

Abstract
Background:
Increasing population, fast paced industrialization, increased, competitiveness, unanticipated problems in the work place have increased the stress among the females working in health care in recent times.
Aim:
The aim of the following study is to detect the stress levels among female health care professionals in the age group of 25-35 years and its impact on health.
Subjects and Methods:
A prospective cross-sectional pilot project was conducted in a tertiary care hospital in Eastern part of India, after receiving approval from the Institutional Ethics Committee and informed consent form was taken from the subjects. Stress level in the subjects was assessed according to the presumptive life event stress scale. Females with scores above 200 were selected. For these, initial assessment of anthropometric measurement, electrocardiogram and lipid profile analysis, resting pulse rate, blood pressure, physical fitness index (PFI), breath holding time (BHT), isometric hand grip (IHG) test results were evaluated and recorded. All subjects were given training of progressive muscle relaxation (PMR) for 3 months. After 3 months, the lipid profile and vital parameters, Perceived Stress Scale values were re-evaluated and subjects were asked to repeat the same exercises and data thus recorded were analyzed using Statistical Package for the Social Sciences (SPSS) version 16 (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, SPSS Inc.).
Results:
Significant decrease in resting heart rate, blood pressure and Perceived Stress Scale levels was seen after PMR training in the subjects. Results of BHT, IHG tests and PFI were significantly increased after PMR training. There was a significant decrease in total cholesterol, triglyceride and low-density lipoprotein cholesterol in subjects after practicing PMR for 3 months.
Conclusions:
Increasing stress among female health care professionals is a cause for concern and there is a need to adopt early life-style modification by practicing relaxation exercises to ameliorate stress and to improve not only their quality-of-life in general, but patient care in particular.
Keywords: Female stress, relaxation techniques, health care professionals
Introduction
Stress in recent times has increased manifold with rapid industrialization. Women who are engaged in providing health care are subjected to more stress in developing countries than those in developed countries. Stress experiences often lead to various chronic health conditions such as hypertension, coronary heart disease (CAD).[1,2,3,4] The women's ischemic syndrome evaluation study is changing the concept that women suffer less from heart diseases.[1,2,3,4] The cardiovascular death rate is seen to be declining steadily in men. Women who have angioplasties and bypasses do not do as well as their male counterparts. Most of them suffer from heart attacks or congestive heart failure after treatment. The discovery of widespread micro vessel disease helps to explain why so many women with ischemic heart disease are misdiagnosed and undertreated.[1,2,3,4]
Stress at work is an important risk factor for the emergence of metabolic syndrome. Plausible pathophysiology involves direct neuroendocrine effects and autonomic imbalance.[5,6,7,8] Perceived stress has been reported higher in health care professionals. A national survey of physicians in Canada showed that both male and female doctors experienced high levels of occupational stress.[5] Another study in a teaching hospital in Pakistan showed 68% of the doctors were not satisfied with their jobs and workload.[6] Female doctors had significantly lower satisfaction with their workload.[7] The magnitude of the problem was further emphasized in the report of the American Foundation for Suicide Prevention, which claimed that on the average, death by suicide is about 70% more likely among male physicians than among other professionals and 250-400% higher among female doctors.[8] Higher levels of stress are also seen in the majority of the nurses.[9]
Stress management programs such as meditation, yoga, hypnosis, imagery, muscle relaxation, have shown improvement in positive coping skills.[10] Progressive muscle relaxation (PMR) technique developed by Dr. Edmund Jacobson is a technique for reduction of stress and anxiety.[11] Muscle tension accompanies anxiety; one can reduce anxiety by learning how to relax the muscular tension.[11] This technique is easy to learn and requires no constant guidance. Once the individual learns the correct way of doing PMR he/she can continue doing it to relieve the tension in the muscles.
The present study was conducted to detect stress levels among female health care professionals in the age group of 25-35 years and its impact on health and to employ early life-style modifications, i.e., PMR training, to improve the quality-of-life.
Subjects and Methods
This prospective cross-sectional pilot project was conducted in a tertiary care hospital in Eastern India in a time span of 1 year, after receiving approval from the Institutional Ethics Committee. Informed consent was taken from the subjects.
