

Abstract
Purpose
To evaluate the incidence, clinicopathological characteristics, treatment outcomes, prognostic factors, and survival of gastric cancer patients with bone metastases.
Materials and Methods
Of 4,617 gastric cancer patients who were treated between 2001 and 2013, 176 patients with bone metastases were analyzed.
Results
The incidence of bone metastasis was 3.8%. The most common histopathological subtype was adenocarcinoma (79%) with poor differentiation (60.8%). The median interval from the diagnosis to bone metastasis was 11 months. The median survival time after bone metastasis was 5.4 months. Factors that were associated with longer median survival times included the following: isolated bone metastasis (P=0.004), well-differentiated tumors (P=0.002), palliative chemotherapy (P=0.003), zoledronic acid treatment (P<0.001), no smoking history (P=0.007), and no metastatic gastric cancer at the time of diagnosis (P=0.01). On the other hand, high levels of lactate dehydrogenase (LDH) (hazard ratio [HR]: 1.86; P=0.015), carcinoembryonic antigen (CEA) (HR: 2.04; P=0.002), and carbohydrate antigen (CA) 19-9 (HR: 2.94; P<0.001) were associated with shorter survival times. In multivariate analysis, receiving zoledronic acid (P<0.001) and performance status (P=0.013) were independent prognostic factors.
Conclusions
Smoking history, poor performance status, poorly differentiated adenocarcinoma, and high levels of LDH, CEA, and CA 19-9 were shown to be poor prognostic factors, while receiving chemotherapy and zoledronic acid were associated with prolonged survival in gastric cancer patients with bone metastases.
Keywords: Stomach neoplasms, Bone metastasis, Prognosis, Survival, Zoledronic acid
Introduction
Gastric cancer (GC) is the fourth most common malignancy worldwide, with an estimated 989,600 newly diagnosed cases annually, and it is the second leading cause of cancer-related deaths, resulting in 738,000 deaths per year.1 According to GLOBOCAN 2012, age-standardized incidence rates for GC were 17.9 and 10.9, and mortality rates were 15.5 and 9.3 per 100,000 Turkish men and women, respectively.2
Most patients have metastatic or locally advanced disease at the time diagnosis, and the overall 5-year survival rate is 7% for stage IV GC. The systemic recurrence rate after curative resection is 60%, and the most common sites are the liver, peritoneum, and lungs.3,4 Although bone metastasis can be commonly observed in breast, prostate, and lung cancers, it is extremely rare in GC, and consequently, there is limited data available on the clinicopathological features, optimal treatment approaches, and prognostic factors for GC patients with bone metastasis in the existing literature. The majority of the studies investigating bone metastasis in GC originate from Japan and Korea where GC is endemic. The clinical course of bone metastasis from GC in different ethnic and regional populations is largely unknown. The reported frequency of bone metastasis in GC patients is 13.4% to 15.9% in autopsy series and increases up to 45.3% in bone metastasis screening studies, whereas it has been reported in only 0.9% to 10% of the GC patients in clinical practice.5,6,7,8,9,10,11,12,13 These findings suggest that asymptomatic bone metastasis is underestimated, and that the rate of bone metastasis in clinical cases may be much higher than is reported. The presence of bone metastasis in GC is a poor prognostic factor, and it is also associated with pain, pathological fractures, paralysis, hypercalcemia, and hematologic complications, all of which have a negative impact on the quality of life and treatment outcomes.
The purpose of this study was to investigate the frequency, demographics, and clinical and pathological features of GC patients with bone metastases. Furthermore, the prognostic factors, treatment outcomes, and survival in these patients were also evaluated.
Materials and Methods
1. Study population and data collection
A total of 4,617 patients who were diagnosed gastric adenocarcinoma between 2001 and 2013 were retrospectively reviewed. Of these, 176 GC patients with radiologically and/or pathologically confirmed bone metastasis were analyzed. Patients with nonadenocarcinoma histology, such as small cell, squamous cell types, as well as those with neuroendocrine carcinoma, gastric lymphoma, and those with other synchronous malignancies were excluded.
Sociodemographic data, such as the age at diagnosis, sex, smoking history, alcohol use, comorbid disease, and family history, as well as tumor characteristics, including histopathology, tumor localization, tumor size, TNM stage (according to 7th Union for International Cancer Control/American Joint Committee on Cancer classification), differentiation (good, moderate, poor, unknown) were obtained from the medical records of each patient. Furthermore, the number of total and metastatic lymph nodes, and the presence of lymphovascular invasion (LVI) and perineural invasion were also determined from patient records. Performance categories of the patients at the time of their bone metastasis diagnosis were determined by applying the Eastern Cooperative Oncology Group (ECOG) performance status scale. This study was approved by the ethics committee of Ankara Oncology Hospital.
