

Summary
Background
Intrasphenoidal encephalocele (ISE) is a rare clinical entity. The incidence of congenital encephalocele is very low. Accurate diagnosis and surgical approach is of critical value.
Case Reports
We present a case of intrasphenoidal encephalocele in a 40-year-old man. He complained of cerebrospinal fluid (CSF) rhinorrhea and recurrent meningitis. In images of computed tomography (CT) and magnetic resonance imaging (MRI), intrasphenoidal encephalocele herniating through a defect of the left lateral sphenoid sinus wall was determined. Incisional biopsies were taken by endoscopic transnasal approach and histopathological examination revealed an encephalocele. In the differential diagnosis, ISE can be taken for inflammatory or malignant sinusoidal soft tissue masses. ISE is differentiated from other entities by demonstrating continuity with normal brain tissue.
Conclusions
MRI clearly demonstrates that the herniating soft tissue is isointense with brain and continuous with brain tissue via the sphenoid sinus, thereby the treatment decision-making process is very important.
MeSH Keywords: Encephalocele, Magnetic Resonance Imaging, Multidetector Computed Tomography
Background
A combination of recurrent meningitis with spontaneous cerebro-spinal (CSF) rhinorrhea and intrasphenoidal encephalocele without obvious causes such as trauma or tumour is an extremely rare case [1]. The sphenoid bone develops from the ossification of several unconnected cartilaginous precursors; presphenoid and postsphenoid/basisphenoid centers (body of the sphenoid bone), orbitosphenoids (lesser wings), and alisphenoids (greater wings). Union of those ossified components results in formation of the sphenoid bone [2]. If the posterior part of the bony fusion of the greater wings with the bone’s body is incomplete, a canal forms at the involved area and it is called lateral craniopharyngeal canal. This canal was described by Sternberg in 1888. It is a weak area of the skull base, which may result in development of a temporal lobe encephalocele protruding into the lateral recess of the sphenoid sinus [3].
We reported on a case of intrasphenoidal encephalocele of the temporal lobe through the defect of the lateral wall of the sphenoid sinus. To the best of our knowledge, 63 cases were reported on in English literature [4].
Case Report
We reported on a 40-year-old man with complaints of headache and rhinorrhea, and a history of meningitis three times in the last 4 years, as well as no history of head trauma. His rhinorea was present for the last 6 months, as he stated.
Otolaryngologic examination was normal except for rhinorrhea. Hemogram was normal. In order to determine the etiology of CSF rhinorrhea, paranasal sinus CT was obtained and a bone defect in the lower part of the lateral wall of the left sphenoid sinus was determined. Moreover, polypoid mass with the same density as the brain tissue beside the defect was seen in the left sphenoid sinus (Figure 1). What is more, bilateral, apparent petrous apex pneumatization was noticed. In order to identify the structure of the polypoid mass in the left sphenoid sinus, brain magnetic resonance imaging (MRI) with contrasting agent was obtained. In brain MRI, intrasphenoidal encephalocele was seen (Figure 2). With those findings, the patient underwent transnasal endoscopic surgery. Incisional biopsy was taken from the polypoid mass in the sphenoid sinus (Figure 3). The histological examination of the specimens taken from the sphenoid sinus revealed glial tissue in fibrovascular connective tissue fragments of mucosa coated by respiratory-type epithelium (Figure 4A). Immunohistochemical stains for glial fibrillary acidic protein (GFAP) and S-100 confirmed the diagnosis (Figure 4B).
Figure 1.
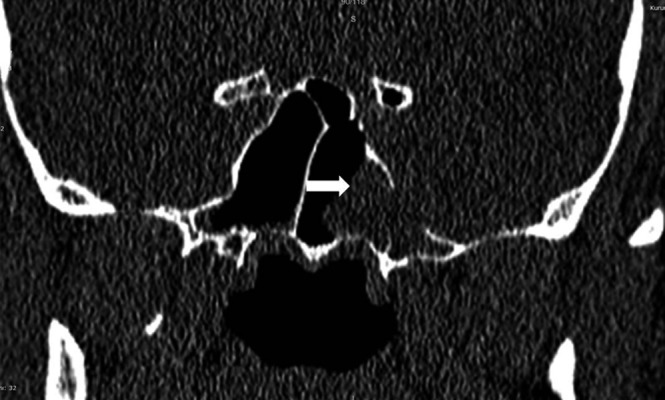
Coronal CT scan; sphenoid sinus in mid-level slices. Bone defect is noticed in the inferior third of the lateral wall of the left sphenoid sinus, and soft tissue with the same density as the brain tissue can be noticed beside the defect in the left sphenoid sinus.
Figure 2.