Inclusion criteria
Female health care professionals in the age group of 25-35 years were selected. The study subjects were graduate female doctors and nurses, both married and unmarried, working in rural hospitals. Due to lack of trained manpower and poor infrastructure, one has to take extra burden of long duty hours and emergency duties day, night and evening schedules. More often only 2 persons have to continue duties for the whole week in one ward/section (duty hours extend to 84 h/week). Since, the pay does not include extra remuneration for these extra duties; they are frustrated and stressed out. In such situations, one cannot dream to get compensatory leave. Further due to inadequate rest and leisure time they cannot adequately prepare to take up competitive exams for post graduate courses to improve their career. This also is an added stress.
Exclusion criteria
Subjects suffering from chronic debilitating diseases such as cardiac arrhythmias, hypertension, diabetes, ischemic heart disease, retinopathy, nephropathy, or respiratory diseases, smokers, persons receiving any drug that may affect the autonomic reflexes were excluded. Subjects on treatment from psychiatry problem, pregnant women, puerperal mothers, sportswomen, yogis, subjects on regular meditation and exercise regime were excluded. Women on oral contraceptives were not included.
Methods
Sampling was performed using multistage and random cluster method. The first stage of sampling included a simple random sample to select five institutions with female health-care professionals in the region. In the second stage of sampling, 20 subjects were randomly selected from each institution, who were then administered questionnaires.[10,12]
On the first appointment, history of the subjects was carefully recorded. Subjects were asked to tally a list of 43 life events based on a relative score. Stress level in the subjects was assessed according to the presumptive life event stress scale.[12]
Accordingly, they were categorized into no stress, less/moderate stress and severe stress. Score stress up to 40: No stress; 41-200 less/moderate stress; more than 200 severe stress. Finally, 64 females with scores above 200 were selected for the study, as they had a higher risk of developing illness.[12]
The Perceived Stress Scale (PSS) of Sheldon Cohen, the most widely used psychological instrument for measuring the perception of stress, was used. It is a measure of the degree to which situations in one's life are appraised to be stressful. Items were designed to find how unpredictable, uncontrollable and overloaded respondents find their lives. The scale also includes a number of direct queries about current levels of experienced stress. The questions in the PSS ask about feelings and thoughts during the last month. It comprises of 10 items, four of which are reverse-scored, measured on a 5-point scale from 0 to 4. PSS scores are obtained by reversing responses (e.g., 0 = 4, 1 = 3, 2 = 2, 3 = 1 and 4 = 0) to the four positively stated items (items 4, 5, 7 and 8) and then summing across all scale items. Total score ranges from 0 to 40.[9]
Later clinical examinations were conducted and pre-test instructions were given to avoid consumption of any drugs that may alter the autonomic function 48 h prior to test, subjects were advised to have a good restful sleep. The subjects were advised to have a light dinner at 8 p.m. and go to bed early and avoid stressful situations during the day before the tests were conducted. Relaxing bedtime routine, such as soaking in a hot bath or hot tub and then reading a book or listening to soothing music, was advised. They were asked to avoid caffeine (e.g., coffee, tea and soft drinks, chocolate), nicotine (e.g., cigarettes, tobacco products) and alcohol close to bedtime.
On the day of the test, no cigarette, nicotine, coffee, or drugs was permitted. Fasting blood samples were drawn to exclude diabetes. Baseline anthropometric measurements, electrocardiogram (ECG) and lipid profile analysis were carried out. Body mass index (BMI) was recorded for each subject. Among the 64 subjects, three had pathological waveforms in ECG and in two of them, fasting sugar was more than the normal level. Hence, they were excluded from the study. Ultimately, 61 were included in the study. The tests were performed at controlled room temperature in the morning between 10 a.m. and 11 a.m.
Subjects had a light breakfast at least 3 h prior to exercise testing and at least 24 h of abstinence from any form of alcohol, tobacco, tea and coffee. It was ensured that they had not undergone any strenuous work or exercises 3 h prior to the tests.
Resting pulse rate and blood pressure were measured. Physical fitness index (PFI), breath holding time (BHT), isometric hand grip (IHG) test results were evaluated.
