

Abstract
Background
Pigmented purpuric dermatoses (PPD) are chronic, recurrent group of disorders characterized by petechial and pigmentary macules usually localized on the lower limbs. Its etiopathogenesis is unknown. There are very few clinical and etiological studies on PPD in the literature.
Objective
We aim to examine the etiopathogenetic factors of PPD retrospectively.
Methods
Demographic characteristics, history of co-morbid disorders and drug usage, hepatitis markers, levels of serum lipids, findings of Doppler ultrasonography in lower extremities, and patch test results of the 24 patients of PPD were examined retrospectively. The patch test results, history of drug use, and co-morbid disorders of the patients were compared with those of the control groups.
Results
The male-to-female ratio was 1 : 2, and 83.3% of the patients had Schamberg disease. Seventeen patients had co-morbid disorders and 16 used various drugs, but there was no statistically significant difference between the controls and patients. One patient was positive for hepatitis B surface antigen and 1, for anti-hepatitis C virus antibody. Nine had elevated total cholesterol levels, and 5 had elevated triglyceride levels. Further, 30% of them were positive for at least 1 allergen, while 16% of the control subjects were positive for at least 1 allergen, but statistically significant difference was not found between the 2 groups. Variable degrees of venous insufficiency were detected in 75% of the patients on Doppler ultrasonography of the lower extremities.
Conclusion
Venous insufficiency and hypercholesterolemia might be the basic predisposing factors for PPD. Further studies are needed to show if diabetes mellitus and hypertension may cause perivascular inflammation in PPD.
Keywords: Patch tests, Pigmentation disorders, Vascular diseases
INTRODUCTION
Pigmented purpuric dermatosis (PPD) includes a spectrum of vascular disorders characterized by petechiae and bronze discoloration of the skin. The primary areas of localization of the lesions are the lower limbs. The etiology of PPD, however, remains obscure1,2,3. There are very few clinical and etiological studies on PPD in the literature, as the disorder is rather uncommon2,3. A few case series on the relation between PPD and hepatitis B or C virus and hyperlipidemia have been reported4,5. PPD patients underwent patch testing only in 1 study, and this study did not have a control group6. In the present study, the demographic characteristics, history of co-morbid disorders and drug usage, hepatitis markers, levels of serum lipids, findings of Doppler ultrasonography in the lower extremities, and patch test results of the PPD patients were examined retrospectively. To the best of our knowledge, this study is the first to compare the patch test results of the PPD patient group with those of the control group.
MATERIALS AND METHODS
In all, 24 patients diagnosed with PPD on the basis of clinical and histopathological findings in the last 2 years were enrolled in the study. As this study was a retrospective study, the age; sex; duration of the disorder and clinical type of PPD; co-morbid disorders; systemic drugs taken by the patients; levels of total cholesterol, cholesterol subtypes, and triglycerides; positivity for hepatitis B surface antigen (HBsAg), anti-hepatitis B surface antigen (anti-HBs), and anti-hepatitis C virus (anti-HCV) antibodies; and outcomes of patch testing with European Standard Series (ALSER, 27 allergen) were obtained from the patients' records. The patch tests were evaluated after 48, 72, and 96 hours. The results of the patch test, drug use, and co-morbid disorders of the patients were statistically compared with those of the control group using the chisquare test (25 age- and sex-matched subjects with tinea pedis and onychomycosis were chosen from the control group of another study, which has not been published yet, as the control group in this study). This study was approved by local ethical commity of Ankara Numune Education and Research Hospital. The statistical evaluation is made with SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 24 patients with PPD (13 men [54.2%] and 11 women [45.8%]) were enrolled in the study. The male-to-female ratio was 1 : 2. The patients' age ranged from 19 to 82 years (mean, 48.96±16.80 years). The duration of PPD varied between 15 days and 72 months (mean, 12.15±18.40 months); 20 patients (83.3%) had Schamberg disease (SD) (Fig. 1), 3 (12.5%) had lichen aureus (Fig. 2), and 1 (4.2%) had eczematid-like purpura of Doucas and Kapetanakis. In all patients, the lower extremities were the main affected sites.
Fig. 1.

Schamberg disease.
Fig. 2.

Lichen aureus.
Furthermore, 17 patients had disorders other than PPD, 4 patients had diabetes mellitus (DM), 3 had hypertension (HT), and 2 had both DM and HT (Table 1). Sixteen patients were receiving therapy with various medications for diseases other than PPD (Table 1). When the patient group was compared with the control group with regard to co-morbid diseases (total, p=0.10; DM, p=0.28; and HT, p=0.72) and drug use (p=0.11), no statistically significant difference was found, although in the patient group, the frequencies of co-morbid diseases and drug use were higher in the patient group than in the control group.
