving behaviors, tobacco, anabolic steroid, and illicit drug use, and sports-related risks | CCED use associated with increased likelihood of driving after drinking to inebriation and riding with a drunk driver. |
| Stasio et al. (2011)41 | n=107 college students | Cross-sectional | Past-week use: 57% | Anxiety, sleep quality | CCED use accounted for 29% and 20% of variance in anxiety and sleep quality, respectively.* |
| Trapp et al. (2014)47 | n=1,234 young adults ages 18 to 22 | Cross-sectional | 48% monthly use | Alcohol, cigarette, and illicit drug use | Monthly CCED use associated with increased alcohol quantity, being a cigarette smoker, use of ecstasy and marijuana, and the count of illicit drugs used. |
| Velazquez et al. (2012)37 | n=585 underclassmen college students | Cross-sectional | Past-month use: 40% Past week use: 18% | Alcohol use, heavy drinking, mixing alcohol and CCED | CCED use associated with greater risk of all behaviors studied. |
| Woolsey et al. (in press)40 | n=267 college and graduate students | Cross-sectional | Past-year use: 83% | Nonmedical use of prescription stimulants | CCED use was significantly associated with nonmedical prescription stimulant use. |
Caffeine-containing energy drink
controlled for other types of caffeine use
RELATIONSHIP BETWEEN CCED USE AND RISK-TAKING BEHAVIORS AMONG COLLEGE STUDENTS
Several observational studies and one experimental study have examined the association between CCED use and various types of risk-taking behaviors (see Table 3). All of the studies were conducted among college students and young adults, except for one study of 18- to 45-year-old musicians. All but one of the studies have gathered data using cross-sectional survey designs, where questions about CCED consumption were asked along with questions about risk-taking behaviors. The results of these studies are consistent and clearly show that CCED users are more likely to engage in risk-taking behavior.
Many forms of risk-taking behavior have been investigated, including marijuana, tobacco, other forms of drug use, sexual risk-taking, and seat belt omission. CCED consumption, regardless of mixing with alcohol at the time of consumption, has been associated with alcohol-related outcomes. In a study of 298 college students, Skewes et al.45 found a positive association between the typical number of CCEDs consumed per week and measures of alcohol dependence, current symptoms of alcohol dependence, and alcohol-related problems when controlling for age, gender, and frequency of binge drinking. Specifically, CCED consumption was positively associated with scores on the Alcohol Use Disorders Identification Test (a screening tool used to identify hazardous drinking), the Young Adult Alcohol Consequences Questionnaire (a measure of alcohol-related problems), and the Short Alcohol Dependence Data questionnaire (a measure of current alcohol dependence symptoms). Typical CCED frequency was also associated with two types of alcohol use motives: enhancement motives (i.e., drinking for enjoyment or for fun) and coping motives (i.e., drinking to forget one’s problems).
Arria et al.43 found a positive relationship between the frequency of CCED use and risk for alcohol dependence among college students, even after statistical adjustment for the level of alcohol consumption (i.e., typical quantity) and a wide range of background variables and other known risk factors for alcohol dependence, including sensation-seeking, conduct problems before the age of 18, the age of first alcohol intoxication, depressive symptoms, and parental history of alcohol problems. Demographic variables also included in the model were sex, race/ethnicity, socioeconomic status, and involvement in a fraternity or sorority. Also unique to this study was that use of other caffeinated products was measured and used as a covariate in the analyses. The breadth of variables included in this model was important because it points to the possibility that CCED use and alcohol dependence might be interrelated in a meaningful way, rather than merely co-occurring due to shared risk factors such as a general propensity to drink more alcohol.
Another study of college students reported that approximately one third of past-month CCED users had mixed CCEDs and alcohol during the past month.46 CCED use frequency was also associated with alcohol quantity consumed during a single event. A study of Australian young adults47 also found that alcohol quantity was associated with consuming CCEDs at least monthly. In another study, Miller44 found that CCED frequency and alcohol problems were positively associated for White but not Black undergraduates.