2. Bone metastases definitions and diagnostic methods
Synchronous bone metastasis was defined as the development of bone metastasis simultaneously with the diagnosis of GC, and metachronous bone metastasis were considered to occur at any time during the follow-up period. Clinical symptoms, such as new onset, bone-related localized or generalized pain, paralysis, or limitation of movement; bone imaging findings; and laboratory parameters suggestive of bone metastases were further evaluated. In addition to plain radiography of the affected bone, Tc-99m whole body bone scintigraphy (WBBS), 18F fluorodeoxyglucose positron emission tomography (PET), and magnetic resonance imaging or computed tomography (CT) were performed. Patients with high uptake values underwent PET-CT and other imaging tests including WBBS for confirmation. Suspected involvement of bone metastasis was confirmed via other imaging methods, and those patients with suspected involvement in all radiologic studies were excluded from the analysis.
The following numerical values were recorded and obtained from tests performed at the time of the bone metastasis diagnosis: the interval between the date of GC diagnosis and the date of developing bone metastasis (months), the number and the localization of bone metastases, coexistence of bone and non-bone metastasis, and serum levels of hemoglobin, hematocrit, alkaline phosphatase (ALP), lactate dehydrogenase (LDH), carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA 19-9), and calcium.
3. Treatments and survival
The treatment modalities included surgery (curative/palliative), radiotherapy (adjuvant/palliative), chemotherapy (adjuvant/palliative), and bisphosphonates administration (zoledronic acid). Detailed information about treatment initiation/termination dates was obtained from the patients' medical records. Zoledronic acid was administered to patients with normal renal clearance at a dose of 4 mg every 4 weeks via a 15-minute infusion. The most commonly used chemotherapy regimens after bone metastasis development included the following: docetaxel/cisplatin/5-fluorouracil [5-FU] (DCF), 5-FU/leucovorin/irinotecan (FOLFIRI), cisplatin/capecitabine (CX), 5-FU/leucovorin, cisplatin/5-FU/leucovorin, epirubicin/cisplatin/5-FU, and single agent capecitabine.
The primary endpoint was the overall survival (OS) after developing bone metastasis (OS-BM), which was considered as the time from the date of bone metastasis diagnosis to the date of GC death. Data on mortality were obtained from the hospitals' medical records and via linkage with their respective death registries. If death was not evident, patients were censored at their last follow-up.
4. Statistical analyses
Descriptive statistics were expressed as the mean±standard deviation or median (minimum-maximum) for continuous variables in conjunction with the number of subjects and percentage for categorical variables. The Pearson chi-square test and Student t-test were used to analyze frequencies and means, respectively, to compare the clinicopathological parameters among groups, whereas the Kaplan-Meier analysis with a log-rank test was used to determine cumulative survival curves. Univariate and multivariate Cox proportional hazards regression models with 95% confidence intervals (CI) for OS-BM were performed to evaluate the prognostic factors. To select the factors with an independent significant influence on outcomes, only those factors with clinical significance in univariate analyses were included, and multivariate analyses were carried out in a stepwise Cox regression with backward selection.
Statistical analyses were performed using SPSS software version 15.0 (SPSS Inc., Chicago, IL, USA). All statistical assessments were two-sided, and the significance levels were set at P<0.05.
Results
1. Patient and tumor characteristics
A total of 4,617 patients with GC were analyzed, and bone metastasis was observed in 3.8% of the patients (n=176). The frequency of bone metastasis was 3.5% in men and 4.5% in women, with the mean age of the entire cohort being 57.8±12.9 years (range, 18~81 years). The majority of the patients (77%) had non-cardia GC, and the most common localization was the corpus (27.8%). The most common histopathological subtype was adenocarcinoma (79%) with poor differentiation (60.8%). The most common sites of metastases (except bone) were the liver (42.3%), lungs (23.9%), and peritoneum (19.6%). The patient and tumor characteristics are shown in Table 1.
Table 1.