PFI
The metronome was set at a rate of 90/min. A wooden bench of 18 inch height was used. The subject was demonstrated the stepping cycle in rhythm with the step frequency. That is, to start with, the subject places one foot on the bench followed by the other foot; then the first foot is brought back down to the floor followed by the other foot, i.e., up-up-down-down. Duration of the test was set at 4 min. The subject was closely watched for any signs of discomfort or any of the indications to stop the test. Immediately after finishing the test, the subject's pulse rate was counted using radial artery. The radial pulse was again counted at intervals of 1-1½, 2-2½ and 3-3½ min of completing the test to evaluate the PFI. The PFI was evaluated by using the formula:[13,14]
PFI = Duration of test in seconds × 100/2 × Sum of pulse count of 1-1½, 2-2½ and 3-3½ min
BHT
The subject was first explained and demonstrated the technique for breath holding. She was asked to inhale maximally then hold his breath until breaking point was reached, i.e., the point when the subject could no longer hold his breath. The subject was motivated to maximize the breath holding period. The time was noted in seconds by using a stop watch and the value was rounded off to integers. A minimum of three trials were given with a rest period of 3 min between the trials and the highest of three similar best performances was taken for statistical analysis.[13,14]
IHG test
Basal blood pressure was measured. Then, the subject was asked to perform maximum grip of the handgrip dynamometer in a sitting position with her dominant hand and the maximum capacity was noted. After 5 min, the subject was asked to hold her grip with 30% of the maximum capacity for 5 min and the blood pressure was recorded just after release of the grip. The rise in diastolic blood pressure (DBP) was calculated and taken as the result of IHG test.[14]
All subjects were given training of PMR. Training involved tensing the specific muscle groups for 7-10 s, followed by releasing them (relaxing) for 15-20 s as per Jacobson's protocol.[11] They were asked to practice this technique at home for 20 min every day for 3 months and come for follow-up. Subjects were followed up at regular intervals during this period. Four subjects did not turn up for follow-up so they were excluded. Therefore, the final sample consisted of 57 subjects.
After 3 months, the lipid profile and vital parameters were rechecked and subjects were asked to repeat the same exercise. The vitals were recorded in a similar fashion.
The computer software “Statistical Package for the Social Sciences (SPSS) version 16 (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, SPSS Inc.)” was used to analyze the data, and paired t-test was used. The data was considered significant and highly significant if the analyzed probability values (P values) were < 0.05* and P < 0.01** respectively.
Results
A total of 100 female subjects were asked to tally a list of 43 life events. Sixty four females with scores > 200 were chosen for the study. Among the 64 subjects, three had pathological waveforms in ECG and in two of them; fasting sugar was more than the normal level. Hence, they were excluded from the study. Sixty one were included in the study. Four subjects did not turn up for follow-up so they were excluded. Therefore, the final sample consisted of 57 subjects.
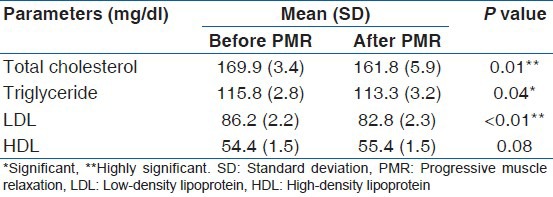
Mean age of the subjects was 30 (1.6) years, BMI was 21.1 (1) kg/m2 and fasting blood sugar was 86 (2.4) mg/dl. Significant decreases in resting heart rate (HR: Pre 75.3 [1.9] beats/min vs. post 71.8 [1.5] beats/min), systolic blood pressure (SBP: Pre 126 [4.4] mm of Hg vs. post 120.1 [2.9] mm of Hg), diastolic blood pressure (DBP: Pre 80.1 [1.8] mm of Hg vs. post 75.8 [1.7] mm of Hg) and Perceived Stress Score levels (PSS: Pre 21.1 [2.2] vs. post 13.8 [1.2]) were seen after PMR training in the subjects [Table 1]. Results of BHT (BHT: Pre 40.5 [4.3] vs. post 44.5 [2]), IHG tests (IHG: Pre 17.7 [2.4] vs. post 19.3 [1.3]) and PFI (PFI: Pre 80.4 [7.2] vs. post 85.5 [4.8]) were significantly increased after PMR training. There was a significant decrease in total cholesterol, triglyceride and low-density lipoprotein (LDL) cholesterol in subjects after practicing PMR for 3 months [Table 2].
Table 1.
Comparison of vital parameters of subjects before and after practicing PMR
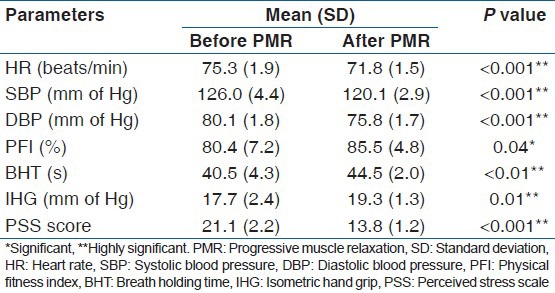
Table 2.