A study of musicians ages 18 to 45 found that the frequency of CCED consumption was positively associated with binge drinking and alcohol-related social problems, even when controlling for demographic variables, sensation-seeking, impulsivity, and other types of caffeine use.48
Other substance use has also been associated with the consumption of CCEDs, including marijuana, tobacco, and nonmedical use of prescription drugs.44,48–50 Woolsey et al.50 found that past-month frequency of CCED use was associated with nonmedical use of prescription stimulants, with 22.2% of CCED consumers using prescription stimulants nonmedically. Miller44 found that CCED consumption was associated with nonmedical use of prescription drugs among White, but not Black undergraduates. In another study, Miller and Quigley48 also found that CCED consumption was associated with nonmedical prescription drug use even when controlling for other types of caffeine use. Trapp et al.47 reported that consuming CCEDs at least monthly was associated with using ecstasy and marijuana, as well as the number of illicit drugs used.
Several other risk behaviors have been linked to CCED consumption. Miller44 found that sexual risk-taking (e.g., unprotected intercourse, having intercourse under the influence of alcohol or other drugs), participating in extreme sports, seatbelt omission, and taking risks on a dare were more common among high-frequency (at least once a week) CCED consumers than low-frequency consumers. Another study of college students found that past-week consumption of CCEDs accounted for 29% and 21% of the variance in anxiety and sleep disturbances, respectively, when controlling for other types of caffeine use.51 A study of students at a predominantly minority university reported that CCED consumption was associated with drunk driving and riding in a car with an inebriated driver.52
One experimental study has been conducted on risk-taking behaviors related to CCED consumption.53 Participants attended four sessions. They were randomly assigned to consume one of four beverages at each session in a counterbalanced order: a CCED, alcohol, a CCED mixed with alcohol, or a placebo beverage. Doses of alcohol and caffeine were based on body weight. After consuming the beverages, participants completed the Balloon Analogue Risk Task, a laboratory measure of risk-taking. A small but significant increase in risk-taking was seen only among participants who had consumed the non-alcoholic CCED.
The only prospective study conducted to date on the relationship between CCED use and risk-taking behavior was guided by prior research suggesting that use of caffeine might exacerbate the underlying vulnerability to the use of other substances. Arria et al.49 examined the prospective relationship between CCED use during the second year of college and the risk for other forms of drug use during the subsequent year, after adjusting for prior use of each drug, demographic characteristics, and the use of other types of caffeine. The results showed that after adjustment for these variables, CCED users were more likely to initiate nonmedical use of prescription stimulants and analgesics and they increased the frequency with which they smoked tobacco. The adjusted odds ratio associated with CCED use for incident stimulant and analgesic use were 2.05 and 1.46, respectively.
The consumption of alcohol mixed with CCEDs has been linked to acute health risks and serious alcohol-related consequences.54–60 For further discussion of the consumption of alcohol mixed with CCEDs, see Marczinski et al. in this issue.
Among adolescents, Terry-McElrath et al.22 found that the consumption of CCEDs and energy shots is associated with past-month frequency of alcohol, cigarettes, marijuana, and amphetamine use among eighth, tenth, and twelfth graders, even after adjusting for demographic variables.
CONCLUSION AND KNOWLEDGE GAPS
Our analyses of MTF data show that almost one in three secondary school students in the US recently consumed a CCED. Data on CCED consumption from Canadian adolescents shows wide variation by province with estimates ranging from 57.2% to 64.6% on adolescents consuming CCEDs during the past year.61
The high prevalence of consumption of CCEDs observed in the current study underscores the need to demonstrate the safety of consuming these beverages, especially for individuals between the ages of 13 and 18. As mentioned earlier, the amount of caffeine per serving and the concentrations of caffeine among this beverage class varies widely.6,7 The acute and long term health consequences of such consumption are not known.