Table 1.
The co-morbid diseases and drugs used by the patients and control subjects
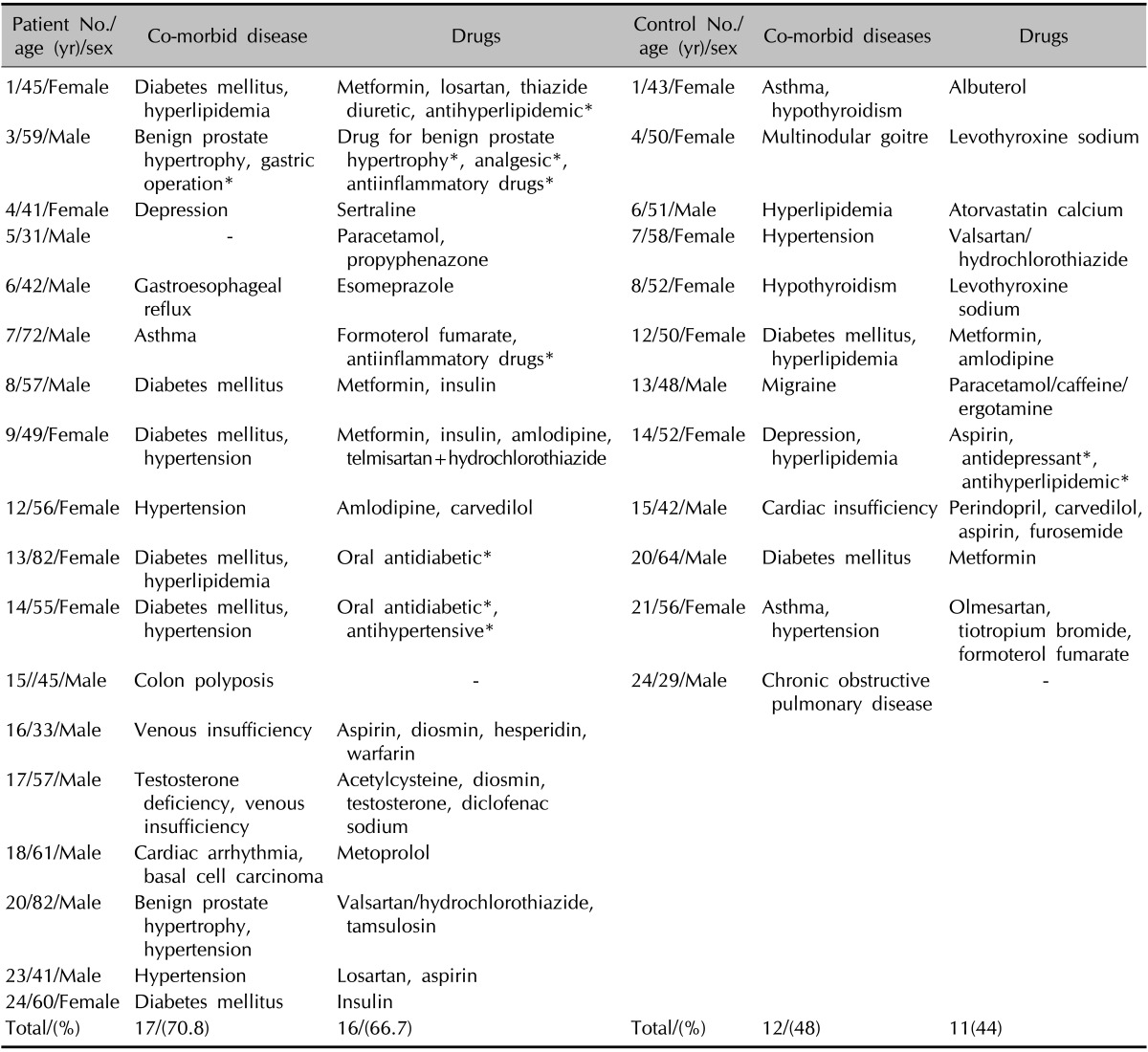
*The unknown name of drugs' of the patients.
Six of 23 patients were positive for anti-HBs antibody; 1 of 23 patients, for HBsAg (data regarding 23 patients were available); and 1, for HCV antibody (data regarding 22 patients were available). The serum lipid levels were measured in 21 patients-9 of them had high levels of total cholesterol, and 5 had high levels of triglyceride. The detailed results of serum lipid tests are presented in Table 2. While varicose dilatation was detected in 5 patients clinically, variable degrees of venous insufficiency were detected in 15 of 20 patients whose lower extremities were examined by Doppler ultrasonography (Table 2).
