

Abstract
Background
The Global Burden of Disease (GBD) study is designed to give a comprehensive and standardized assessment of the health of populations around the world. It measures the burden of disease by considering years of life lost due to premature death as well as years lived with disability. The findings enable the identification of secular trends and disparities between countries and can serve as a basis for decision-making in health policy.
Methods
In cooperation with the authors of the GBD study, we summarize the key methods used to assess the burden of disease in terms of disability-adjusted life years (DALYs). We present findings that specifically pertain to Germany, drawn from freely available data of the most recent round of analysis for the years 1990 and 2010.
Results
According to the GBD study, life expectancy in Germany rose from 75.4 years in 1990 to 80.2 years in 2010. Ischemic heart disease and back pain caused the largest number of DALYs lost (2.5 million and 2.1 million, respectively). Over the period of the study, the absolute number of DALYs due to ischemic heart disease dropped by 33%, while the number of DALYs due to low back pain rose by 11%. Nutrition-related risks ranked first among all risk factors considered, accounting for 13.8% of total DALYs, followed by high blood pressure and high body-mass index, accounting for 10.9% each.
Conclusion
In Germany, important changes have been seen over time in the burden of disease attributable to different chronic diseases. Some of these changes reflect the successful interventions of the past, while others indicate a need for new action. The data from Germany that went into the GBD study must be systematically assessed and supplemented by further data relating to questions of specific relevance in this country.
The original Global Burden of Disease Study, conducted in the late 1980s, represented the first attempt to paint a comprehensive and comparative picture of health and disease in the world population. In the intervening years the method of measuring the burden of disease has been applied both in developing and in developed nations (1– 4). The focus is not on the health/disease of individual persons; rather, calculations of disease burden are carried out at the population level. Disease burden data can be used—with due consideration of the known methodological limitations—to aid decision-making processes in the area of health policy. Burden of disease studies use summary measures that combine epidemiological data on mortality and morbidity in one single metric, thus rendering heterogeneous disease states comparable (5, 6).
The new GBD study, carried out by the Institute for Health Metrics and Evaluation (Seattle, USA), presents findings covering the period 1990 to 2010 and provides the first completely revised, comprehensive, and comparative overview of the global health/disease situation (7, 8). The study uses modern Bayesian modeling techniques to combine epidemiological data on disease occurrence, disease consequences, and risk factors in order to improve the conclusiveness of the findings. Some nations (e.g., China and the UK) have already utilized the country-specific GBD 2010 results to:
Analyze country-specific health trends over time
Pinpoint successes and challenges in the fields of medicine and public health
Benchmark with other countries
Identify potential areas for improvement in public health and draw up recommendations for action (9, 10).
Although many nations worldwide have meanwhile investigated disease burden and quantified health deficits with the aid of summary measures, particularly the disability-adjusted life year (DALY), to date Germany's participation in international debate has been modest and the GBD methodology has been employed only selectively (11– 13).
This article therefore sets out to portray the basic methodology of the GBD study and to describe and discuss the freely available data for Germany from GBD 2010. Previous publications have mostly focused on the global findings, and no comprehensive account of the burden of disease in Germany is yet available. This paper aims to present the major causes of the disease burden in Germany, the corresponding risk factors, and the trends over time. We also compare the disease burdens of a selected set of European countries, including Germany.
Methods
The data sources, statistical analyses, and modeling procedures employed have been previously described in great detail by the authors of the GBD 2010 Study (8, 14– 20). We therefore confine ourselves to the key points of the methods.
GBD 2010 employed the summary measure DALY, combining epidemiological data on mortality and morbidity in one measure (see eBox 1 for details of the DALY and eBox 2 for the basic methodology of the study).
Key Messages.
Despite certain methodological limitations, use of the measure “disability-adjusted life year” enables overall evaluation of the health of populations.
With its consistently applied methods, the Global Burden of Disease Study 2010 showed that trends in the importance of diseases and risk factors could be followed from 1990 to 2010.
The most important causes of loss of healthy years of life in Germany are, by far, ischemic heart disease and low back pain. Overall, there is a shift away from life years lost to premature death towards life years affected by health impairments.
The complex of nutrition-related risks is currently the most important risk factor in Germany, followed by high blood pressure and high body mass index.
The validity of the results of the GBD 2010 study for Germany could be improved by including the results obtained by continuous national health monitoring as established at by the Robert Koch Institute in 2008 with funding of the Federal Ministry of Health, and adaptation of the analyses to the specific situation in Germany.
eBox 1. Basic parameters and calculation of DALYs.
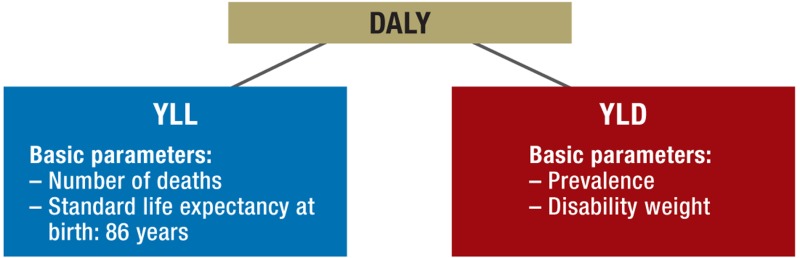
The DALYs comprise two complementary components, years of life lost due to premature death (YLLs) and years lived with disability (YLDs). The unit of measurement is lost years of healthy life.
In the context of burden of disease studies, the term “disability” is used to mean any quantifiable (percentage) deviation from optimal health status.