Research is needed to develop more comprehensive assessment methods for CCED and energy shot consumption. Despite the methodological strengths of the MTF survey, including its large sample size and its national representativeness, only a few questions were asked about CCEDs and energy shots. Because of this, the results cannot provide sufficient information about patterns of use, specific products consumed, contexts, or consequences. It would be useful to know the proportion of youth that have used various types of CCEDs in a defined time period, such as the past year or the past month, to more accurately estimate how much caffeine is being consumed by adolescents. Among users, assessments are needed that can reliably measure how much is consumed (e.g., typical, maximum, minimum) and how regularly consumption occurs. Given the concerns regarding ingesting high doses of caffeine on acute cardiovascular functioning, and during physical activity, future measures should attempt to characterize CCED use patterns (e.g., acute, chronic) and the contexts during which they are used (e.g., during exercise or sporting activities). CCED marketing messages often involve associations with physical activity and sporting events.18,62
Moreover, it is important to understand how these beverages are being incorporated into the usual dietary intake of adolescents. It is possible that they are replacing other beverages (e.g., water, soda, sports drinks) or alternatively, they might be consumed in addition to other types of beverages. Concerns have been raised about the dietary choices that adolescents and young adults make, including the types of nutritional supplements and beverages they consume.63,64 Recent data suggest that caffeine intake among children and adolescents in the US has remained steady during the last decade, but the proportion of caffeine intake that comes from energy drinks and coffee is increasing.65 The extent to which CCED consumption might be contributing to weight gain is not as well understood as for other sugar-sweetened beverages.66 Our data show that few youth report consuming energy shots only, but rather consume them in addition to larger-volume CCEDs. Although data from MTF does not differentiate between sugar-containing and sugar-free CCEDs, some CCEDs contain substantial amounts of sugar in addition to caffeine. It will be important for future research to understand the extent to which CCED consumption is a source of “empty calories” in the adolescent diet, and therefore could be a target for obesity prevention strategies. Malinauskas et al.5 reported that 74% of college students who consumed CCEDs drank sugar-containing versions, with females being over-represented among individuals who consumed sugar-free versions.
In contrast to the health concerns about cardiovascular effects of CCEDs that have been raised for several years, a newer concern relates to the possible effects of high levels of caffeine on the developing brain of adolescents.27,67,68 A limit of 2.5 milligrams per kilogram of caffeine per day has been suggested for children.67
Specific subgroups appear to be at increased risk for consuming excessive caffeine. Namely, eighth graders were both more likely to have consumed a CCED and to have consumed greater quantities of CCEDs and energy shots than their older counterparts. Similarly, Hispanic youth were more likely to consume CCEDs and energy shots than other racial/ethnic groups. No data are available to shed light on possible contributory factors underlying this observed subgroup variation. Adolescents begin to make more autonomous dietary choices during this time, and personal preference begins to play a larger role.24 Although parents’ influence on food choices decreases throughout this period, parental modeling still plays a role in determining adolescents’ food choices.24,69 For example, in one study of adolescent consumption of soft drinks, adolescents were approximately three times more likely to consume soft drinks regularly if they reported that their parents also consumed them regularly.69 Taste preference, peer habits, habit strength, and mass media have also been identified as important influences on adolescence food and beverage choices.69–72 While it is tempting to speculate that differences in family modeling of dietary practices or targeted marketing practices might underlie these differences, future research is needed to fully explain different patterns of consumption.
Little research has been conducted to understand CCED patterns among high-risk populations, such as young individuals with cardiovascular abnormalities. No data are available to evaluate the safety of consuming highly-caffeinated CCEDs concurrently or simultaneously with stimulant medications and/or illicit substances used by adolescents and young adults.
With respect to the association between CCED consumption and risk-taking behavior, the studies reviewed herein consistently demonstrate the existence of an association. However, more research is needed to clarify the nature of the observed relationship. For example, it is not entirely clear whether the association stems from a general increased propensity for risk-taking behavior among CCED users or whether CCEDs potentiate risk-taking among users. A few studies adjusted statistically for measures of general risk-taking propensity and still found strong associations between CCED use and alcohol-related problems.43,48 Further research is needed to understand the extent to which caffeine use during adolescence potentiates the reinforcing properties of other substances, especially because it is a period of rapid brain development.31,73 Additionally, more longitudinal research is needed to understand the temporal relationship between CCED use and risk-taking behaviors. The one prospective study conducted to date observed a relationship between CCEDs and the incident or “new” use of nonmedical prescription stimulants and analgesics, even after statistical adjustment for other indicators of risk-taking behavior.49
Given other research suggesting that adolescents are more likely to experience the rewarding properties of substances,74 it is important to understand if high levels of caffeine early in adolescence might be related to increased risk for use of other psychoactive substances later in life.36,37 It is clear that neurobiological changes during adolescence partially explain why adolescents are more likely than older individuals to engage in risk-taking behavior75–77 and perhaps less likely to fully recognize the consequences of such behavior. How caffeine and CCED use fit into the sequence of underage alcohol use and the use of other drugs among adolescents requires further inquiry.