Patient and tumor characteristics
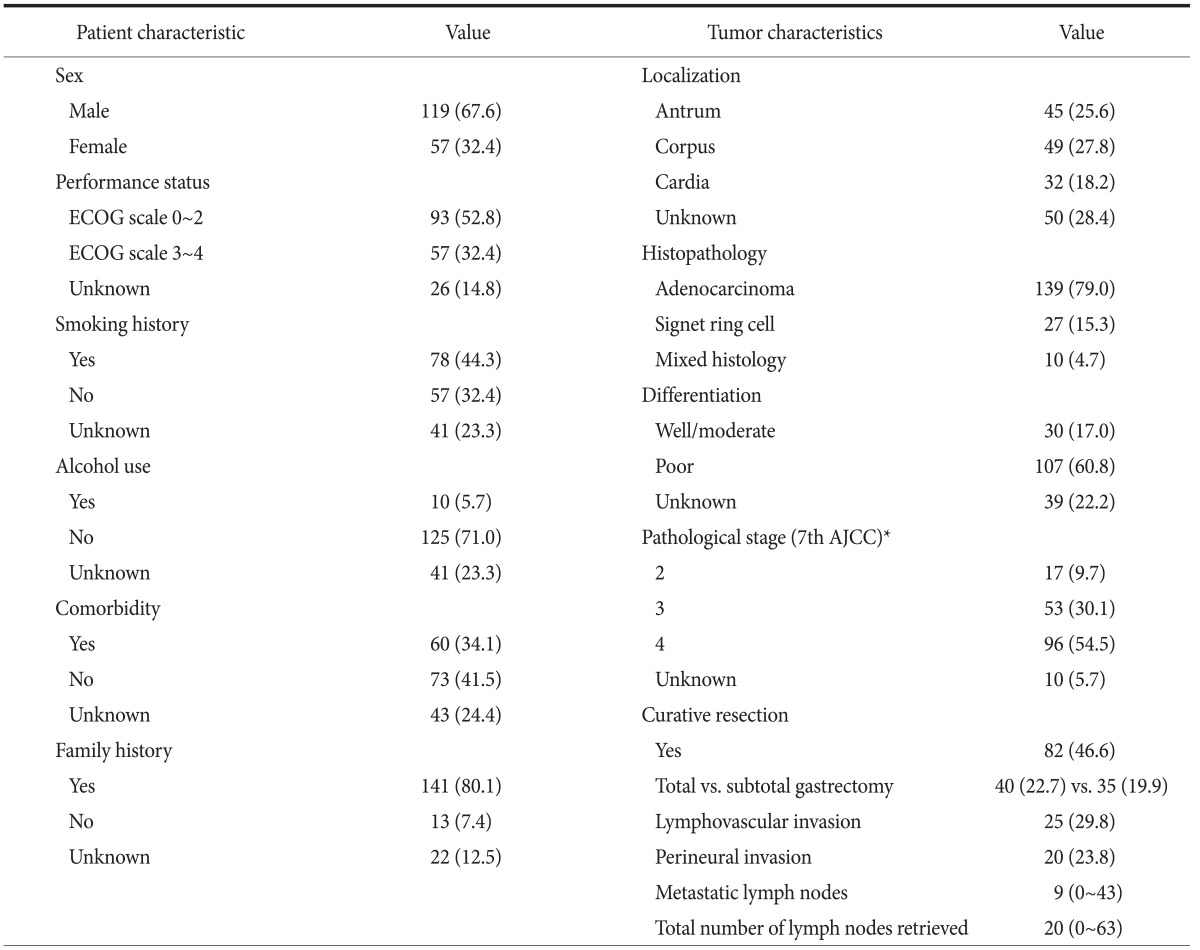
Values are presented as number (%) or median (range). ECOG = Eastern cooperative oncology group. *According to the 7th edition of the American Joint Committee on Cancer (AJCC) staging manual.
No significant associations were shown between bone metastasis patterns (synchronous vs. metachronous, isolated vs. co-existence of non-bone metastasis, or solitary vs. multiple) and demographic characteristics, such as age, sex, family history, tumor localization, differentiation, histopathology and ECOG performance status.
2. Patterns of skeletal metastasis
The median interval from the diagnosis of GC to skeletal metastasis was 11 months (14.2 months for resected GC and 8.2 months for inoperable GC patients; range, 2.5~121.1 months). In our cohort, 62.5% (n=110) of patients had metachronous lesions, 17.6% (n=31) had solitary lesions, and the remaining 28.4% (n=50) had isolated bone metastases. The diagnostic methods and bone metastasis characteristics are summarized in Table 2.
Table 2.