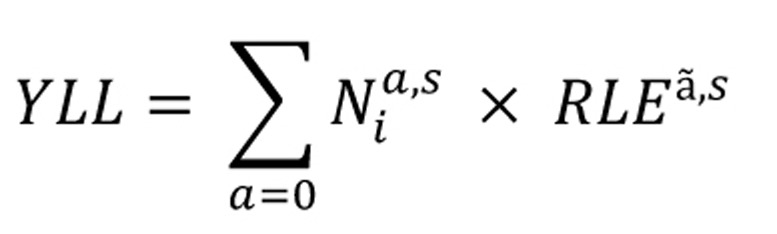
The mortality component (YLLs) is calculated from the number of persons who have died (N) (by age [a], sex [s], and cause of death [i]) and a global standard, valid for both sexes, for the life expectancy at birth (used to estimate the remaining life expectancy [RLE] at the time of death [ã]): (Equation 1)
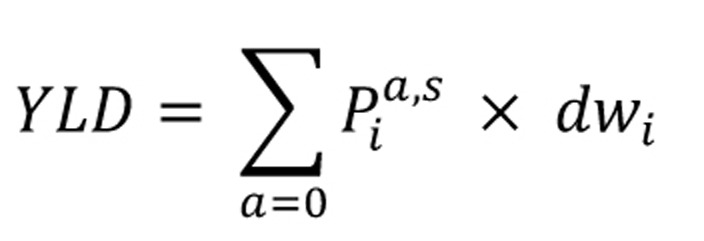
The morbidity component (YLDs) is calculated from the prevalence (P) (by age [a] and sex [s]) of the health-impairing condition being investigated (i) and the disability weight (dw) (Equation 2):
The sum of the YLLs and YLDs gives the DALYs (Equation 3):

-
Disability weights
The first GBD study introduced the concept of disability weights, used to quantify the impact of diseases and injuries on health by measuring impairments of health on a scale of 0 (complete health) to 1 (a state comparable with death). In the GBD 2010 Study health states were evaluated on the basis of population-based studies in which the participants had to weigh health states against each other in pairwise comparisons and decide which was the healthier (17). Therefore the newly derived disability weights (GBD 2010) reflect the perspective of the population, rather than being based on expert opinion.
Main input data on mortality and morbidity
The calculation of DALYs in the GBD study was preceded by an analysis of the basic epidemiological data that would be required. In the framework of the study, data drawn from reviews and subsequent meta-analyses and from publicly available sources were subjected to statistical processing (see, for example, publications on ischemic heart disease [21] and depression [22]). Depending on data quantity and quality, estimates were based primarily on either country-specific data sources or were derived from prediction models accounting for incomplete or qualitatively insufficient data (for details see [8, 18, 23, 24]).
For Germany, the official death registry data and ICD-coded cause of death statistics were used. Various publicly available sources were drawn upon to estimate disease prevalences, because national health monitoring by the Robert Koch Institute (RKI) providing nationally representative prevalence estimates at regular intervals was not set up until 2008 (25).
Disability weights
Alongside the basic parameters, calculation of DALYs requires quantification of the impairment to health resulting from disease or injury. To this end, disability weights were established for all of the health states considered for GBD 2010 with the aid of population-based studies and used uniformly for all 187 nations (eBox 1) (17).
Quantitative parameters
The findings of the GBD 2010 Study for Germany are presented as DALYs, years lived with disability (YLDs), years of life lost (YLLs), life expectancy (LE), and health-adjusted life expectancy (HALE) (26) (for details on summary measures see [5]). All results are given as means or modes with 95% uncertainty intervals (95% UI). Like the confidence interval, the 95% UI reflects estimation-related uncertainties, but additionally accounts for uncertainties from other sources, e. g. modeling uncertainties.
For the present paper we drew data for the disease burden in Germany from the visualization tools of the Institute for Health Metrics and Evaluation (IHME) (27), the Global Health Data Exchange (GHDx) database (28), and additional material provided by the IHME.
Results
(Healthy) life expectancy
According to the calculations of the GBD 2010 Study, the mean LE in Germany increased by 4.8 years from 75.4 (95% UI 75.3 to 75.4) in 1990 to 80.2 (95% UI 80.1 to 80.4) in 2010 (Table 1). Sex-specific analyses (data not shown) revealed that the increase was greater for men than for women: in men the LE rose by 5.6 years, from 71.9 (95% UI 71.8 to 72.0) to 77.5 (95% UI 77.3 to 77.7), in women the LE rose by 4.4 years, from 78.4 (95% UI 78.4 to 78.5) to 82.8 (95% UI 82.6 to 83.1). Thus the difference in LE between women and men decreased by 1.2 years (29). The overall rise in HALE was 3.7 years, markedly below that for total LE (Table 1). Again, the increase was much greater for men (3.9 years) than for women (2.7) during the study period. Among the 15 founding members of the European Union, Germany ranked seventh for LE and HALE in 2010 (Table 1).
Table 1. Trends in (healthy) life expectancy in the 15 founding members of the EU from 1990 to 2010 (28, 29).