Table 2.
The laboratory results of the patients with pigmented purpuric dermatoses
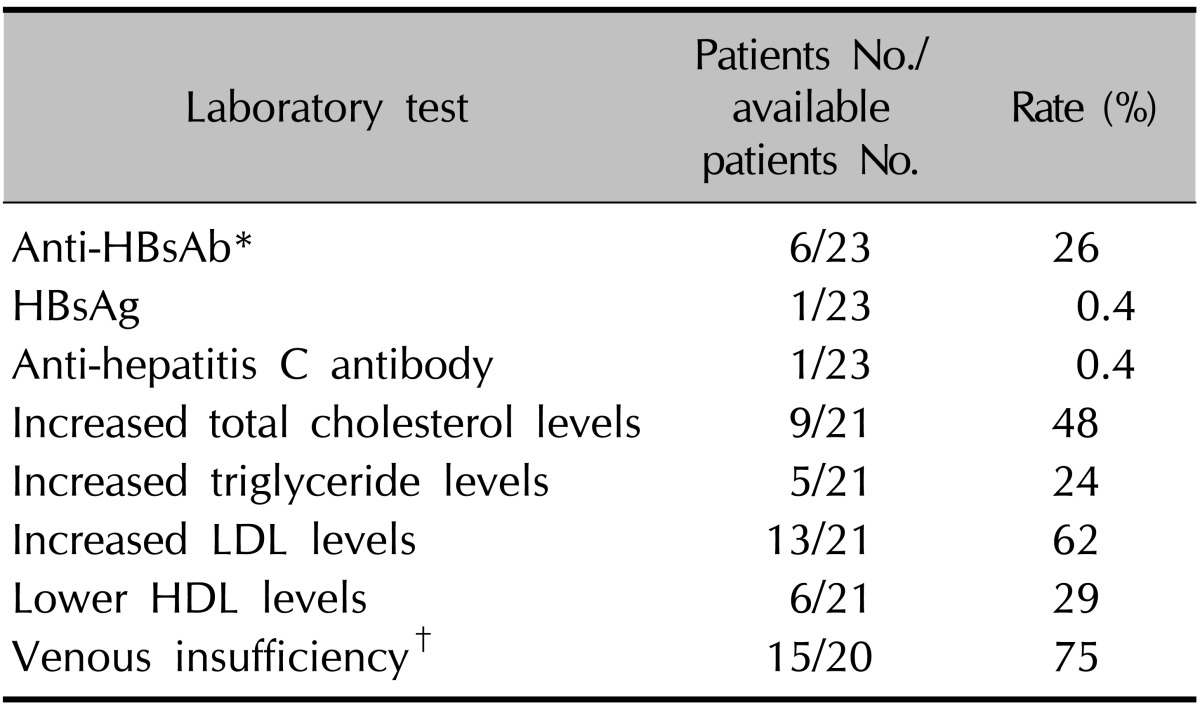
LDL: low density lipoprotein, HDL: high density lipoprotein, HBsAg: hepatitis B surface antigen. *None of the patients that have positive anti-hepatitis B antibodies had vaccination for hepatitis B virus. †The patients with venous insufficiency that was detected by Doppler ultrasonography of lower extremities. Normal limits for total cholesterol, triglyceride, LDL and HDL are <200 mg/dl, <200 mg/dl, <100 mg/dl and 35~55 mg/dl, respectively.
The patch test results were available for 23 patients: 7 (30%) of them were positive for at least 1 allergen while 4 (16%) control subjects were positive for at least 1 allergen. In the patient group, 4 patients tested positive for only 1 allergen and 3, for more than 1 allergen; in the control group, all patients tested positive for only 1 allergen.
Positive patch test results are presented in Table 3. None of the patients had a purpuric response to the patch test.
Table 3.
The results of patch test of the patients and control subjects

*Three patients had positivity to more than one allergen.
Positive patch test results showing positivity to at least 1 allergen (p=0.23), to more than 1 allergen (p=0.10), and to each allergen were compared in both groups by using the chi-square test. There was no statistically significant difference in any of these parameters between the groups.
DISCUSSION
PPD consists of a group of chronic and recurrent diseases that are morphologically different but pathologically indistinguishable and have been traditionally divided into 5 clinical entities; however, this division does not influence the management or prognosis.