It is possible that CCED consumption during the developmental periods of adolescence and young adulthood potentiates natural risk-taking behaviors of young people due to the stimulating pharmacological effects of caffeine. This possibility raises questions about the appropriateness of marketing and selling highly caffeinated CCEDs to adolescents because they might be especially susceptible to the potentiating effects of CCED use on risk-taking behavior. More research is warranted to fully understand the relationship between CCED use and risk-taking behavior, and how dose and pattern of caffeine consumption might mediate the relationship. Resolving these issues based on scientific evidence is needed to promote and protect adolescent health and safety.
Acknowledgments
Special thanks are given to Kaitlin Hippen, the interviewing team, and the participants.
FUNDING
The investigators acknowledge funding from the National Institute on Drug Abuse (R01DA014845, Dr. Arria, PI). The National Institute on Drug Abuse played no role in the study design, data collection and analysis, manuscript preparation and revision, or publication of this manuscript. Data collection for the Monitoring the Future survey was also funded by the National Institute on Drug Abuse (R01DA001411, Dr. Johnston, PI).
Footnotes
DECLARATION OF CONFLICT OF INTEREST
The authors have no relevant conflicts of interest to declare.
References
- 1.McCusker RR, Goldberger BA, Cone EJ. Caffeine content of energy drinks, carbonated sodas, and other beverages. J Anal Toxicol. 2006;30(2):112–114. doi: 10.1093/jat/30.2.112. [DOI] [PubMed] [Google Scholar]
- 2.Heckman MA, Sherry K, Gonzalez de Mejia E. Energy drinks: An assessment of their market size, consumer demographics, ingredient profile, functionality, and regulations in the United States. Compr Rev Food Sci Food Saf. 2010;9(3):303–317. doi: 10.1111/j.1541-4337.2010.00111.x. [DOI] [PubMed] [Google Scholar]
- 3.Clauson KA, Shields KM, McQueen CE, Persad N. Safety issues associated with commercially available energy drinks. J Am Pharm Assoc. 2008;48(3):e55–e63. doi: 10.1331/JAPhA.2008.07055. [DOI] [PubMed] [Google Scholar]
- 4.Smit HJ, Cotton JR, Hughes SC, Rogers PJ. Mood and cognitive performance effects of “energy” drink constituents: Caffeine, glucose and carbonation. Nutr Neurosci. 2004;7(3):127–139. doi: 10.1080/10284150400003041. [DOI] [PubMed] [Google Scholar]
- 5.Malinauskas BM, Aeby VG, Overton RF, Carpenter-Aeby T, Barber-Heidal K. A survey of energy drink consumption patterns among college students. Nutr J. 2007;6(1):35–41. doi: 10.1186/1475-2891-6-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks-A growing problem. Drug Alcohol Depend. 2009;99(1–3):1–10. doi: 10.1016/j.drugalcdep.2008.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wolk BJ, Ganetsky M, Babu KM. Toxicity of energy drinks. Curr Opin Pediatr. 2012;24(2):243–251. doi: 10.1097/MOP.0b013e3283506827. [DOI] [PubMed] [Google Scholar]
- 8.U.S. Code of Federal Regulations, nr 21CFR-182.1180, 21(2012).