| a) | LE | |||||
| Rank*1 | Country | 1990 | 2010 | Change*2 | ||
| 1 | Italy | 77.0 (76.9–77.0) | 81.5 (81.3–81.6) | 4.5 | ||
| 2 | Spain | 76.9 (76.9–77.0) | 81.4 (81.2–81.5) | 4.5 | ||
| 3 | Sweden | 77.6 (77.5–77.7) | 81.4 (81.3–81.5) | 3.5 | ||
| 4 | France | 77.1 (77.0–77.1) | 80.9 (80.7–81.1) | 3.8 | ||
| 5 | Netherlands | 77.0 (77.0–77.1) | 80.6 (80.5–80.7) | 3.6 | ||
| 6 | Austria | 75.7 (75.6–75.8) | 80.6 (80.5–80.7) | 4.9 | ||
| 7 | Germany | 75.4 (75.3–75.4) | 80.2 (80.1–80.4) | 4.8 | ||
| 8 | Luxembourg | 75.3 (75.0–75.6) | 80.2 (79.8–80.5) | 4.9 | ||
| 9 | Finland | 75.1 (75.0–75.2) | 80.1 (79.9–80.2) | 5 | ||
| 10 | Great Britain | 75.7 (75.6–75.7) | 79.9 (79.9–80.0) | 4.2 | ||
| 11 | Ireland | 74.8 (74.7–75.0) | 79.9 (79.7–80.1) | 5.1 | ||
| 12 | Greece | 76.9 (76.8–77.0) | 79.6 (79.4–79.8) | 2.7 | ||
| 13 | Belgium | 75.9 (75.8–76.0) | 79.5 (79.3–79.8) | 3.6 | ||
| 14 | Portugal | 74.3 (74.2–74.4) | 79.4 (79.2–79.5) | 5.1 | ||
| 15 | Denmark | 75.2 (75.0–75.3) | 78.9 (78.8–79.1) | 3.7 | ||
| b) | HALE | Change | ||||
| Rank*1 | Country | 1990 | 2010 | Change*2 | LE-HALE | |
| 1 | Spain | 67.5 (65.7–69.1) | 70.9 (68.9–72.7) | 3.4 | 1.1 | |
| 2 | Italy | 66.7 (64.7–68.5) | 70.2 (68.0–72.1) | 3.5 | 1 | |
| 3 | Sweden | 66.8 (64.9–68.7) | 69.6 (67.4–71.7) | 2.8 | 0.7 | |
| 4 | France | 66.5 (64.6–68.4) | 69.5 (67.3–71.5) | 3 | 0.8 | |
| 5 | Netherlands | 66.5 (64.6–68.3) | 69.1 (67.0–70.9) | 2.6 | 1 | |
| 6 | Austria | 65.8 (63.7–67.5) | 69.1 (66.9–71.2) | 3.3 | 1.6 | |
| 7 | Germany | 65.3 (63.4–67.0) | 69.0 (66.9–70.9) | 3.7 | 1.1 | |
| 8 | Ireland | 65.2 (63.3–67.1) | 68.9 (66.6–70.8) | 3.7 | 1.4 | |
| 9 | Greece | 66.5 (64.4–68.4) | 68.7 (66.5–70.6) | 2.2 | 0.5 | |
| 10 | Great Britain | 65.4 (63.4–67.2) | 68.6 (66.4–70.5) | 3.2 | 1 | |
| 11 | Portugal | 64.4 (62.3–66.2) | 68.6 (66.3–70.5) | 4.2 | 0.9 | |
| 12 | Belgium | 65.7 (63.6–67.5) | 68.5 (66.4–70.5) | 2.8 | 0.8 | |
| 13 | Luxembourg | 65.2 (63.1–67.1) | 68.4 (65.9–70.5) | 3.2 | 1.7 | |
| 14 | Denmark | 65.3 (63.3–67.1) | 67.9 (65.8–69.8) | 2.6 | 1.1 | |
| 15 | Finland | 63.8 (61.6–65.9) | 67.3 (64.8–69.6) | 3.5 | 1.5 | |
Mean values (incl. 95% UI); *1 based on mean for 2010; *2 based on change in mean;
LE, life expectancy; HALE, health-adjusted life expectancy
Mortality
The GBD 2010 Study showed that ischemic heart disease (195 797 deaths) was by far the most common cause of death in Germany in 2010 (eFigure 1). This was true both for women (99 364 [95% UI 90 760 to 122 070]) and for men (96 433 [95% UI 89 980 to 110 219]). The second most common overall cause of death was stroke (76 291 deaths). In sex-specific analyses, this held true for women, while for men the second leading cause of death was lung cancer. Altogether, cardiovascular diseases played a greater role in women (483 deaths/100 000) than in men (394/100 000) (data not shown) (30).
eFigure 1.

The 20 most frequent causes of death in Germany and how they changed between 1990 and 2010 (incl. 95% UI) (red: group I; blue: group II; green: group III) (30)
*Standardized on the basis of the WHO world population 2001
**Including other dementias
The absolute numbers of deaths from the two leading overall causes of death decreased considerably during the study period, by 24% and 34% respectively (eFigure 1). The age-standardized rates per 100 000 of the population decreased even more, by 47% and 53% respectively. In contrast, the absolute numbers of deaths increased for lung cancer (+18%), chronic obstructive pulmonary disease (COPD) (+1%), other cardiovascular diseases (+15%), chronic lower respiratory diseases (+13%), diabetes (+1%), and hypertensive heart disease (+2%).
The increase in the overall absolute number of deaths can be attributed largely to demographic changes in the population, because the age-standardized rates show that all of the 10 most common causes of death are on the decrease. Apart from the 10 leading causes of death the trends for absolute numbers of deaths and age-standardized death rates are rising for several disease groups, including Alzheimer‘s disease and other dementias (+244% and +119% respectively), chronic kidney disease (+106% and +33% respectively), and atrial fibrillation (+501% and +304% respectively) (30).
Disability-adjusted life years
A total of 23.9 (95% UI 22 to 26) million healthy years of life were lost due to disease and injury in Germany in 2010, 52.7% of them in men. Compared with 1990 (25.7 million DALYs), the absolute number of DALYs went down by 7.3% and the age-standardized DALYs decreased from 25 197 (95% UI 23 299 to 27 306) to 19 527 (95% UI 17 646 to 21 560) per 100 000 of the population (31).
At the first level of the GBD classification system, 3.5% (circa 0.83 million DALYs) of the total burden of disease in Germany could be attributed to group I (communicable, maternal neonatal and nutrional disorders), 88.1% (circa 21 million DALYs) to group II (non-communicable diseases), and 8.4% (circa 2 million DALYs) to group III (injuries) (31).
At the second level of the GBD classification system (21 major disease groups), the most important disease groups are cardiovascular and circulatory diseases (19.4%), malignant neoplasms (17.9%), musculoskeletal disorders (15.8%), and mental and behavioral disorders (11.4%). Stratification by sex shows that the leading cause of lost healthy years in women is not cardiovascular diseases but musculoskeletal disorders (Table 2a and b) (31).
