

Abstract
The cerebello-pontine angle lipomas causing trigeminal neuralgia or hemifacial spasm are rare. A lipoma causing glossopharyngel neuralgia is also very rare. A 46-year-old woman complained of 2-year history of severe right throat pain, with ipsilateral episodic otalgic pain. The throat pain was described as an episodic lancinating character confined to the throat. Computed tomography and magnetic resonance imaging revealed a suspicious offending posterior inferior cerebellar artery (PICA) compressing lower cranial nerves including glossopharyngeal nerve. At surgery, a soft, yellowish mass (2×3×3 mm in size) was found incorporating the lateral aspect of proximal portion of 9th and 10th cranial nerves. Only microvascular decompression of the offending PICA was performed. Additional procedure was not performed. Her severe lancinating pain remained unchanged, immediate postoperatively. The neuralgic pain disappeared over a period of several weeks. In this particular patient with a fatty neurovascular lump causing glossopharyngeal neuralgia, microvascular decompression of offending vessel alone was enough to control the neuralgic pain.
Keywords: Lipoma, Glossopharyngeal neuralgia
INTRODUCTION
Glossopharyngeal neuralgia (GPN) is a rare condition, occurring with a frequency of about 1% of that of trigeminal neuralgia6,7). Its reported incidence is approximately 0.8 per 100000 people. Vascular compression is a common and treatable cause.
The cerebellopontine angle (CPA) lipomas causing trigeminal neuralgia or hemifacial spasm are uncommon and a lipoma causing GPN is extremely rare. Because of the rare occurrence of these tumors of the CPA lipoma causing GPN, the experience in the therapeutic management is limited.
We report a rare case of GPN caused by a lipoma with a review of the literature.
CASE REPORT
A 46-year-old woman complained of 2-year history of severe right throat pain, and ipsilateral otalgic pain. The throat pain was described as an episodic lancinating character confined to the right side. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed a suspicious offending posterior inferior cerebellar artery (PICA) compressing lower cranial nerves including glossopharyngeal nerve (Fig. 1).
Fig. 1.

MRI finding shows a suspicious offending vessels visible at both in fast imaging employing steady-state acquisition (FIESTA) (A and B) and in time of flight (TOF) image (C and D). A small oval-shaped mass is observed as low signal intensity in TOF image (C and D). PICA : posterior inferior cerebellar artery.
Preoperatively, an electromyogram-motor nerve conduction velocity [EMG-MCV, Medelec Synergy (EMG/EP), YoungWoo-Meditec, Seoul, Korea] of facial nerve, and otolaryngologic evaluation were carried.
To detect vascular anatomy causing a neuralgic pain and to inspect relationships between offending vessels and causative nerve, MRI, magnetic resonance angiography (MRA) and computed tomographic angiography (CTA, Philips Biliance, Cleveland, OH, USA) were studied. MRI was performed on 1.5 T (Sigma EXCI-TE, General Electronics, Milwaukee, WI, USA) or 3.0-T scanners (Achieva, Philips, Eindhoven, The Netherland).
A retromastoid lateral suboccipital craniotomy was performed to visualize the root entry zone of glossopharyngeal, vagus and accessory nerves. A soft, yellowish mass (2×3×3 mm in size) was found incorporating the lateral aspect of proximal portion of 9th and 10th cranial nerves. Therefore, the proximal portion of 9th nerve was displaced medially. The distal portion of glossopharyngeal nerve was pushed laterally by pulsatory compression of PICA (Fig. 2). Microvascular decompression (MVD) of the offending PICA was performed. No additional procedure to remove the lipoma was carried out. Immediate postoperatively, her severe lancinating pain remained unchanged. However, the neuralgic pain intensity diminished gradually over a period of several weeks and disappeared. One year later, her pain developed intermittently, however its intensity is tolerable and well controlled with intermittent carbamazepine.
Fig. 2.