- 9.Packaged Facts. Energy drinks and shots: US market trends. Rockville, MD: 2013. [Google Scholar]
- 10.Drug Abuse Warning Network. Update on emergency department visits involving energy drinks: A continuing public health concern. Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality; 2013. [PubMed] [Google Scholar]
- 11.Center for Food Safety and Applied Nutrition. Voluntary reports on Red Bull energy drink. Washington, DC: Food and Drug Administration; 2012. [Google Scholar]
- 12.Center for Food Safety and Applied Nutrition. Voluntary and mandatory reports on 5-Hour Energy, Monster Energy, and Rockstar energy drink. Washington, DC: Food and Drug Administration; 2012. [Google Scholar]
- 13.Higgins JP, Babu KM. Caffeine reduces myocardial blood flow during exercise. Am J Med. 2013;126(8):730.e1–730.e8. doi: 10.1016/j.amjmed.2012.12.023. [DOI] [PubMed] [Google Scholar]
- 14.Savoca MR, MacKey L, Evans CD, Wilson M, Ludwig DA, Harshfield GA. Association of ambulatory blood pressure and dietary caffeine in adolescents. Am J Hypertens. 2005;18(1):116–120. doi: 10.1016/j.amjhyper.2004.08.011. [DOI] [PubMed] [Google Scholar]
- 15.Temple JL, Dewey AM, Briatico LN. Effects of acute caffeine administration on adolescents. Exp Clin Psychopharmacol. 2010;18(6):510–520. doi: 10.1037/a0021651. [DOI] [PubMed] [Google Scholar]
- 16.Temple JL, Ziegler AM. Gender differences in subjective and physiological responses to caffeine and the role of steroid hormones. J Caffeine Res. 2011;1(1):41–48. doi: 10.1089/jcr.2011.0005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Committee on Nutrition and the Council on Sports Medicine and Fitness. Sports drinks and energy drinks for children and adolescents: Are they appropriate? Pediatrics. 2011;127(6):1182–1189. doi: 10.1542/peds.2011-0965. [DOI] [PubMed] [Google Scholar]
- 18.American Medical Association House of Delegates. Banning marketing and sale of high-energy/stimulant drinks to children/adolescents under the age of 18 (Resolution: 409 (A-13)) 2013. [Google Scholar]
- 19.Centers for Disease Control and Prevention. [Accessed September 10, 2013];2010 NHIS Questionnaire: Sample adult, diet and nutrition. 2011 Question ID: NAC.045_001.000. Available at: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Survey_Questionnaires/NHIS/2010/English/qcancer.pdf.
- 20.Centers for Disease Control and Prevention. [Accessed September 10, 2013];National Health and Nutrition Examination Survey: Dietary interview component. 2009 http://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/dietaryrecall_f.pdf.
- 21.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future: National survey results on drug use, 1975–2012: Volume I: Secondary school students. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2013. [Google Scholar]
- 22.Terry-McElrath YM, O’Malley PM, Johnston LD. Energy drinks, soft drinks, and substance use among United States secondary school students. J Addict Med. 2014;8(1):6–13. doi: 10.1097/01.ADM.0000435322.07020.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wahl R. Nutrition in the adolescent. Pediatr Ann. 1999;28(2):107–111. doi: 10.3928/0090-4481-19990201-07. [DOI] [PubMed] [Google Scholar]
- 24.World Health Organization. Nutrition in adolescence: Issues and challenges for the health sector. World Health Organization; 2005. [Google Scholar]
- 25.Orbeta RL, Overpeck MD, Ramcharran D, Kogan MD, Ledsky R. High caffeine intake in adolescents: Associations with difficulty sleeping and feeling tired in the morning. J Adolesc Health. 2006;38(4):451–453. doi: 10.1016/j.jadohealth.2005.05.014. [DOI] [PubMed] [Google Scholar]