Table 2a. Burden of disease for the 21 major disease groups on the second level of the GBD classification system (Germany 2010) (30).
| Men | ||||
|---|---|---|---|---|
| Rank | Cause | DALY | YLL | YLD |
| 1 | Cardiovascular and circulatory diseases | 2551248 | 2252040 | 299208 |
| 2 | Cancer | 2452880 | 2375480 | 77400 |
| 3 | Musculoskeletal disease | 1679000 | 16860 | 1662140 |
| 4 | Mental and behavioral disorders | 1305863 | 192543 | 1113320 |
| 5 | Diabetes, urogenital, blood-related and endocrine disorders | 733326 | 320654 | 412672 |
| 6 | Unintentional injury | 614616 | 183137 | 431479 |
| 7 | Chronic respiratory diseases | 578996 | 325573 | 253423 |
| 8 | Other non-communicable diseases | 545057 | 61685 | 484372 |
| 9 | Neurological disorders | 491927 | 202664 | 289263 |
| 10 | Transport injuries | 345240 | 170269 | 174971 |
| 11 | Intentional injuries | 328251 | 310882 | 17369 |
| 12 | Cirrhosis | 292923 | 288070 | 4853 |
| 13 | Diarrhea, lower respiratory tract disease, and other infectious diseases | 255849 | 172406 | 83443 |
| 14 | Digestive diseases | 193883 | 138585 | 55298 |
| 15 | Neonatal disorders | 95752 | 69727 | 26025 |
| 16 | Nutritional deficiencies | 43650 | 5476 | 38174 |
| 17 | HIV/AIDS and tuberculosis | 33241 | 24171 | 9069 |
| 18 | Other communicable diseases | 25528 | 16633 | 8895 |
| 19 | NTDs* and malaria | 5810 | 1794 | 4016 |
| 20 | Maternal disorders | 0 | 0 | 0 |
| 21 | War and desasters | 0 | 0 | 0 |
*NTDs: neglected tropical diseases; DALY, disability-adjusted life years; YLL, years of life lost due to premature death; YLD, years lived with disability
Table 2b. Burden of disease for the 21 major disease groups on the second level of the GBD classification system (Germany 2010) (30).
| Women | ||||
|---|---|---|---|---|
| Rank | Cause | DALY | YLL | YLD |
| 1 | Musculoskeletal disease | 2092654 | 23344 | 2069310 |
| 2 | Cardiovascular and circulatory diseases | 2072319 | 1788880 | 283439 |
| 3 | Cancer | 1807685 | 1726940 | 80745 |
| 4 | Mental and behavioral disorders | 1460018 | 56358 | 1349660 |
| 5 | Diabetes, urogenital, blood-related and endocrine disorders | 737065 | 277159 | 459906 |
| 6 | Neurological disorders | 664661 | 186003 | 478658 |
| 7 | Other non-communicable diseases | 608604 | 56458 | 552146 |
| 8 | Chronic respiratory diseases | 489 548 | 208274 | 281274 |
| 9 | Unintentional injury | 460015 | 112 969 | 347046 |
| 10 | Diarrhea, lower respiratory tract disease, and other infectious diseases | 233992 | 147256 | 86736 |
| 11 | Digestive diseases | 196593 | 145869 | 50724 |
| 12 | Transport injuries | 147146 | 54811 | 92335 |
| 13 | Cirrhosis | 138381 | 135707 | 2674 |
| 14 | Intentional injuries | 107181 | 102 661 | 4520 |
| 15 | Neonatal disorders | 72358 | 52003 | 20355 |
| 16 | Nutritional deficiencies | 25210 | 7504 | 17706 |
| 17 | Other communicable diseases | 19991 | 12846 | 7145 |
| 18 | HIV/AIDS and tuberculosis | 10900 | 8091 | 2809 |
| 19 | Maternal disorders | 5558 | 2715 | 2843 |
| 20 | NTDs and malaria | 5212 | 4054 | 1158 |
| 21 | War and desasters | 0 | 0 | 0 |
NTDs: neglected tropical diseases; DALY, disability-adjusted life years; YLL, years
At the fourth level of detail, ischemic heart disease (men) and low back pain (women) were identified as by far the most common causes of lost healthy years (eFigure 2). Despite the prominent place occupied by ischemic heart disease, the disease burden in absolute DALYs fell by a median 27% (rate: –52%) in men and 41% (rate: –54%) in women between 1990 and 2010 (efigure 2). In contrast, the absolute DALYs rose by 19% (rate: 2%) in men and by 4% (rate: -3%) in women over the same period.
eFigure 2.

The 10 most frequent causes for DALYs in men and women and the change in burden of disease in Germany between 1990 and 2010 (% change expressed as median) (blue: group II; green: group III) (30)
*Standardized on the basis of the WHO world population 2001
**Other musculoskeletal diseases
With regard to DALY rates, the generally decreasing or moderately increasing tendencies among the 30 most frequent causes of lost healthy years are accompanied by an increase in DALY rates due to Alzheimer‘s disease and other dementias of 26% (from 157 to 198 DALYs/100 000) for men and 16% (from 182 to 210 DALYs/100 000) for women (30).
For ischemic heart disease, the greatest part of the disease burden can be attributed to the YLLs, i.e., to premature deaths. In contrast, all of the low back pain DALYs are due to morbidity effects (YLDs) (Figure 1).The relevance of YLDs for the majority of the 10 most common diseases increased in the period 1990 to 2010 (Figure 1) (30).
Figure 1.