Bone metastasis characteristics
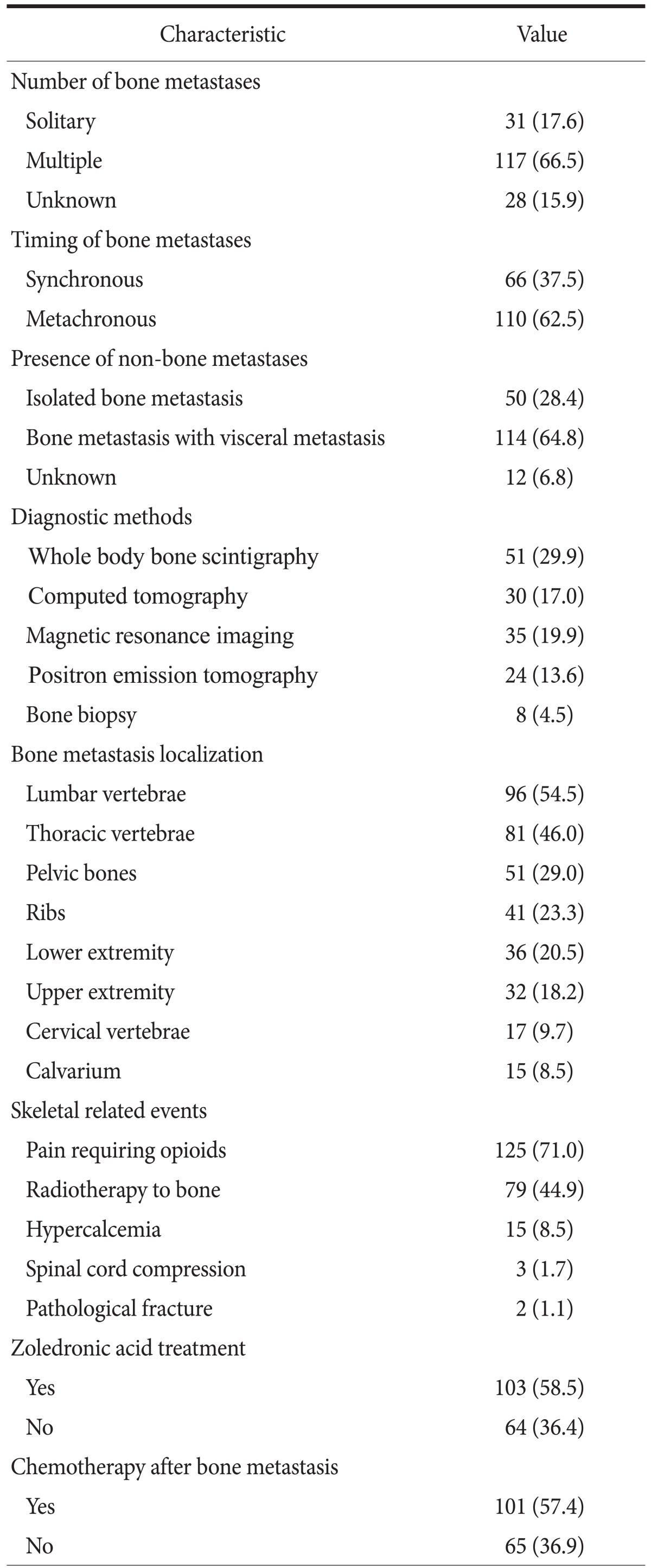
Values are presented as number (%).
Isolated bone metastases were observed more frequently in resected cases (82% vs. 18%; P<0.0001). However, no significant difference was seen in the number of bone metastases (P=0.53). We also showed that pelvic bone metastasis was significantly less common in patients who underwent operations with a curative intent (25.8% vs. 74.2%; P=0.004).
Anemia was observed in 46.6% of the patients, with concomitant bone marrow infiltration in only 7 patients (3.9%). Elevated levels of serum LDH, ALP, and CEA at the time of bone metastasis diagnosis were found in 40.0%, 31.3%, and 31.8% of the patients, respectively. Skeletal-related events (SREs), such as pain, hypercalcemia, and pathologic fractures, were observed in 75% (n=132) of the patients (Table 2).
There were no significant associations between the patterns of bone metastasis (isolated vs. co-existence of non-bone metastasis) and anemia, and hypercalcemia and serum levels of ALP. On the other hand, higher levels of LDH (75.4% vs. 55.2%; P=0.048), CEA (62.3% vs. 33.3%; P=0.006), and CA 19-9 (50.7% vs. 28.1%; P=0.033) were detected in patients who had both bone and concomitant non-bone metastases. Serum LDH levels were also higher in patients with synchronous bone metastasis than in the patients with metachronous bone metastasis (82.9% vs. 59.7%; P=0.013).
3. Treatments and survival
Eighty-two patients underwent curative resection for GC (46.6%). Palliative chemotherapy was administered to 101 patients (57.4%), while 18 patients with synchronous bone metastases and 52 patients with metachronous bone metastases could not receive chemotherapy owing to poor performance status, old age, or comorbidity, or because they refused chemotherapy, and 39.8% of patients only received the best supportive care.
The patients received a median of 5 (1~12) and 3 (1~8) cycles of chemotherapy in the first- and second-line of treatment, respectively. Of 101 patients, 58.9% received first-line palliative DCF, with a response rate of 36%. The other commonly administered chemotherapy regimen in the first-line palliative setting was CX (21.4%), with a response rate of 33.3%. Overall, 37 patients received second-line chemotherapy, and the most commonly used regimen was FOLFIRI. Although the response rates were high with the FOLFIRI regimen (53.4%), one-third of the patients had not completed therapy owing to intolerance.
Palliative radiotherapy was administered to 79 patients (44.9%), and zoledronic acid was administered to 103 patients (58.5%). Zoledronic acid treatment was given to patients with a good performance status (72% vs. 28%; P=0.004) who were also receiving chemotherapy (70.5% vs. 29.5%; P=0.016). Only 36.7% of the patients receiving the best supportive care were treated with zoledronic acid. Those patients receiving zoledronic acid had higher levels of LDH, CEA, and CA 19-9 (P=0.01, P=0.07, and P=0.003, respectively).