- 26.James JE, Kristjansson AL, Sigfusdottir ID. Adolescent substance use, sleep, and academic achievement: Evidence of harm due to caffeine. J Adolesc. 2011;34(4):665–673. doi: 10.1016/j.adolescence.2010.09.006. [DOI] [PubMed] [Google Scholar]
- 27.Olini N, Kurth S, Huber R. The effects of caffeine on sleep and maturational markers in the rat. PLoS One. 2013;8(9):1–8. doi: 10.1371/journal.pone.0072539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Steinberg L. Risk taking in adolescence: What changes, and why? Ann N Y Acad Sci. 2004;1021:51–58. doi: 10.1196/annals.1308.005. [DOI] [PubMed] [Google Scholar]
- 29.White AM. Understanding adolescent brain development and its implications for the clinician. Adolesc Med. 2009;20(1):73–90. [PubMed] [Google Scholar]
- 30.Casey BJ, Getz S, Galvan A. The adolescent brain. Dev Rev. 2008;28(1):62–77. doi: 10.1016/j.dr.2007.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Giedd JN. Structural magnetic resonance imaging of the adolescent brain. Ann N Y Acad Sci. 2004;1021:77–85. doi: 10.1196/annals.1308.009. [DOI] [PubMed] [Google Scholar]
- 32.Rubia K, Overmeyer S, Taylor E, et al. Functional frontalisation with age: Mapping neurodevelopmental trajectories with fMRI. Neurosci Biobehav Rev. 2000;24(1):13–19. doi: 10.1016/s0149-7634(99)00055-x. [DOI] [PubMed] [Google Scholar]
- 33.Blakemore SJ, Robbins TW. Decision-making in the adolescent brain. Nat Neurosci. 2012;15(9):1184–1191. doi: 10.1038/nn.3177. [DOI] [PubMed] [Google Scholar]
- 34.Monk CS, McClure EB, Nelson EE, et al. Adolescent immaturity in attention-related brain engagement to emotional facial expressions. NeuroImage. 2003;20(1):420–428. doi: 10.1016/s1053-8119(03)00355-0. [DOI] [PubMed] [Google Scholar]
- 35.Somerville LH, Jones RM, Casey BJ. A time of change: Behavioral and neural correlates of adolescent sensitivity to appetitive and aversive environmental cues. Brain Cogn. 2010;72(1):124–133. doi: 10.1016/j.bandc.2009.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Temple JL. Caffeine use in children: What we know, what we have left to learn, and why we should worry. Neurosci Biobehav Rev. 2009;33(6):793–806. doi: 10.1016/j.neubiorev.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cauli O, Morelli M. Caffeine and the dopaminergic system. Behav Pharmacol. 2005;16(2):63–77. doi: 10.1097/00008877-200503000-00001. [DOI] [PubMed] [Google Scholar]
- 38.Swanson JA, Lee JW, Hopp JW. Caffeine and nicotine: A review of their joint use and possible interactive effects in tobacco withdrawal. Addict Behav. 1994;19(3):229–256. doi: 10.1016/0306-4603(94)90027-2. [DOI] [PubMed] [Google Scholar]
- 39.Inter-university Consortium for Political and Social Research. [Accessed September 10, 2013];National Addiction and HIV Data Archive Program. 2012 http://www.icpsr.umich.edu/icpsrweb/NAHDAP/
- 40.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future: National survey results on drug use, 1975–2011: Volume I: Secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan; 2012. [Google Scholar]
- 41.IBM Corporation. IBM SPSS Statistics. Armonk, NY: IBM Corporation; 2011. [computer program]. Version 20. [Google Scholar]
- 42.Johnston LD, Bachman JG, O’Malley PM, Schulenberg JE. [Accessed August 1, 2013];Monitoring the Future: A continuing study of American youth (8th- and 10th-Grade Surveys), 2011: Data codebook. 2012 http://doi.org/10.3886/ICPSR33902.v1.