SD accounts for half of all PPD cases. Eczematid-like purpura of Doucas and Kapetanakis, lichen aureus, Majocchi disease (MD), and pigmented purpuric lichenoid dermatosis account for, respectively, 10%, 10%, 5%, and 5% of all PPD cases7. In the present study, SD was the most common type of PPD, accounting for 83.3% of all PPD cases. The reasons for the high incidence rate in our study as compared to that in the literature may be the genetic and geographic differences.
PPD appears more frequently in males, except for MD. The male-to-female ratio was variable in different studies (range, 1.4~3.8)1,2,3,6. PPD may occur at any age, but it is most commonly seen in the fourth and fifth decades of life2,3,6. In the present study, age and male : female ratio of the patients were similar to those reported in the literature. The etiology of PPD is unknown. It has been reported that venous HT, exercise, gravitational dependency, capillary fragility, focal infections, and alcohol ingestion are important provocative factors for the occurrence of PPD1,2,5.
Drugs have been reported as triggering factors in PPD, especially SD. The most common medications implicated in PPD are acetaminophen, aspirin, adalin, glipizide, glybuzole, hydralazine, and reserpine1. Sixteen patients were using various drugs for diseases other than PPD in this study. When the patient group was compared with the control group according to drug use, a statistically significant difference was not detected. Both groups might have had similar incidence of drug use, mostly multiple drugs, because of the advanced age of the patients and controls. Since this study was a retrospective study, the causative drugs could not be detected.
A number of disorders have been found to be associated with PPD, such as DM, rheumatoid arthritis, lupus erythematous, thyroid dysfunction, hereditary spherocytosis, hematological disorders, hepatic disease, porphyria, and other malignancies1,3,5,8. In our study, 4 patients had DM, 3 patients, HT, and 2 patients, both DM and HT. However, statistical significance could not be detected between PPD patients and control subjects according to associated diseases. We think that diseases such as DM and HT do not play a primary role, but if microvascular damage develops because of these disorders, it may contribute to the occurrence of PPD.
Some reports have suggested an association between PPD and hepatitis B or C infection4. While 5 patients were positive for HCV and 2 for HBsAg in a study involving 10 patients, in a case-control study, no statistically significant difference was observed in the prevalence of positive hepatitis B or C serological findings between the patients and controls2,4. In the present study, only 1 patient was positive for HBsAg and 1, for HCV. In Turkey, anti-HCV seroprevalence was found to be 1% in the TURKHEP study that was conducted in the whole country9. In an epidemiologic study published in 2012, HBsAg positivity was found to be 5.96% in Turkey10. When the results of the present study were compared to prevalence of hepatitis B or C in Turkey, it was found that these viruses did not play a role in the etiopathogenesis of PPD.
There are very few case series on the granulomatous variant of PPD associated with hyperlipidemia5,11. The levels of serum lipids in the PPD patients were evaluated in the present study, although none of our patients had the granulomatous variant; hyperlipidemia may have been responsible for the microvascular inflammatory reaction.
Further, 42.9% of the patients had hypercholesterolemia, 23.8%, hypertriglyceridemia, 62%, increased low density lipoprotein (LDL) level, and 29%, decreased high density lipoprotein (HDL). The rates of hypercholesterolemia and increased levels of LDL in our study were higher than those in Turkish adults. The prevalence of hypercholesterolemia, hypertriglyceridemia, increased LDL levels, and decreased HDL levels were 38.6%, 51.3%, 30.9%, and 33.7%, respectively, in Turkish adults12,13. We think hypercholesterolemia plays a role in the etiopathogenesis of not only the granulomatous variant but also other forms of PPD.
To the best of our knowledge, this is the first study examining venous insufficiency with Doppler ultrasonography findings in PPD patients. The present study showed varicose dilatation in 20% of the patients clinically and variable degrees of venous insufficiencies in 75% of the patients. This rate is rather high and the main predisposing factor of PPD may be venous insufficiency.
Another factor that might be responsible in the etiopathogenesis of PPD is contact allergy. The patch test results were found to be relevant in some case reports on PPD14.
In one study that evaluated the patch test results in patients with PPD, the positive results could not be compared with those of the control group. Engin et al.6 found positive patch test results for 54% of the patients, and nickel sulfate was the most common allergen detected. The other allergens were fragrance mix, disperse blue 106, formaldehyde resin, cobalt chloride, and epoxy resin. In the present study, positive patch tests were obtained in 30% of the patients and the most common allergens were nickel sulfate and fragrance mix, similar to the study of Engin et al.6. The positivity rate was not statistically different between the patients and control subjects. We think that contact allergy is not the primary etiologic factor responsible for PPD.