In the overall study population, the 2-year OS rates were 31%, 21%, and 3% for patients with stage II, III, and IV GC, respectively (Plog-rank<0.001). The median OS and OS-BM were 13.8 months (95% CI, 11.5~16.1) and 5.4 months (95% CI, 4.0~6.9), respectively (Fig. 1). The median follow-up time after bone metastasis was 27.5 months (range, 1~56.5 months). The patients with isolated bone metastases had longer OS (27.1 vs. 11.9 months; Plog-rank<0.001) and OS-BM (20.4 vs. 8.5 months; Plog-rank=0.004) than the patients who had both bone and concomitant non-bone metastases (Fig. 2). No significant differences were found in OS and OS-BM between the patients with solitary and multiple bone metastases (18.2 vs. 13.2 months; Plog-rank=0.266, and 5.9 vs. 5.4 months; Plog-rank=0.153, respectively). The median OS-BM was also similar between the patients with synchronous and metachronous bone metastases (4.3 vs. 5.3 months; Plog-rank=0.124).
Fig. 1.

Overall survival of patients after developing bone metastasis. OS-BM = overall survival after developing bone metastasis.
Fig. 2.

Overall survival of patients with and without isolated bone metastasis. OS-BM = overall survival after developing bone metastasis.
The median OS-BM was longer in patients who had no smoking history (8.7 vs. 4.6 months; Plog-rank=0.007) and no metastatic GC at the time of diagnosis (6.7 vs. 4.3 months; Plog-rank=0.01). In addition, patients with a good ECOG performance status had a longer OS-BM (7.4 vs. 3.1 months; Plog-rank<0.001) compared to patients with a poor performance status (Fig. 3). The median OS-BM was 19.3 months in patients with well-differentiated tumors, and only 4 months for patients with poorly-differentiated GC (Plog-rank=0.002). The patients with elevated levels of serum LDH (4.3 vs. 9 months; Plog-rank=0.013), CEA (4.2 vs. 8.4 months; Plog-rank=0.002), and CA 19-9 (3.1 vs. 10 months; Plog-rank<0.001) had significantly shorter OS-BM compared to patients with normal levels of LDH, CEA, and CA 19-9, respectively. Sex (Plog-rank=0.092), presence of comorbidity (Plog-rank=0.107), number of bone metastases (Plog-rank=0.153), hypercalcemia (Plog-rank=0.185), anemia (Plog-rank=0.097), and serum ALP levels (Plog-rank=0.358) all did not seem to have significant effects on OS-BM.
Fig. 3.

Overall survival of patients after developing bone metastasis, according to the performance status. OS-BM = overall survival after developing bone metastasis, ECOG = Eastern Cooperative Oncology Group scale.
The median OS-BM was 7 months (95% CI, 4.6~9.4) for patients who received palliative chemotherapy versus 3.1 months (95% CI, 2.1~4.1) for those receiving only the best supportive care (Plog-rank=0.003). In addition, patients treated with zoledronic acid (10.1 vs. 1.8 months; Plog-rank<0.001) showed significantly longer survival times (OS-BM). The survival curves are shown in Fig. 4,5,6.
Fig. 4.

Overall survival of patients receiving chemotherapy after developing bone metastasis. OS-BM = overall survival after developing bone metastasis.
Fig. 5.

Overall survival of patients receiving zoledronic acid after developing bone metastasis. OS-BM = overall survival after developing bone metastasis.
Fig. 6.

Overall survival of patients receiving zoledronic acid after developing bone metastasis, according to the TNM stage. OS-BM = overall survival after developing bone metastasis.
In univariate analysis, high levels of LDH (hazard ratio [HR]: 1.86, 1.13~3.05; P=0.015), CEA (HR: 2.04, 1.29~3.23; P=0.002), and CA 19-9 (HR: 2.94, 1.86~4.64; P<0.001) were associated with shorter survival times after bone metastasis. The patients with poor ECOG performance status had an approximately 2-fold increased risk of mortality (HR: 1.93, 1.34~2.79; P<0.001). In contrast, the patients who received chemotherapy after bone metastasis had a decreased risk of mortality (HR: 0.59, 0.42~0.84; P=0.003). In multivariate analysis, receiving zoledronic acid treatment (P<0.001) and ECOG performance status (P=0.013) were independent prognostic factors for GC patients with bone metastases.