Effect of PMR on the lipid profile
Discussion
Depression is the most common mental illness experienced by women. It is by far more prevalent among women than men with women being twice as likely as men to experience depression. It has been observed in different studies that female health care professionals perceive more stress as compared to males.[6,7,8] Work stress and burnout remain significant concerns in female health care professionals, affecting both individuals and organizations. For the individuals, regardless of whether stress is perceived positively or negatively, the neuroendocrine response yields physiologic reactions that may contribute to illness.[9] In the health care organization, work stress may contribute to absenteeism and turnover, both of which detract from the quality of care. Unless, the health care setups acknowledge the problem and take preemptive steps to tackle the growing menace of chronic stress, personnel costs will keep rising and add to the already soaring costs of care and adversely affect patient outcome. Hence, the present study was conducted to implement a relaxation technique to reduce stress.
Fear of mistakes and litigations are becoming increasingly important in the medical profession. Incidence of psychosomatic illness increased with the level of stress. Burnout was found to be less if females worked the number of hours they preferred. Similar causes of stress in health care professionals have been reported in earlier studies.[5,6,7,8,9]
In the present study, PMR training significantly reduced PSS, total cholesterol, LDL, triglycerides. In an article in 2008, Vyas et al. showed that Raja yoga meditation lowers serum cholesterol and LDL-cholesterol in women thus reducing the risk of CAD.[15] PMR also lowers serum cholesterol and LDL-cholesterol and thereby reduces the risk of CAD.[16] Decrease in Cholesterol, Triglyceride, LDL cholesterol may be a reflection of reduced cortisol levels and decreased sympathetic activity following PMR training.[16]
Among PMR long-term benefits, the following are included: Reduction of salivary cortisol levels and generalized anxiety, decreased blood pressure and HR, decreased headaches, better management of cardiac rehabilitation.[16] We also observed decrease in blood pressure and HR in our subjects after practicing PMR for 3 months.
PMR produces reliable short-term as well as long-term changes in heart rate variability (HRV).[17] Heart rhythm coherence (HRC)-a stable, sine-wave-like pattern in the HRV waveform. It is the pattern of the heart's rhythm that is primarily reflective of the emotional state. This method provides an accurate measure of coherence that allows for the nonlinear nature of the HRV waveform over time. HRC also increases significantly with PMR.[17] These may be a result of decreased sympathetic activity and increased vagal activity following relaxation therapy.[11] LDL cholesterol is known to decrease baroreceptor sensitivity and total cholesterol decreases HRV and reduction of LDL cholesterol and total cholesterol following relaxation exercises may contribute to increases in HRV.[16] In our study, IHG tests were significantly decreased following PMR practice and BHT was significantly increased. In a study by Madanmohan et al. showed that yoga training reduces stress and improves results of IHG test.[14] Yogic practices and relaxation exercises have been found to improve PFI in healthy individuals.[10,11,18,19] Physical fitness is the ability to carry out daily task with vigor and alertness, without undue and ample energy to enjoy leisure time pursuits and to meet unforeseen emergencies. PMR training in our study also significantly improved PFI. Relaxation are attempted in order to reduce pain perception and tension, create a pleasant mental state, increase parasympathetic activities, increase knowledge concerning muscle tension and autonomous stimuli, improve concentration, increase the feeling of control, improve the ability to block inner talk, energize and improve sleep, enhance performance of physical activities and help in the relationship with others, these may contribute in improving PFI.[10,11]
Limitations and future scope of the study
Graduate female health-workers were only included. This may be a limitation of our study as they represent a small cross-section of the population in a developing country. The fact that there is no control group does compromise the results, but the results show positive trends. Future projects with larger samples representing all categories of the population are on the way.