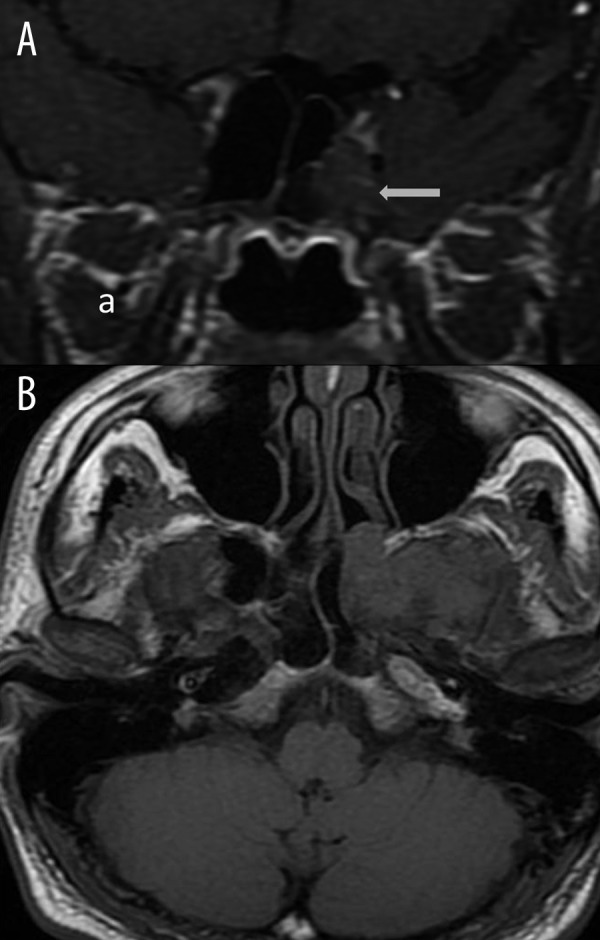
Contrast-enhanced T1W coronal (A) and axial (B) images: herniation of the temporal lobe into the sphenoid sinus is noticed (white arrows).
Figure 3.
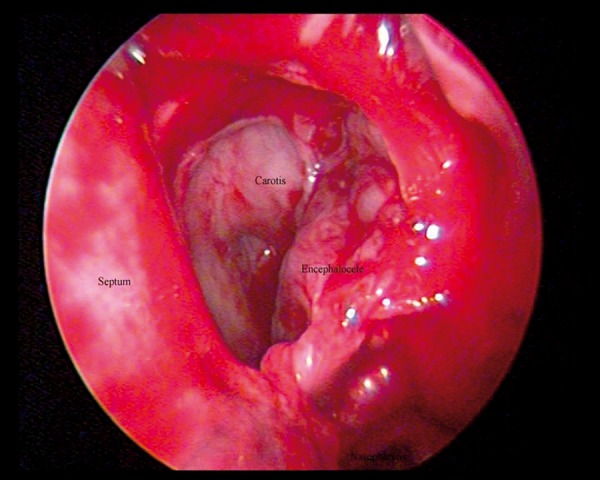
Endoscopic image shows left intraspheniodal encephalocele via transsphenoidal approach. Posterior part of the middle turbinate, posterior etmoidal cells and anterior wall of sphenoid sinus were removed.
Figure 4.
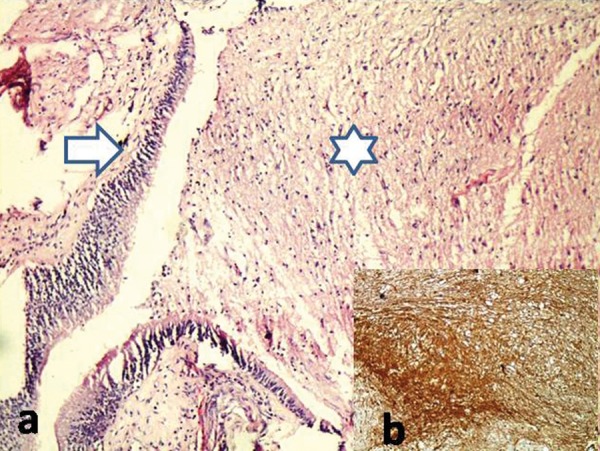
(A) There is a mixture of mature astrocytes and glial fibers (star) in fibrovascular connective tissue underlying respiratory epithelium (arrow) ×10 H&E. (B) GFAP-positive glial tissue ×200 IHC.
Discussion
Intrasphenoidal encephalocele (ISE) is a rare clinical condition. The incidence of congenital encephalocele is approximately 1 in 3000–5000 live birth [5]. ISE has an estimated incidence of 1 in 700,000 live birth [6]. A small occult congenital dysplasia in the form of defects or clefts in the base of the skull in the middle cranial fossa is suggested in the etiology of ISE. These structures constituting a weak area, under the pressure of the CSF may favor the creation of meningoceles or encephaloceles which finally become clinically apparent as spontaneous CSF rhinorrhea [7]. Incomplete posterior portion of the bony fusion in the sphenoid sinus creates a lateral craniopharyngeal canal (Sternberg’s canal). Sternberg’s canal is attributed as a possible site of origin of congenital encephalocele. Sphenoidal defects at fusion planes are more likely to be congenital than acquired [3].
Intracranial hypertension, by means of arachnoid pits in the lateral recess of the sphenoid sinus, is the major cause of acquired spontaneous CSF leaks and lateral intrasphenoidal encephaloceles [8]. Intrasphenoidal encephaloceles that have an intact dura and no CSF leak are generally reported during imaging studies for other causes [9].