Discussion
In our study, of 4,617 patients diagnosed with GC, the frequency of bone metastasis was 3.8%. Although GC is most commonly known to spread to the peritoneum, liver, and lungs, the reported incidence of bone metastasis is 1% to 45% in the literature.7,8,9,10,11,12,13 Park et al.9 evaluated 8,633 Korean GC patients and described the clinicopathological features of 204 (2.4%) cases showing bone metastases. According to their study, the incidence of bone metastasis was only 0.9% after gastric resection and 11.2% in inoperable patients. In a multicenter Italian study, the authors reported an incidence of bone metastasis in 10% of GC patients.13 Ahn et al.10 reported that among 2,150 GC patients, 19 patients (0.9%) had bone metastases. Yoshikawa and Kitaoka12 also reported low rates of bone metastasis (1.2%) in 1,945 curatively resected GC cases. Nishidoi and Koga6 reported that the incidence of bone metastasis of GC was 13.4% among 246 autopsies and was higher than that observed among 2,242 resected cases (1.5%). In another autopsy study of 176 GC cases, Mori et al.5 found that 15.9% of the patients had lesions that had metastasized to bones, which was the third most common site of GC metastases. Two previous studies evaluated skeletal metastases with bone scintigraphy, and metastatic bone lesions were found in 25.0% to 45.3% of the patients with advanced GC.7,8 These reported incidences and prognoses of GC patients with bone metastases differ substantially between studies, which may be because of several factors such as ethnic or regional variations, bone metastasis definitions, time of evaluation, and/or the diagnostic methods.
In the present study, the median time to skeletal metastasis was 14.2 months in resected GC patients and 8.2 months in inoperable GC patients. Yoshikawa and Kitaoka12 reported that 87% of the patients developed bone metastasis within 2 years of gastric surgery. Nakanishi et al.14 reported a mean interval of 14 months between gastric surgery and the diagnosis of bone metastasis. Consistent with these findings, Park et al.9 found that the median time to skeletal metastasis was 16 months. On the basis of these previous data, the possibility of bone metastases should be considered during the follow-up of GC patients, even in the early period.
The most common histopathological subtype in our study was adenocarcinoma (79%) with poor differentiation (60.8%). Most of the previous studies showed relationships between poorly differentiated adenocarcinoma and the risk of bone metastasis in advanced GC patients.6,9,10,11,12,13,14,15 In our study, a significant survival benefit (19.3 vs. 4 months) was observed for patients with well-differentiated tumors. It has been suggested that the risk of bone metastasis is associated with lymph node involvement, large tumor size, the depth of the tumor, and the presence of LVI in some studies, whereas no association was reported in others.8,9,11,12,13,15 We found no significant associations between survival and the above variables.
Sudo et al.15 reported that metastatic bone lesions were predominantly seen in the lumbar-thoracic vertebra and in the ribs. Park at al.9 also showed that bone metastases of GC most commonly occurred in the spine and pelvis. In our study, the most common sites of metastases were in the lumbar vertebra (54.5%), thoracic vertebra (46%), and pelvis (29%), similar to previous reports.7,8,9,10,11,15 Only the multicenter Italian study indicated long bones as the most common site of bone metastasis (52%) followed by the hip and spine.13 The underlying pathophysiology of bone metastasis in GC is still controversial, and the suggested pathways include the paravertebral venous plexus, portal vein, lymphatic channels, thoracic duct and gastric mucosal capillaries;9,12,14,16,17,18 the paravertebral venous plexus might be the major route of bone metastasis in our cohort.
Skeletal metastatic lesions arising from GC usually occur as many lesions and are of the osteolytic type.7,8,9,10,11,12,13,14 We observed multiple bone metastases in 66.5% of patients and found no difference in OS-BM with regard to the number of bone metastases. Silvestris et al.13 also showed similar survival durations between multiple and solitary bone metastases; however, Park et al.9 found that the presence of multiple bone metastases was a poor prognostic factor (HR=2.59; P=0.002) in their study population. The majority of our patients had metachronous bone metastases (62.5%). The clinical, pathological features, and the median OS-BM were similar between the patients with synchronous and metachronous bone metastases, which is consistent with previous reports.9,10,13
Higher LDH, CEA, and CA 19-9 levels were detected in patients who had both bone and concomitant non-bone metastases, and they were poor prognostic factors in the present study. Moreover, ECOG performance status was found to be an independent prognostic factor. Sudo et al.15 identified elevated serum LDH levels in 47.7% of their study population. In comparison, our study detected elevated serum LDH levels in 40.3% of the patients, which was associated with synchronous bone metastasis and an increased mortality risk (HR: 1.86; P=0.015). An elevated serum ALP level was an important diagnostic factor for patients with bone metastases from GC, as reported in several previous studies; in our study, 31.3% of the patients were determined to have elevated serum ALP levels, which had no impact on survival.7,8,16,19 In GC patients, elevated serum levels of calcium, ALP, LDH, and tumor markers might indicate bone metastasis. Park et al.9 linked high CEA levels with the presence of multiple metastases, and both elevated CEA levels and a poor ECOG performance status were independent prognostic factors. They developed a simple prognostic model to facilitate the clinical decision-making process, and they reported a median OS of 43 days in patients with all three risk factors compared to a median OS of 219 days in patients with no risk factors. Although these factors may be helpful in predicting treatment outcomes, the therapeutic approach should be personalized for individual patients.