Conclusions
Increase in stress levels are found in female health care professionals in the Eastern part of India due to shortage of manpower, lack of infrastructure, long emergency duty hours and inadequate remuneration for their hard work. Practicing relaxation exercises has shown to improve not only the stress levels but the quality of their life and most important patient care.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Von Känel R. Psychological distress and cardiovascular risk: What are the links? J Am Coll Cardiol. 2008;52:2163–5. doi: 10.1016/j.jacc.2008.09.015. [DOI] [PubMed] [Google Scholar]
- 2.Kohli P, Gulati M. Exercise stress testing in women: Going back to the basics. Circulation. 2010;122:2570–80. doi: 10.1161/CIRCULATIONAHA.109.914754. [DOI] [PubMed] [Google Scholar]
- 3.Lopez-Ruiz A, Sartori-Valinotti J, Yanes LL, Iliescu R, Reckelhoff JF. Sex differences in control of blood pressure: Role of oxidative stressin hypertension in females. Am J Physiol Heart Circ Physiol. 2008;295:H466–74. doi: 10.1152/ajpheart.01232.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rosengren A, Hawken S, Ounpuu S, Sliwa K, Zubaid M, Almahmeed WA, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet. 2004;364:953–62. doi: 10.1016/S0140-6736(04)17019-0. [DOI] [PubMed] [Google Scholar]
- 5.Al-Lamki L. Stress in the medical profession and its roots in medical school. Sultan Qaboos Univ Med J. 2010;10:156–9. [PMC free article] [PubMed] [Google Scholar]
- 6.Khuwaja AK, Qureshi R, Andrades M, Fatmi Z, Khuwaja NK. Comparison of job satisfaction and stress among male and female doctors in teaching hospitals of Karachi. J Ayub Med Coll Abbottabad. 2004;16:23–7. [PubMed] [Google Scholar]
- 7.Richardsen AM, Burke RJ. Occupational stress and job satisfaction among physicians: Sex differences. Soc Sci Med. 1991;33:1179–87. doi: 10.1016/0277-9536(91)90234-4. [DOI] [PubMed] [Google Scholar]
- 8.Familoni OB. An overview of stress in medical practice. Afr Health Sci. 2008;8:6–7. [PMC free article] [PubMed] [Google Scholar]
- 9.Kane PP. Stress causing psychosomatic illness among nurses. Indian J Occup Environ Med. 2009;13:28–32. doi: 10.4103/0019-5278.50721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sharma VK, Trakroo M, Subramaniam V, Rajajeyakumar M, Bhavanani AB, Sahai A. Effect of fast and slow pranayama on perceived stress and cardiovascular parameters in young health-care students. Int J Yoga. 2013;6:104–10. doi: 10.4103/0973-6131.113400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Varvogli L, Darviri C. Stress management techniques: Evidence-based procedures that reduce stress and promote health. Health Sci J. 2011;5:74–89. [Google Scholar]
- 12.Mannapur B, Dorle AS, Hiremath LD, Ghattargi CH, Ramadurg U, Kulkarni KR. A study of psycological stress in undergraduate medical students at S.N. Medical College, Bagalkot, Karnataka. J Clin Diagn Res. 2010;4:2869–74. [Google Scholar]
- 13.Madanmohan, Udupa K, Bhavanani AB, Vijayalakshmi P, Surendiran A. Effect of slow and fast pranayams on reaction time and cardiorespiratory variables. Indian J Physiol Pharmacol. 2005;49:313–8. [PubMed] [Google Scholar]
- 14.Madanmohan, Mahadevan SK, Balakrishnan S, Gopalakrishnan M, Prakash ES. Effect of six weeks yoga training on weight loss following step test, respiratory pressures, handgrip strength and handgrip endurance in young healthy subjects. Indian J Physiol Pharmacol. 2008;52:164–70. [PubMed] [Google Scholar]
- 15.Vyas R, Raval KV, Dikshit N. Effect of Raja yoga meditation on the lipid profile of post-menopausal women. Indian J Physiol Pharmacol. 2008;52:420–4. [PubMed] [Google Scholar]
- 16.Sheu S, Irvin BL, Lin HS, Mar CL. Effects of progressive muscle relaxation on blood pressure and psychosocial status for clients with essential hypertension in Taiwan. Holist Nurs Pract. 2003;17:41–7. doi: 10.1097/00004650-200301000-00009. [DOI] [PubMed] [Google Scholar]
- 17.Leonaite A, Vainoras A. Heart rate variability during two relaxation techniques in post-MI men. Electron Electr Eng Kaunas Technologija. 2010;5:107–10. [Google Scholar]
- 18.Yokesh TP, Chandrasekaran K. Effect of yogic practice on selected physical fitness among overweighted school boys. Recent Res Sci Technol. 2011;3:43–5. [Google Scholar]
- 19.Sharma B, Wavare R, Deshpande A, Nigam R, Chandorkar R. A study of academic stress and its effect on vital parameters in final year medical students at SAIMS Medical College, Indore, Madhya Pradesh. Biomed Res. 2011;22:361–5. [Google Scholar]