- 43.Arria AM, Caldeira KM, Kasperski SJ, Vincent KB, Griffiths RR, O’Grady KE. Energy drink consumption and increased risk for alcohol dependence. Alcohol Clin Exp Res. 2011;35(2):365–375. doi: 10.1111/j.1530-0277.2010.01352.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Miller KE. Energy drinks, race, and problem behaviors among college students. J Adolesc Health. 2008;43(5):490–497. doi: 10.1016/j.jadohealth.2008.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Skewes MC, Decou CR, Gonzalez VM. Energy drink use, problem drinking and drinking motives in a diverse sample of Alaskan college students. Int J Circumpolar Health. 2013:72. doi: 10.3402/ijch.v72i0.21204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Velazquez CE, Poulos NS, Latimer LA, Pasch KE. Associations between energy drink consumption and alcohol use behaviors among college students. Drug Alcohol Depend. 2012;123(1–3):167–172. doi: 10.1016/j.drugalcdep.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 47.Trapp GSA, Allen KL, O’Sullivan T, Robinson M, Jacoby P, Oddy WH. Energy drink consumption among young Australian adults: Associations with alcohol and illicit drug use. Drug Alcohol Depend. 2014;134(1):30–37. doi: 10.1016/j.drugalcdep.2013.09.006. [DOI] [PubMed] [Google Scholar]
- 48.Miller KE, Quigley BM. Energy drink use and substance use among musicians. J Caffeine Res. 2011;1(1):67–73. [Google Scholar]
- 49.Arria AM, Caldeira KM, Kasperski SJ, et al. Increased alcohol consumption, nonmedical prescription drug use, and illicit drug use are associated with energy drink consumption among college students. J Addict Med. 2010;4(2):74–80. doi: 10.1097/ADM.0b013e3181aa8dd4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Woolsey CL, Barnes LB, Jacobson BH, et al. Frequency of energy drink use predicts illicit prescription stimulant use. Subst Abus. 2013;10(8):784–791. doi: 10.1080/08897077.2013.810561. [DOI] [PubMed] [Google Scholar]
- 51.Stasio MJ, Curry KIM, Wagener AL, Glassman DM. Revving up and staying up: Energy drink use associated with anxiety and sleep quality in a college sample. Coll Stud J. 2011;45(4):738–748. [Google Scholar]
- 52.Spierer DK, Blanding N, Santella A. Energy drink consumption and associated health behaviors among university students in an urban setting. J Community Health. 2014;39(1):132–138. doi: 10.1007/s10900-013-9749-y. [DOI] [PubMed] [Google Scholar]
- 53.Peacock A, Bruno R, Martin FH, Carr A. The impact of alcohol and energy drink consumption on intoxication and risk-taking behavior. Alcohol Clin Exp Res. 2013;37(7):1234–1242. doi: 10.1111/acer.12086. [DOI] [PubMed] [Google Scholar]
- 54.O’Brien MC, McCoy TP, Rhodes SD, Wagoner A, Wolfson M. Caffeinated cocktails: Energy drink consumption, high-risk drinking, and alcohol-related consequences among college students. Acad Emerg Med. 2008;15(5):453–460. doi: 10.1111/j.1553-2712.2008.00085.x. [DOI] [PubMed] [Google Scholar]
- 55.O’Brien MC, McCoy TP, Egan KL, Goldin S, Rhodes SD, Wolfson M. Caffeinated alcohol, sensation seeking, and injury risk. J Caffeine Res. 2013;3(2):59–66. doi: 10.1089/jcr.2013.0004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Miller KE. Alcohol mixed with energy drink use and sexual risk-taking: Casual, intoxicated, and unprotected sex. J Caffeine Res. 2012;2(2):62–69. doi: 10.1089/jcr.2012.0015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Howland J, Rohsenow DJ. Risks of energy drinks mixed with alcohol. JAMA. 2013;309(3):245–246. doi: 10.1001/jama.2012.187978. [DOI] [PubMed] [Google Scholar]