In our study, anemia was observed in 46.6% of the patients, and both bone and bone marrow involvement were detected in 7 patients (3.9%). Park et al.9 observed secondary bone marrow involvement in 4.9% of their patients, who all had significantly poorer survival when compared to those patients without bone marrow involvement (51 vs. 110 days, P<0.001). In bone metastasis from GC, the cancer cells may diffusely proliferate in the bone marrow, resulting in bone destruction and eventually leading to disseminated carcinomatosis.16
Pain, immobilization, pathological fractures, sudden paralysis and hematological disorders, such as hemolytic anemia and disseminated intravascular coagulation, are all associated with bone metastasis, which will lead to a negative impact on the patients' quality of life, performance status and further treatment. Early diagnosis and treatment are very important to prevent disease progression in these patients. When comparing rates of SREs, our data revealed a rate of 75% in our patients while the previous literature reported rates of 37% to 84%.9,10,13,19 In an observational study, the median time to the first SRE was 2 months and the median survival after SRE occurrence was 3 months.13 Pain is the most frequent form of SRE that is treated with non-steroidal anti-inflammatory drugs and opioid analgesics. Palliative radiotherapy is also used to control severe pain and to prevent fractures, which was reported as an effective strategy in these patients.10,12,13
Zoledronic acid, a bisphosphonate, inhibits osteoclast-mediated bone resorption and increases bone mineralization. It also has antitumor and anti-angiogenic effects, and it has been proven effective in preventing SREs in bone metastases of solid tumors.20 However, the data on the efficacy of bisphosphonates in bone metastatic GC are lacking in the literature. In a recent study, Silvestris et al.13 showed a significant extension of the time to the first SRE and an increase in the median survival time with zoledronic acid after the diagnosis of bone metastasis in GC patients. As a confirmatory finding, we also observed a significantly longer survival time (OS-BM) for patients treated with zoledronic acid (10.1 vs. 1.8 months; Plog-rank<0.001), indicating that zoledronic acid treatment (P<0.001) was an independent prognostic factor for these patients (P<0.001). These data may support the beneficial effects of zoledronic acid in GC patients with bone metastasis. On the other hand, zoledronic acid was prescribed selectively to the patients who received chemotherapy and who had a good performance status, which must be considered when evaluating these results.
A number of trials have provided evidence for the effect of systemic chemotherapy compared to best supportive care alone for patients with advanced GC. In a meta-analysis, a significant improvement in OS was shown in favor of chemotherapy (HR: 0.37; 95% CI, 0.24~0.55).21 We observed a significant impact of receiving palliative chemotherapy on survival (HR: 0.59; P=0.003) in our cohort. Ahn et al.10 reported an improvement in the clinical symptoms and survival time with chemotherapy in these patients. Although earlier studies showed no clear benefit of chemotherapy in GC patients with bone metastasis, with the development of chemotherapeutic agents such as taxanes and S-1, and targeted therapies such as trastuzumab have been recognized to be an effective management approach.12 Park et al.9 suggested that aggressive therapeutic approaches should be reserved for low-risk patients while conservative care is a more desirable option for high-risk patients. A number of various effective chemotherapy regimens have been described in cases of GC with bone metastases in the literature; however, no prospective randomized trials have been conducted.
Several studies have reported that the presence of bone metastasis in GC is associated with a poor prognosis. The median OS and OS-BM of the entire study population were 13.8 and 5.4 months, respectively. Moreover, the median OS-BM was significantly shorter in patients with a smoking history, metastatic GC at the time of diagnosis and a poor ECOG performance status. Nakanishi et al.14 found that the mean survival time after a diagnosis of skeletal metastasis was 60 days in their study, which included 48 GC patients. Ahn et al.10 reported that the mean survival time after the diagnosis of bone metastasis was 3.8±2.6 months and Sudo et al.15 found that the median survival time was 189 days. Similarly, the median OS-BM was found to be approximately 6 months in two recent studies.9,13 The survival results of our study are similar to those described in these previous studies.
One of the limitations of our study was that the majority of the bone metastases were not confirmed pathologically. Another limitation was that the impact of bone metastases on the function and quality of life could not be evaluated owing to the retrospective design of the study. Moreover, the current study did not quantify and compare the therapeutic effects of chemotherapy regimens because of the wide range of anti-cancer therapies utilized. Although univariate and multivariate analyses reached the statistical significance threshold (P<0.05), missing data could lead to some biases.
