

Abstract
Specimen retrieval bags have long been used in laparoscopic gynecologic surgery for contained removal of adnexal cysts and masses. More recently, the concerns regarding spread of malignant cells during mechanical morcellation of myoma have led to an additional use of specimen retrieval bags for contained "in-bag" morcellation. This review will discuss the indications for use retrieval bags in gynecologic endoscopy, and describe the different specimen bags available to date.
Keywords: Laparoscopy, Specimen retrieval bag, Ovarian cyst, Morcellation
Review
Laparoscopic specimen retrieval bags have been used in minimally invasive gynecologic surgeries for many years. Originally, retrieval bags were used to remove adnexal cysts and masses through the small laparoscopic incisions while avoiding spillage of their content in the abdominal cavity. In those cases, the adnexa (in cases of adnexa removal) or the cyst (in cases of cystectomy) are placed within the specimen retrieval bag introduced into the pelvic, and the fluid is drained and suctioned in a contained manner. This practice was advocated due to concerns regarding spillage of a malignant cyst, which may be associated with dissemination of malignancy and upstaging of the disease [1]. In addition, intra-abdominal spillage of benign cysts such as benign cystic teratoma and mucinous cystadenoma may also be hazardous, and in rare cases has been associated with chemical peritonitis [2, 3].
More recently, an additional use for specimen retrieval bags in gynecology has been suggested in view of the FDA warning regarding use of mechanical power morcellators for removal of myoma and myomatous uteri [4]. This warning stems from the debate on the safety of using morcellators for the laparoscopic extraction of myoma due to the risk of inadvertent spread of unsuspected leiomyosarcoma resulting in cancer spread and worsened prognosis. This risk has been estimated from about 1/350 to 1/1000 cases. In order to decrease risk of spread of unsuspected leiomyosarcoma during morcellation, the option of placing the specimen retrieval bag in the abdominal cavity and performing the morcellation within the bag has been suggested. This practice would require the use of large specimen bags and adaptation of the morcellation technique [5].
Currently marketed specimen retrieval bags differ in their size (i.e., diameter of the bag) and in the technique employed to open and deploy the bag. The most commonly used specimen bags in gynecology range from 10 to 15 cm in diameter, and allow for easy removal of most adnexal masses. The 10 cm bags usually require a 10 mm laparoscopic port for introduction into the abdomen, which may be placed in the umbilicus or in the lower abdomen. The advantage of using a 10 cm umbilical port for introduction of the bag instead of a lower abdominal port is that the former usually does not require fascial closure. The 15 cm specimen bag usually requires a 12 mm port for introduction into the pelvic, necessitating closure of the fascia layer to avoid port-site hernia.
Specimen retrieval bags also differ in their opening technique. Some specimen bags have the ability to open automatically after introduction into the abdomen, while others require manual opening by two graspers holding the bag edges. The bags with automatic opening are usually easier to use, but often more expensive than the bags with manual opening. Figures 1, 2 show examples of a manually opening bag (Endobag, manufactured by Covidien, Mansfield, MA, USA) and an automatically opening bag (Endocatch, manufactured by Covidien, Mansfield, MA, USA), respectively. All bags are manufactured for single use. We have found that the specimen bag with a 10-cm diameter and manual opening is suitable for most adnexal surgeries, obviating the need to use the more expensive bags with automatic opening (Fig. 3). Some authors have described the use of “home-made” specimen bags, such as a surgical glove or a zipper storage bag, which are cheaper than the manufactured bags [6, 7]. The author has not used any of the “home-made” bags and therefore cannot recommend them.
Fig. 1.

Specimen bag with manual opening
Fig. 2.