- 58.Marczinski CA, Fillmore MT, Henges AL, Ramsey MA, Young CR. Mixing an energy drink with an alcoholic beverage increases motivation for more alcohol in college students. Alcohol Clin Exp Res. 2013;37(2):276–283. doi: 10.1111/j.1530-0277.2012.01868.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Marczinski CA, Fillmore MT, Henges AL, Ramsey MA, Young CR. Effects of energy drinks mixed with alcohol on information processing, motor coordination and subjective reports of intoxication. Exp Clin Psychopharmacol. 2012;20(2):129–138. doi: 10.1037/a0026136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Marczinski CA, Fillmore MT, Bardgett ME, Howard MA. Effects of energy drinks mixed with alcohol on behavioral control: risks for college students consuming trendy cocktails. Alcohol Clin Exp Res. 2011;35(7):1282–1292. doi: 10.1111/j.1530-0277.2011.01464.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Gupta N, Wang H, Collette M, Pilgrim W. New Brunswick Study Drug Use Survey report 2012. New Brunswick: New Brunswick Department of Health; 2013. [Google Scholar]
- 62.Blankson KL, Thompson AM, Ahrendt DM, Vijayalakshmy P. Energy drinks: What teenagers (and their doctors) should know. Pediatr Rev. 2013;34(2):55–62. doi: 10.1542/pir.34-2-55. [DOI] [PubMed] [Google Scholar]
- 63.Popkin BM, Armstrong LE, Bray GM, Caballero B, Frei B, Willett WC. A new proposed guidance system for beverage consumption in the United States. Am J Clin Nutr. 2006;83(3):529–542. doi: 10.1093/ajcn.83.3.529. [DOI] [PubMed] [Google Scholar]
- 64.O’Dea JA. Consumption of nutritional supplements among adolescents: Usage and perceived benefits. Health Educ Res. 2003;18(1):98–107. doi: 10.1093/her/18.1.98. [DOI] [PubMed] [Google Scholar]
- 65.Branum AM, Rossen LM, Schoendorf KC. Trends in caffeine intake among US children and adolescents. Pediatrics. doi: 10.1542/peds.2013-2877. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am J Clin Nutr. 2006;84(2):274–288. doi: 10.1093/ajcn/84.1.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam. 2003;20(1):1–30. doi: 10.1080/0265203021000007840. [DOI] [PubMed] [Google Scholar]
- 68.Hughes RN. Neurobiological consequences of exposure to caffeine during development: Important issues and areas of concern. J Caffeine Res. 2011;1(2):97–99. [Google Scholar]
- 69.Grimm GC, Harnack L, Story M. Factors associated with soft drink consumption in school-aged children. J Am Diet Assoc. 2004;104(8):1244–1249. doi: 10.1016/j.jada.2004.05.206. [DOI] [PubMed] [Google Scholar]
- 70.Freisling H, Elmadfa I, Haas K. Mass media nutrition information sources and associations with fruit and vegetable consumption among adolescents. Public Health Nutr. 2010;13(2):269–275. doi: 10.1017/S1368980009991297. [DOI] [PubMed] [Google Scholar]
- 71.Utter J, Scragg R, Schaaf D. Associations between television viewing and consumption of commonly advertised foods among New Zealand children and young adolescents. Public Health Nutr. 2006;9(5):606–612. doi: 10.1079/phn2005899. [DOI] [PubMed] [Google Scholar]
- 72.van der Horst K, Kremers S, Ferreira I, Singh A, Oenema A, Brug J. Perceived parenting style and practices and the consumption of sugar-sweetened beverages by adolescents. Health Educ Res. 2007;22(2):295–304. doi: 10.1093/her/cyl080. [DOI] [PubMed] [Google Scholar]
- 73.Giedd JN, Blumenthal J, Jeffries NO, et al. Brain development during childhood and adolescence: A longitudinal MRI study. Nat Neurosci. 1999;2(10):861–863. doi: 10.1038/13158. [DOI] [PubMed] [Google Scholar]
- 74.Sturman DA, Moghaddam B. The neurobiology of adolescence: changes in brain architecture, functional dynamics, and behavioral tendencies. Neurosci Biobehav Rev. 2011;35(8):1704–1712. doi: 10.1016/j.neubiorev.2011.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Romer D, Hennessy M. A biosocial-affect model of adolescent sensation seeking: The role of affect evaluation and peer-group influence in adolescent drug use. Prev Sci. 2007;8(2):89–101. doi: 10.1007/s11121-007-0064-7. [DOI] [PubMed] [Google Scholar]
- 76.Pharo H, Sim C, Graham M, Gross J, Hayne H. Risky business: Executive function, personality, and reckless behavior during adolescence and emerging adulthood. Behav Neurosci. 2011;125(6):970–978. doi: 10.1037/a0025768. [DOI] [PubMed] [Google Scholar]
- 77.Spear LP. Adolescent neurodevelopment. J Adolesc Health. 2013;52(Suppl 2):s7–s13. doi: 10.1016/j.jadohealth.2012.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]