The 10 most important causes of DALYs for men and women in Germany, by YLL and YLD (mean, 2010) (30) DALY, disability-adjusted life years; YLL, years of life lost due to premature death; YLD, years lived with disability; COPD, chronic obstructive pulmonary disease
Germany in comparison with other European countries
Comparison of the founding members of the European Union shows that the three leading causes of DALYs are distributed similarly, with minor deviations, in all 15 countries. However, Germany shows the highest rates for low back pain and is near the top of the rankings for ischemic heart disease and depression (Table 3) (32).
Table 3. Comparison of age-standardized DALY rates per 100000 of the population for the 10 most frequent causes of disease burden (32).
| Rank*1 | DE | BE | DK | FI | FR | GR | UK | IE | IT | LU | NL | A | PT | ES | SE | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Low back pain | 2033 | 1742 (1) | 2014 (1) | 1832 (1) | 1906 (1) | 1806 (1) | 1931 (1) | 1879 (1) | 1570 (1) | 1882 (1) | 1749 (1) | 1910 (1) | 1890 (1) | 1093 (1) | 1982 (1) |
| 2 | Ischemic heart disease | 1406 | 1300 (2) | 1266 (2) | 1585 (2) | 814 (3) | 1711 (2) | 1310 (2) | 1487 (2) | 1019 (2) | 1209 (3) | 980 (3) | 1311 (2) | 960 (2) | 963 (2) | 1202 (2) |
| 3 | Major depressive disorder | 1027 | 842 (3) | 1068 (3) | 1264 (3) | 1014 (2) | 1031 (3) | 656 (5) | 856 (3) | 1024 (3) | 1383 (2) | 1700 (2) | 1056 (3) | 914 (4) | 922 (3) | 1006 (3) |
| 4 | Neck pain | 610 | 613 (7) | 579 (8) | 726 (5) | 609 (8) | 619 (7) | 607 (6) | 616 (4) | 618 (5) | 617 (5) | 609 (6) | 610 (6) | 622 (6) | 610 (5) | 566 (4) |
| 5 | Lung cancer | 576 | 705 (5) | 741 (5) | 387 (13) | 644 (6) | 661 (6) | 595 (7) | 536 (8) | 505 (9) | 581 (7) | 734 (4) | 519 (8) | 447 (11) | 534 (7) | 371 (17) |
| 6 | Falls | 560 | 602 (9) | 566 (9) | 656 (7) | 593 (9) | 567 (8) | 559 (8) | 570 (6) | 549 (6) | 601 (6) | 546 (7) | 611 (4) | 565 (8) | 535 (9) | 548 (5) |
| 7 | Other musculoskeletal conditions | 531 | 532 (11) | 544 (11) | 528 (10) | 540 (10) | 513 (9) | 542 (11) | 537 (9) | 520 (8) | 526 (9) | 533 (8) | 526 (9) | 532 (9) | 546 (6) | 524 (6) |
| 8 | Road injuries | 514 | 766 (4) | 554 (10) | 528 (9) | 633 (7) | 895 (5) | 500 (13) | 551 (7) | 657 (4) | 611 (4) | 458 (11) | 600 (5) | 709 (5) | 597 (4) | 447 (9) |
| 9 | Stroke | 488 | 557 (10) | 638 (7) | 592 (8) | 453 (12) | 939 (4) | 542 (10) | 508 (10) | 537 (7) | 573 (8) | 495 (10) | 491 (13) | 975 (3) | 505 (10) | 484 (8) |
| 10 | Anxiety disorders | 495 | 360 (15) | 381 (16) | 437 (16) | 675 (4) | 498 (10) | 555 (9) | 408 (13) | 368 (13) | 588 (12) | 506 (9) | 374 (17) | 484 (12) | 287 (16) | 471 (11) |
Note: Age-standardized DALY rates (mean) per 100 000 of the population (standardized to WHO world population 2001)
*1Rank in Germany (rank in other countries shown in parentheses)
Risk factors
According to the findings of the GBD 2010 Study the most significant risk factor is the complex of nutrion-related risks, to which can be attributed 13.8% (95% UI 12.3 to 15.4) of the total DALYs and 26% (95% UI 23.4 to 28.4) of all deaths. High blood pressure and high body mass index (BMI) jointly occupy second place, each accounting for 10.9% of total DALYs (31). Within the risk factor cluster of nutrition-related factors (14 individual factors) (20), the most important in Germany are diets low in nuts, fruits, and seeds or high in sodium (31).
The risk factor complex of nutrition-related factors accounts for 16.2% of DALYs in men, compared with 11.2% in women. Smoking and alcohol abuse are more important factors in men than in women, while high BMI seems to be a more serious risk for women than for men (Figure 2) (31).
Figure 2.

Attributable disease burden for the 10 principal risk factors in Germany, 2010 (stratified by sex, with error bars showing the 95% UI) (30, 31).
BMI, body mass index; PM, particulate matter; DALYs, disability-adjusted life years
The disease burden attributable to all 10 most frequent risk factors decreased considerably over the study period, with regard to both absolute DALYs and age-standardized DALY rates. The highest reductions in rates were seen for air pollution (-67%; 95%UI –70 to –64), high total cholesterol (-58%; 95%UI –70 to –46), and high blood pressure (-54%; 95%UI –61 to –46) (data not shown) (31).
Discussion
The results of the GBD 2010 Study indicate changes in the importance of chronic diseases and reflect demographic trends and intervention effects. Comparison of LE with HALE clearly shows that residents of Germany are living longer than in 1990, but that a portion of the extra years of life is spent in a state of reduced health. Altogether, there is a pronounced shift of disease burden towards morbidity effects (YLDs). On one hand this represents a success, because for example fewer people are dying of myocardial infarction, but on the other hand it is a challenge, because patients living with the long-term consequences of coronary heart disease have to receive appropriate care.
One notable trend between 1990 and 2010 was the increase in the importance of back pain in both women and men. Although the health surveys of the RKI show that the prevalence of low back pain was considerably higher in women than in men in the years 2003 and 2009 (33), GBD 2010 reveals a higher disease burden for men.