Although a retrospective study, this study examined multiple parameters. Moreover, it highlighted the importance of comparing some parameters such as co-morbid diseases, drug use, and patch test results between patients and controls. We think that venous insufficiency and hyperlipidemia are the basic predisposing factors in PPD.
Future case-control studies are needed to show whether DM and HT contribute to the pathogenesis through microvascular damage.
References
- 1.Sardana K, Sarkar R, Sehgal VN. Pigmented purpuric dermatoses: an overview. Int J Dermatol. 2004;43:482–488. doi: 10.1111/j.1365-4632.2004.02213.x. [DOI] [PubMed] [Google Scholar]
- 2.Ehsani AH, Ghodsi SZ, Nourmohammad-Pour P, Aghazadeh N, Damavandi MR. Pigmented purpura dermatosis and viral hepatitis: a case-control study. Australas J Dermatol. 2013;54:225–227. doi: 10.1111/ajd.12003. [DOI] [PubMed] [Google Scholar]
- 3.Sharma L, Gupta S. Clinicoepidemiological study of pigmented purpuric dermatoses. Indian Dermatol Online J. 2012;3:17–20. doi: 10.4103/2229-5178.93486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dessoukey MW, Abdel-Dayem H, Omar MF, Al-Suweidi NE. Pigmented purpuric dermatosis and hepatitis profile: a report on 10 patients. Int J Dermatol. 2005;44:486–488. doi: 10.1111/j.1365-4632.2005.02045.x. [DOI] [PubMed] [Google Scholar]
- 5.Lin WL, Kuo TT, Shih PY, Lin WC, Wong WR, Hong HS. Granulomatous variant of chronic pigmented purpuric dermatoses: report of four new cases and an association with hyperlipidaemia. Clin Exp Dermatol. 2007;32:513–515. doi: 10.1111/j.1365-2230.2007.02462.x. [DOI] [PubMed] [Google Scholar]
- 6.Engin B, Ozdemir M, Kaplan M, Mevlitoğlu I. Patch test results in patients with progressive pigmented purpuric dermatosis. J Eur Acad Dermatol Venereol. 2009;23:209. doi: 10.1111/j.1468-3083.2008.02789.x. [DOI] [PubMed] [Google Scholar]
- 7.Cox NH, Piette WW. Purpura and microvascular occlusion. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's textbook of dermatology. 8th ed. Vol. 3. Chichester, West Sussex, UK: Wiley-Blackwell Publishing; 2010. Chapter 49.22. [Google Scholar]
- 8.Magro CM, Schaefer JT, Crowson AN, Li J, Morrison C. Pigmented purpuric dermatosis: classification by phenotypic and molecular profiles. Am J Clin Pathol. 2007;128:218–229. doi: 10.1309/AQMU3JFE2A66LC7E. [DOI] [PubMed] [Google Scholar]
- 9.Tozun N, Ozdogan OC, Cakaloglu Y, İdilman R, Karasu Z, Akarca US, et al. Nationwide prevalence study and risk factors for hepatitis A, B, C and D infections in Turkey. Hepatology. 2010;23:393–395. [Google Scholar]
- 10.Ergunay K, Balaban Y, Cosgun E, Alp A, Simsek H, Sener B, et al. Epidemiologic trends in HBV infections at a reference centre in Turkey: an 11-year retrospective analysis. Ann Hepatol. 2012;11:672–678. [PubMed] [Google Scholar]
- 11.Wong WR, Kuo TT, Chen MJ, Chan HL. Granulomatous variant of chronic pigmented purpuric dermatosis: report of two cases. Br J Dermatol. 2001;145:162–164. doi: 10.1046/j.1365-2133.2001.04304.x. [DOI] [PubMed] [Google Scholar]
- 12.Onat A, Türkmen S, Karabulut A, Yazıcı M, Can G, Sansoy V. Combined hypercholesterolemia and hypertension among turkish adults: prevalence and prediction of cardiovascular disease risk. Türk Kardiyol Dern Arş. 2004;32:533–541. [Google Scholar]
- 13.Onat A, Sansoy V, Uyarel H, Keleş İ, Hergenç G. Türklerde HDL-kolesterol düzeyleri, çevresel etkenler ve metabolik sendrom kriterleri. Türk Kardiyol Dern Arş. 2004;32:273–278. [Google Scholar]
- 14.Lazarov A, Cordoba M. The purpuric patch test in patients with allergic contact dermatitis from azo dyes. Contact Dermatitis. 2000;42:23–26. doi: 10.1034/j.1600-0536.2000.042001023.x. [DOI] [PubMed] [Google Scholar]