In conclusion, bone metastasis of GC is often in multiple locations, metachronous, coexisting with visceral metastasis, and most commonly in the lumbar-thoracic vertebrae and pelvis. While smoking history and high levels of LDH, CEA, and CA 19-9 are poor prognostic factors, treatment with chemotherapy is associated with longer survival. According to multivariate analysis, treatment with zoledronic acid and the performance status were found to be independent prognostic factors. Early diagnosis and treatment are crucial to prevent the development of severe morbidity in GC patients with bone metastasis.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.International Agency for Research on Cancer. Globocan 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 [Internet] Lyon: International Agency for Research on Cancer; [cited 2014 Jun 15]. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx?country=792. [Google Scholar]
- 3.Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, and the "different disease" hypothesis. Cancer. 2000;88:921–932. [PubMed] [Google Scholar]
- 4.Wanebo HJ, Kennedy BJ, Chmiel J, Steele G, Jr, Winchester D, Osteen R. Cancer of the stomach. A patient care study by the American College of Surgeons. Ann Surg. 1993;218:583–592. doi: 10.1097/00000658-199321850-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mori W, Adachi Y, Okabe H, Ohta K. An analysis of 755 autopsied cases of malignant tumors. A statistical study of their metastasis. Gan No Rinsho. 1963;9:351–374. [Google Scholar]
- 6.Nishidoi H, Koga S. Clinicopathological study of gastric cancer with bone metastasis. Gan To Kagaku Ryoho. 1987;14:1717–1722. [PubMed] [Google Scholar]
- 7.Choi CW, Lee DS, Chung JK, Lee MC, Kim NK, Choi KW, et al. Evaluation of bone metastases by Tc-99m MDP imaging in patients with stomach cancer. Clin Nucl Med. 1995;20:310–314. doi: 10.1097/00003072-199504000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Seto M, Tonami N, Koizumi K, Sui O, Hisada K. Bone metastasis in gastric cancer--clinical evaluation of bone scintigrams. Kaku Igaku. 1983;20:795–801. [PubMed] [Google Scholar]
- 9.Park HS, Rha SY, Kim HS, Hyung WJ, Park JS, Chung HC, et al. A prognostic model to predict clinical outcome in gastric cancer patients with bone metastasis. Oncology. 2011;80:142–150. doi: 10.1159/000328507. [DOI] [PubMed] [Google Scholar]
- 10.Ahn JB, Ha TK, Kwon SJ. Bone metastasis in gastric cancer patients. J Gastric Cancer. 2011;11:38–45. doi: 10.5230/jgc.2011.11.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Park JM, Song KY, O JH, Kim WC, Choi MG, Park CH. Bone recurrence after curative resection of gastric cancer. Gastric Cancer. 2013;16:362–369. doi: 10.1007/s10120-012-0193-y. [DOI] [PubMed] [Google Scholar]
- 12.Yoshikawa K, Kitaoka H. Bone metastasis of gastric cancer. Jpn J Surg. 1983;13:173–176. doi: 10.1007/BF02469472. [DOI] [PubMed] [Google Scholar]
- 13.Silvestris N, Pantano F, Ibrahim T, Gamucci T, De Vita F, Di Palma T, et al. Natural history of malignant bone disease in gastric cancer: final results of a multicenter bone metastasis survey. PLoS One. 2013;8:e74402. doi: 10.1371/journal.pone.0074402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nakanishi H, Araki N, Kuratsu S, Narahara H, Ishikawa O, Yoshikawa H. Skeletal metastasis in patients with gastric cancer. Clin Orthop Relat Res. 2004;(423):208–212. doi: 10.1097/01.blo.0000129159.65684.b3. [DOI] [PubMed] [Google Scholar]
- 15.Sudo H, Takagi Y, Katayanagi S, Hoshino S, Suda T, Hibi Y, et al. Bone metastasis of gastric cancer. Gan To Kagaku Ryoho. 2006;33:1058–1060. [PubMed] [Google Scholar]
- 16.Kobayashi M, Okabayashi T, Sano T, Araki K. Metastatic bone cancer as a recurrence of early gastric cancer -- characteristics and possible mechanisms. World J Gastroenterol. 2005;11:5587–5591. doi: 10.3748/wjg.v11.i36.5587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Batson OV. The function of the vertebral veins and their role in the spread of metastases. 1940. Clin Orthop Relat Res. 1995;(312):4–9. [PubMed] [Google Scholar]
- 18.Lehnert T, Erlandson RA, Decosse JJ. Lymph and blood capillaries of the human gastric mucosa. A morphologic basis for metastasis in early gastric carcinoma. Gastroenterology. 1985;89:939–950. doi: 10.1016/0016-5085(85)90192-1. [DOI] [PubMed] [Google Scholar]
- 19.Kılıçkap S, Tapan Ü, Yalçın Ş. Metastasis to bone from gastric cancer: a single centre experience. Cumhuriyet Med J. 2010;32:192–198. [Google Scholar]
- 20.Aapro M, Abrahamsson PA, Body JJ, Coleman RE, Colomer R, Costa L, et al. Guidance on the use of bisphosphonates in solid tumours: recommendations of an international expert panel. Ann Oncol. 2008;19:420–432. doi: 10.1093/annonc/mdm442. [DOI] [PubMed] [Google Scholar]
- 21.Wagner AD, Grothe W, Haerting J, Kleber G, Grothey A, Fleig WE. Chemotherapy in advanced gastric cancer: a systematic review and meta-analysis based on aggregate data. J Clin Oncol. 2006;24:2903–2909. doi: 10.1200/JCO.2005.05.0245. [DOI] [PubMed] [Google Scholar]