Looking at the input data it was identified that data for Germany were only included up to 2006; for later years, estimates were derived from prediction models that contained no actual data from Germany. This explains why the uncertainty intervals are large and indicate limited data.
Comparison of the GBD 2010 findings with the official causes of death statistics shows that ischemic heart disease is the leading cause of death in both data sources. The number of deaths cannot be compared ad hoc because of the correction algorithms applied in the estimation process for causes of death in the GBD study (34, 35).
The increase in the burden of disease imposed by Alzheimer‘s disease and other dementias is striking. At the same time, dementias exemplify how important it is for estimates of trends in disease burden to be accompanied by detailed monitoring of disease incidence and prevalence and of the prevalence of the principal risk factors. Numerous factors (demographic trends, progress in the prevention of cardiovascular disease, advances in diagnosis and treatment) can influence incidence, prevalence, and mortality in many different ways (36, 37).
According to the GBD 2010 Study, poor nutrition is responsible for the loss of many healthy years of life, particularly through premature death (2.8 [95% UI 2.6 to 3.1] million YLLs). Despite the general decrease in overall disease burden, nutrition-related factors remained by far the greatest risk in 2010, and preventive measures as well as public awareness campaigns should be tailored accordingly. Inadequate nutrition favors risk factors such as hypertension, impaired glucose tolerance, high BMI, and high cholesterol. In view of the complexity of nutrition-related health risks, it is important to observe the prevalence of particular patterns of nutrition and also of individual components (e.g., salt and alcohol) at the population level and ascertain their contribution to impairments of health.
Limitations and recommendations
The new GBD 2010 Study provides many advances in the comprehensive analysis of health trends at the population level. One crucial limitation, however, is that so far regularly collected data representative of the population in Germany have not continuously been available, so that the investigators have had to rely on freely accessible data. As already shown in other country-specific analyses (e.g., China and Turkey), countries often possess further national and regional health data that can help to improve the quality of the models and the validity of the estimates (Christopher Murray, personal communication).
For example, data collected in Germany as part of the RKI‘s national health monitoring (e.g., the German Health Interview and Examination Survey for Adults [DEGS]) were not included in GBD 2010, although they will be included in ongoing GBD analyses. Looking at the DALYs for Germany, it is noticeable that the uncertainty intervals for some diseases are very wide. This can be attributed in part to the limited availability or insufficient quality of the data.
It is important to point out that international data also feature considerable variations of uncertainty intervals, and this should always be borne in mind when comparisons are made. For this reason the international efforts to establish mandatory standards in the acquisition and analysis of health data (especially morbidity data) should be intensified, in order to improve the basis for the calculation of DALYs and thus the validity of international comparisons.
The data sources used for Germany should now be carefully reviewed—as already described for low back pain—and the gaps filled, to provide a broader and stronger basis for the German results. In this regard, sub-national analyses of the disease burden would be very useful in identifying any variation in the distribution of the burden in different parts of the country. Close cooperation between health institutions in Germany and the organizers of the GBD study would be beneficial in setting up a concerted national burden of disease study for Germany (NBD Germany). This study should include analyses of the methodological, ethical, and legal aspects of disability weights (38).
Disability weights constitute a very important aspect of the calculation of DALYs and have been criticized particularly with regard to the universal application of global disability weights, as well as certain methodological limitations. The criticism has focused on the way in which the descriptions of health states in the population-based studies were formulated so as to be comprehensible to a layperson, which may, for instance, possibly have led to the establishment of relatively low disability weights for severe visual impairment or blindness (39).
Conclusion
Comprehensive analyses and evaluations of trends in the health status of populations along the lines of the Global Burden of Disease Study are also helpful for individual countries, providing insight into major changes in population health and new challenges in prevention and care. The crucial prerequisites are availability of data, adaptation to the circumstances of the country concerned, and refinement of the methods. In Germany, the nationwide health monitoring by the Robert Koch Institute provides a good basis for initiating a national burden of disease study (NBD Germany) in cooperation with German and international partners.
eBox 2. Methods of the GBD 2010 study.
-
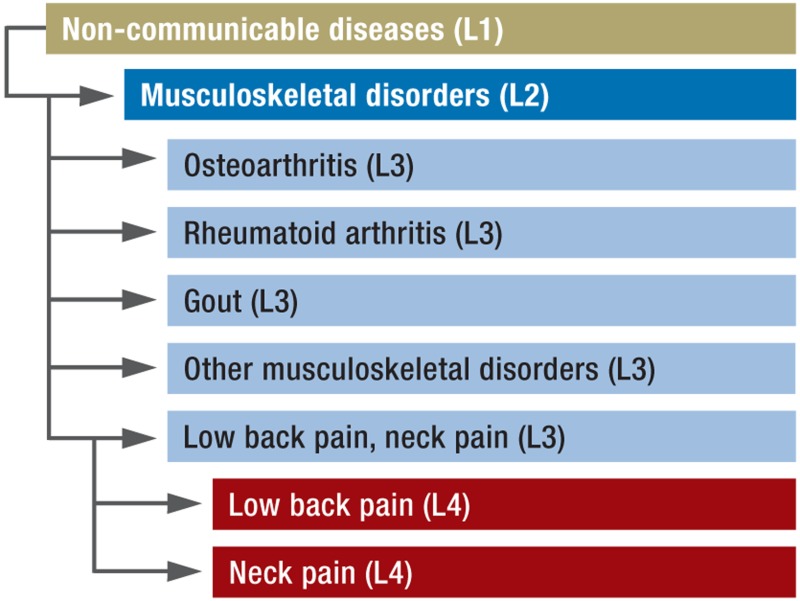
Classification of diseases and injuries
The GBD classification is a tree-like structure with five levels of disaggregation. At the highest level (level 1) are the entities of groups I, II, and III. Group I entities include communicable, maternal, neonatal and nutritional disorders. Group II comprises non-communicable diseases, and group III is made up of injuries. The burden of disease is differentiated into 21 major groups (level 2) and further into individual disease endpoints (levels 3 to 5) depending on the detail required (see example for musculoskeletal diseases). The GBD classification is structured in such way that all codes contained in the International Classification of Diseases (ICD) can be clearly assigned to a group at each level of the GBD classification system (24).