Specimen bag with automatic opening
Fig. 3.
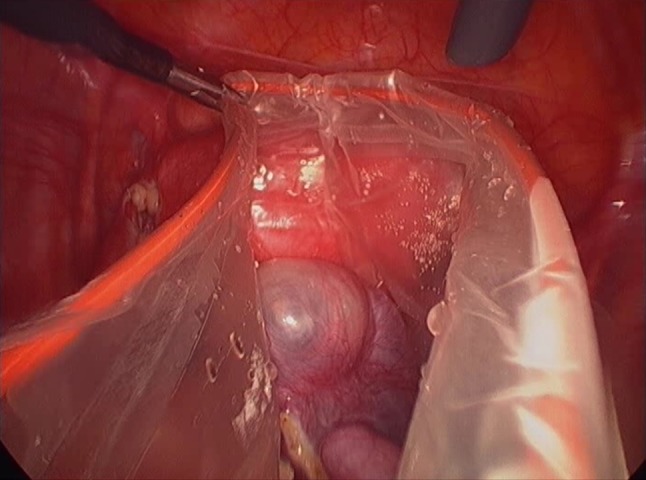
Specimen bag with manual opening deployed in the abdomen, containing two fallopian tubes in a patient with bilateral hydrosalpinges
As mentioned, specimen retrieval bags will likely be increasingly used to contain and prevent spread during myoma or uterine morcellation [8]. In order to perform morcellation in a bag, a large specimen bag is placed in the abdomen, ideally with its edges exteriorized to the abdominal wall and CO2 pneumoperitoneum created inside the bag. For this purpose, large bags are required, such as bowel isolation bags (typically measuring 50 × 50 cm). After the specimen is placed in the bag, the morcellation can be performed using a single port or a multiport approach. This technique requires a learning curve to allow for safe morcellation. As yet, limited clinical data are available on the outcomes and safety of “contained” morcellation. However, an in vitro study performed on box trainers did show lack of tissue dissemination using the contained morcellation technique [9]. Further discussions and statements issued by the national endoscopic societies and the local authorities regulating the use of medical devices will determine whether “contained” or “in-bag” morcellation will become the norm for laparoscopic retrieval of myoma.
Acknowledgments
Conflict of interest
No conflict of interest to disclose.
Noam Smorgick, MD Msc
is a senior faculty in the Gynecologic Endoscopy unit, Department of Obstetrics and Gynecology, Assaf Harofe Medical Center, Israel. She completed her MD degree (2003) at Hadassah school of Medicine, Hebrew University, Jerusalem, and was certified in Obstetrics and Gynecology in 2009. She then proceeded to complete a fellowship in Minimally Invasive Gynecologic Surgery (2011) and a fellowship in Pediatric and Adolescent Gynecology (2012) at the University of Michigan in Ann Arbor, Michigan, USA. She was recently elected as a committee member of the Israeli Society of Gynecological Endoscopy (ISGE), where she is responsible for outlining the ISGE position on endoscopic education for residents and practicing physicians. Her research interests include endometriosis and pelvic pain, robotic surgery, hysteroscopic surgery, and gynecologic ultrasound. She has authored more than 30 scientific publications in peer-reviewed journals. She currently serves as the secretary for the 11th AAGL International Congress (in partnership with the ISGE), to be held in Jerusalem in June 2015
References
- 1.Mayer C, Miller DM, Ehlen TG. Peritoneal implantation of squamous cell carcinoma following rupture of a dermoid cyst during laparoscopic removal. Gynecol Oncol. 2002;84:180–183. doi: 10.1006/gyno.2001.6484. [DOI] [PubMed] [Google Scholar]
- 2.Kondo W, Bourdel N, Cotte B, et al. Does prevention of intraperitoneal spillage when removing a dermoid cyst prevent granulomatous peritonitis? BJOG. 2010;117:1027–1030. doi: 10.1111/j.1471-0528.2010.02580.x. [DOI] [PubMed] [Google Scholar]
- 3.Ben-Ami I, Smorgick N, Tovbin J, et al. Does intraoperative spillage of benign ovarian mucinous cystadenoma increase its recurrence rate? Am J Obstet Gynecol. 2010;202:142-e1. doi: 10.1016/j.ajog.2009.10.854. [DOI] [PubMed] [Google Scholar]
- 4.http://www.fda.gov/medicaldevices/safety/alertsandnotices/ucm393576.htm.
- 5.Einarsson JI, Cohen SL, Fuchs N, et al. In-Bag Morcellation (IBM). J Minim Invasive Gynecol. 2014 [Epub ahead of print]. [DOI] [PubMed]
- 6.Yao CC, Wong HH, Yang CC, et al. Liberal use of a bag made from a surgical glove during laparoscopic surgery for specimens retrieval. Surg Laparosc Endosc Percutan Tech. 2000;10:261–263. [PubMed] [Google Scholar]
- 7.Yuen PM, Rogers MS. Laparoscopic removal of ovarian cysts using a zipper storage bag. Acta Obstet Gynecol Scand. 1994;73:829–831. doi: 10.3109/00016349409072514. [DOI] [PubMed] [Google Scholar]
- 8.Frishman GN. Should we bag tissue morcellation? Looking backwards and forwards. J Minim Invasive Gynecol. 2014 [Epub ahead of print]. [DOI] [PubMed]
- 9.Cohen SL, Greenberg JA, Wang KC, et al. Risk of leakage and tissue dissemination with various contained tissue extraction (CTE) techniques: an in vitro pilot study. J Minim Invasive Gynecol. 2014 [Epub ahead of print]. [DOI] [PubMed]