The CSF volume is generally not affected because of intermittent drainage. Recurrent menengitis may also occur due to CSF drainage. Although there were both rhinorrhea and recurrent meningitis in the presented case, there was no history of trauma or tumour. We suggested that the bone defect in the lateral wall of the sphenoid sinus could be Sternberg’s canal.
In radiological imaging of encephalocele, CT, a non-invasive technique, shows bone structures in details and is more precise in detecting the defect sites in the skull base. Bone defect in the lateral wall of the left sphenoid sinus and soft tissue beside the defect and with the same density as the brain tissue were noticed in CT images of the presented case. In the differential diagnosis of soft tissue of that kind, inflammatory and tumoral lesions originating from the sphenoid sinus and cerebral tissue should be considered initially. Due to the fact that MRI is more accurate in visualizing soft tissues in detail, it should be performed. In the presented case, continuity of the cerebral tissue in the left sphenoid sinus was noticed in MRI and it was regarded as ISE (Figure 2A, 2B). Biopsy was carried out by transnasal endoscopic approach and soft tissue sample was subjected to histopathological examination. The differential diagnosis of ISE includes nasal teratoma, glial heterotopia and also a true glioma. ISE should be distinguish from other developmental anomalies and cystic teratomas based on characteristic clinical and radiological findings [10].
Because a persistent CSF leak may lead to meningitis or brain abscess, it is potentially lethal. Therefore, intrasphenoidal encephalocele should be repaired by surgical intervention. We used transnasal endoscopic approach in the presented case. After pushing the brain tissue toward the endocranium, temporal fascia and a free muscle graft were inserted into the defect of the lateral wall of the left sphenoid sinus and then fixed with fibrin glue.
Conclusions
Intrasphenoidal encephalocele often associated with a persistent Sternberg’s canal is a rare entity. Our patient presented with recurrent meningitis and CSF rhinorrhea. Malignancy, inflammatory changes and encephalocele are taken into account in the differential diagnosis of bone defect seen in CT. MRI examination shows cerebral tissue that extends into the sphenoid sinus. MR examination is extremely important in diagnosing intrasphenoidal encephalocele. Knowing that the soft tissue within the sphenoid sinus is encephalocele, allows us to change the therapeutic approach,
Footnotes
Conflicts of interest
The authors declared no conflicts of interest.
References
- 1.Daniilidis J, Vlachtsis K, Ferekidis E, Dimitriadis A. Intrasphenoidal encephalocele and spontaneous CSF rhinorrhoea. Rhinology. 1999;37(4):186–89. [PubMed] [Google Scholar]
- 2.Schick B, Brors D, Prescher A. Sternberg’s canal – cause of congenital sphenoidal meningocele. Eur Arch Otorhinolaryngol. 2000;257(8):430–32. doi: 10.1007/s004050000235. [DOI] [PubMed] [Google Scholar]
- 3.Arai A, Mizukawa K, Nishihara M, et al. Spontaneous cerebrospinal fluid rhinorrhea associated with a far lateral temporal encephalocele – case report. Neurol Med Chir (Tokyo) 2010;50(3):243–45. doi: 10.2176/nmc.50.243. [DOI] [PubMed] [Google Scholar]
- 4.Sanjari R, Mortazavi SA, Amiri RS, et al. Intrasphenoidal Meningo-encephalocele: Report of two rare cases and review of literature. Surg Neurol Int. 2013;4:5. doi: 10.4103/2152-7806.106260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Spacca B, Amasio ME, Giordano F, et al. Surgical management of congenital median perisellar transsphenoidal encephaloceles with an extracranial approach: a series of 6 cases. Neurosurgery. 2009;65(6):1140–45. doi: 10.1227/01.NEU.0000351780.23357.F5. discussion 1145–46. [DOI] [PubMed] [Google Scholar]
- 6.Kahyaoglu O, Cavusoglu H, Musluman AM, et al. Transsellar transsphenoidal rhino-oral encephalocele. Turk Neurosurg. 2007;17(4):264–68. [PubMed] [Google Scholar]
- 7.Bernstein JM, Roland JT, Persky MS. Sphenoid cranial base defects in siblings presenting with cerebrospinal fluid leak. Skull Base Surg. 1997;7(4):193–97. doi: 10.1055/s-2008-1058595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baranano CF, Cure J, Palmer JN, Woodworth BA. Sternberg’s canal: fact or fiction? Am J Rhinol Allergy. 2009;23(2):167–71. doi: 10.2500/ajra.2009.23.3290. [DOI] [PubMed] [Google Scholar]
- 9.Lai SY, Kennedy DW, Bolger WE. Sphenoid encephaloceles: disease management and identification of lesions within the lateral recess of the sphenoid sinus. Laryngoscope. 2002;112(10):1800–5. doi: 10.1097/00005537-200210000-00018. [DOI] [PubMed] [Google Scholar]
- 10.Douglas RG. Diagnostic surgical pathology of the head and neck. 2009. [Google Scholar]