-
Parameters
Alongside the disability-adjusted life years (DALYs) and their two components, the years of life lost due to premature death (YLLs) and years lived with disability (YLDs), the GBD study employs an indicator for healthy life expectancy, the health-adjusted life expectancy (HALE). This measure represents the life expectancy free of health impairments and is thus a suitable parameter for estimation of the effects on life expectancy of changes in population morbidity (16, 24).
-
Prevalence
The YLDs are established on the basis of the prevalence of diseases and injuries. The reason for this is that present needs in health care (e.g., for resources) are depicted better by prevalence than by incidence. This is particularly true when incidence is decreasing but prevalence is constant or rising slightly (24).
-
Standard life expectancy
The life expectancy at birth was calculated on the basis of the lowest mortality rate observed anywhere in the world and determined as 86 years. The life expectancy at birth was set the same for both sexes because, although differences can be observed, (a) the difference in life expectancy between men and women is continuing to shrink and (b) the goal should be to attain the highest possible life expectancy regardless of sex. The GBD study thus proceeds from the assumption that all people, whatever their origin, ethnicity, or sex, should be able to reach the age defined as standard (24).
-
Age weighting and time discounting
On ethical grounds, these two concepts from economic theory were not used for calculation of the burden of disease in the GBD 2010 Study (24).
-
Uncertainty intervals
The intensified recourse to modeling methods makes it essential to quantify the uncertainty intervals. These enable portrayal in the final results of all uncertainties present in the input data and arising from modeling processes. The uncertainty intervals reflect, in addition to the estimation-related uncertainty depicted in conventional confidence intervals, uncertainties from other sources, e.g., from modeling. The results are expressed as means or modes with 95% uncertainty intervals.
-
Trends over time
The methods of the GBD 2010 Study were applied consistently throughout the period 1990 to 2010. This enabled, for the first time, identification of changes and trends in disease burden (24).
-
Comorbidities
Because of the increasing role of comorbidities, potential accompanying conditions were depicted at population level on the basis of microsimulation models. In a second step, the disability weights were adjusted (in a multiplicative approach) to take into account the severity of comorbid states (24).
-
Risk factors
As for the epidemiological parameters, data on the 67 investigated risk factors (exposure, exposure effect estimator) were derived from existing databases and literature reviews. The attributable disease burdens were estimated by means of comparative risk assessment, in which a proportion of the disease-specific burden is attributed to a particular risk factor (20).
-
Correction of cause of death
Incorrectly or unclearly coded causes of death were redistributed with the aid of a standardized algorithm (19, 35).
-
Age standardization
Age standardization was based on the standard world population data for the year 2001 provided by the WHO (40).

Acknowledgments
Translated from the original German by David Roseveare.
Footnotes
Conflict of interest statement
The authors declare that no conflict of interest exists.
References
- 1.Murray CJL, Lopez AD. Cambridge: Harvard School of Public Health on behalf of the World Health Organization and the World Bank; 1996. The Global Burden of Disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. [Google Scholar]
- 2.Bradshaw D, Groenewald P, Laubscher R, et al. Initial burden of disease estimates for South Africa, 2000. South African Medical Journal. 2003;93:682–688. [PubMed] [Google Scholar]
- 3.Michaud C, McKenna M, Begg S, et al. The burden of disease and injury in the United States 1996. Population Health Metrics. 2006;4 doi: 10.1186/1478-7954-4-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.The World Bank. Investing in Health. New York: Oxford University Press; 1993. World Development Report 1993. [Google Scholar]
- 5.Murray CJL, Salomon JA, Mathers CD, Lopez AD. Geneva. World Health Organization: 2002. World Health Organization: Summary measures of population health: concepts, ethics, measurement and applications. [Google Scholar]
- 6.Field MJ, Gold MR. Washington, D.C.: National Academy Press; 1998. Committee on Summary Measures of Population Health: Summarizing population health: directions for the development and application of population metrics. [PubMed] [Google Scholar]
- 7.Murray CJL, Ezzati M, Flaxman AD, et al. GBD 2010: a multi-investigator collaboration for global comparative descriptive epidemiology. The Lancet. 2012;380:2055–2058. doi: 10.1016/S0140-6736(12)62134-5. [DOI] [PubMed] [Google Scholar]
- 8.Murray CJL, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. [DOI] [PubMed] [Google Scholar]
- 9.Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. The Lancet. 2013;381:1987–2015. doi: 10.1016/S0140-6736(13)61097-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Murray CJ, Richards MA, Newton JN, et al. UK health performance: findings of the Global Burden of Disease Study 2010. Lancet. 2013;381:997–1020. doi: 10.1016/S0140-6736(13)60355-4. [DOI] [PubMed] [Google Scholar]
- 11.Penner D, Pinheiro P, Krämer A. Measuring the burden of disease due to premature mortality using Standard Expected Years of Life Lost (SEYLL) in North Rhine-Westphalia, a Federal State of Germany, in 2005. Journal of Public Health. 2010 [Google Scholar]
- 12.Terschuren C, Mekel OCL, Samson R, Classen TKD, Hornberg C, Fehr R. Health status of ’Ruhr-City’ in 2025—predicted disease burden for the metropolitan Ruhr area in North Rhine-Westphalia. Eur J Public Health. 2009:534–540. doi: 10.1093/eurpub/ckp060. [DOI] [PubMed] [Google Scholar]
- 13.Hornberg C, Claßen T, Steckling N, et al. Berlin: Dessau-Roßlau Umweltbundesamt (UBA); 2012. Endbericht zum Forschungsvorhaben: „Quantifizierung der Auswirkungen verschiedener Umweltbelastungen auf die Gesundheit der Menschen in Deutschland unter Berücksichtigung der bevölkerungsbezogenen Expositionsermittlung“ - (Verteilungsbasierte Analyse gesundheitlicher Auswirkungen von Umwelt-Stressoren, VegAS) [Google Scholar]
- 14.Wang H, Dwyer-Lindgren L, Lofgren KT, et al. Age-specific and sex-specific mortality in 187 countries, 1970-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2071–2094. doi: 10.1016/S0140-6736(12)61719-X. [DOI] [PubMed] [Google Scholar]
- 15.Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salomon JA, Wang H, Freeman MK, et al. Healthy life expectancy for 187 countries, 1990-2010: a systematic analysis for the Global Burden Disease Study 2010. Lancet. 2012;380:2144–2162. doi: 10.1016/S0140-6736(12)61690-0. [DOI] [PubMed] [Google Scholar]
- 17.Salomon JA, Vos T, Hogan DR, et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet. 2012;380:2129–2143. doi: 10.1016/S0140-6736(12)61680-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Murray CJL, Ezzati M, Flaxman AD, et al. GBD 2010: design, definitions, and metrics. Lancet. 2012;380:2063–2066. doi: 10.1016/S0140-6736(12)61899-6. [DOI] [PubMed] [Google Scholar]
- 19.Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Moran AE, Forouzanfar MH, Roth GA, et al. The Global Burden of Ischemic Heart Disease in 1990 and 2010: The Global Burden of Disease 2010 Study. Circulation. 2014;129:1493–1501. doi: 10.1161/CIRCULATIONAHA.113.004046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013;10 doi: 10.1371/journal.pmed.1001547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Murray CJL, Ezzati M, Flaxman AD, et al. Supplementary appendix to: Comprehensive Systematic Analysis of Global Epidemiology: Definitions, Methods, Simplification of DALYs, and Comparative Results from the Global Burden of Disease Study 2010. Lancet. 2012 [Google Scholar]
- 24.Murray CJL, Ezzati M, Flaxman AD, et al. Supplementary appendix to: GBD 2010: design, definitions, and metrics. Lancet. 2012;380:2063–2066. doi: 10.1016/S0140-6736(12)61899-6. [DOI] [PubMed] [Google Scholar]
- 25.Kurth BM, Lange C, Kamtsiuris P, Hölling H. Gesundheitsmonitoring am Robert Koch-Institut. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. 2009;52:557–570. doi: 10.1007/s00103-009-0843-3. [DOI] [PubMed] [Google Scholar]
- 26.Mathers CD. Health expectancies: an overview and critical appraisal. In: Murray CJL, Salomon JA, Mathers CD, Lopez AD, editors. Summary measures of population health: Concepts, ethics, measurement and applications. Geneva: World Health Orgnaization; 2002. pp. 177–204. [Google Scholar]
- 27.Institute for Health Metrics and Evaluation. www.healthdata.org/gbd/data-visualizations. Global Burden of Disease (GBD) Visualizations. (last accessed on 9 August 2013) [Google Scholar]
- 28.Institute for Health Metrics and Evaluation. http://ghdxhealtdata.org/ Global Health Data Exchange (GHDx) (last accessed on 20 May 2014) [Google Scholar]
- 29.Institute for Health Metrics and Evaluation. www.healthdata.org/record/global-burden-disease-study-2010-gbd-2010-healthy-life-expectancy-1990-2010. Global Burden of Disease Study 2010 Healthy Life Expectancy by Country 1990-2010 (updated 2/23/13) (last accessed on 20 May 2014) [Google Scholar]
- 30.Institute for Health Metrics and Evaluation. www.healthdata.org/data-visualization/gbd-arrow-diagram. GBD Arrow diagram. (last accessed on 24 July 2013) [Google Scholar]
- 31.Institute for Health Metrics and Evaluation. www.healthdata.org/data-visualization/gbd-compare. GBD Compare. (last accessed on 24 July 2013) [Google Scholar]
- 32.Institute for Health Metrics and Evaluation. www.healthdata.org/data-visualization/gbd-heatmap. GBD Heatmap. (last accessed on 24 July 2013) [Google Scholar]
- 33.Raspe H. Gesundheitsberichterstattung des Bundes 2012. Berlin: Robert Koch-Institut; 2012. Rückenschmerzen. [Google Scholar]
- 34.Statistisches Bundesamt. Wiesbaden: Statistisches Bundesamt. 2011. Todesursachen in Deutschland 2010. [Google Scholar]
- 35.Lozano R, Naghavi M, Foreman K, et al. Supplementary appendix to: Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:1–765. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Matthews FE, Arthur A, Barnes LE, et al. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II. Lancet; 382. :1405–1412. doi: 10.1016/S0140-6736(13)61570-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement. 2013;9:63–75e2. doi: 10.1016/j.jalz.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 38.Nord E. Disability weights in the Global Burden of Disease 2010: Unclear meaning and overstatement of international agreement. Health Policy. 2013;111:99–104. doi: 10.1016/j.healthpol.2013.03.019. [DOI] [PubMed] [Google Scholar]
- 39.Taylor H, Jonas J, Keeffe J, Leasher J, Naidoo K, Pesudovs K, et al. Disability weights for vision disorders in the Global Burden of Disease Study. Lancet. 2012;381:23–24. doi: 10.1016/S0140-6736(12)62081-9. [DOI] [PubMed] [Google Scholar]
- 40.Ahmad OB, Boschi-pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. GPE Discussion Paper Series: No31 EIP/GPE/EBD. Geneva: World Health Organization; 2001. Age standradization of rates: A new WHO standard. [Google Scholar]