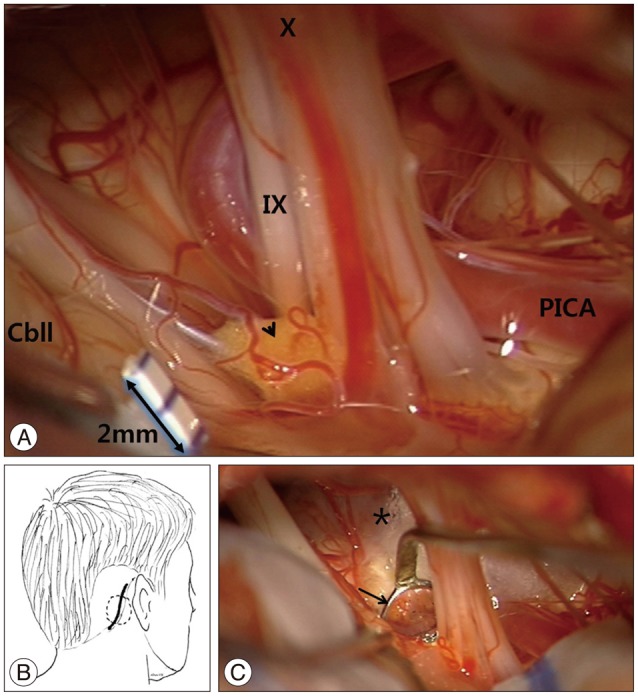
Surgical findings. A : Operative finding shows a soft, yellowish mass (2×3×3 mm in size, arrowhead) incorporating the lateral aspect of proximal portion of 9th and 10th cranial nerves. Additionally, the distal portion of 9th nerve was pushed laterally by pulsatory compression of PICA. B : Scalp incision and a portion of craniotomy was demonstrated. C : After decompression procedure, a glue coated teflon bulk (*) is visible fixing an offending PICA to the brain stem. Sufficient decompression of the root entry zone (REZ) is confirmed with a micromirror (arrow). PICA : posterior inferior cerebellar artery.
DISCUSSION
GPN is characterized by severe, unilateral lancinating and paroxysmal pain on tongue base, throat, and tonsil, triggered by swallowing, chewing, coughing, yawning, etc4,11,12). Treatment modalities for GPN include medications8), Gamma knife radiosurgery13,16), or MVD6,7). MVD of the GPN via lateral suboccipital infrafloccular approach is a good curative treatment modality for GPN7,10), despite its known low operative success rate.
Although lipomas are the most common form of soft tissue neoplasm, its intracranial form is exceedingly rare and most of them are found incidentally during neuroradiological study15) with an incidence of 0.08%, accounting for only 0.1% of all CPA masses14). A few papers were published regarding lipoma causing cranial rhizopathy1,2,3,15,17), including trigeminal neuralgia1) and hemifacial spasm2,3). By 1995, only up to 46 cases of CPA lipoma had been reported in the literature with 7 cases causative of trigeminal neuralgia17). The mechanism can be attributed to 5th nerve pushing against the blood vessel rather than the usual arterial cross-compression1). It was suggested that minimal excision of the lipoma or a partial rhizotomy was enough to relieve trigeminal neuralgia symptoms5).
The CPA lipomas tend to envelop cranial nerves and have attachments to the brain stem that treatment of these tumors should be conservative. Furthermore, as CPA lipoma resection is associated with a high risk of neurologic morbidity and lesion progression is unusual, conservative observation remain the default strategy in most patients9,15). And, limited surgery is indicated if the patients suffer from disabling neurological symptoms and signs1,3).
CONCLUSION
In this particular patients with a fatty neurovascular lump causing a glossopharygeal neuralgia, microvascular decompression of offending vessel alone was enough to control the neuralgic pain.
References
- 1.Alafaci C, Salpietro FM, Puglisi E, Tripodo E, Matalone D, Di Pietro G. Trigeminal pain caused by a cerebellopontine-angle lipoma. Case report and review of the literature. J Neurosurg Sci. 2001;45:110–113. [PubMed] [Google Scholar]
- 2.Barajas RF, Jr, Chi J, Guo L, Barbaro N. Microvascular decompression in hemifacial spasm resulting from a cerebellopontine angle lipoma : case report. Neurosurgery. 2008;63:E815–E816. doi: 10.1227/01.NEU.0000325734.30302.97. discussion E816. [DOI] [PubMed] [Google Scholar]
- 3.Brodsky JR, Smith TW, Litofsky S, Lee DJ. Lipoma of the cerebellopontine angle. Am J Otolaryngol. 2006;27:271–274. doi: 10.1016/j.amjoto.2005.11.002. [DOI] [PubMed] [Google Scholar]
- 4.Jannetta PJ. Treatment of trigeminal neuralgia by suboccipital and transtentorial cranial operations. Clin Neurosurg. 1977;24:538–549. doi: 10.1093/neurosurgery/24.cn_suppl_1.538. [DOI] [PubMed] [Google Scholar]
- 5.Kato T, Sawamura Y, Abe H. Trigeminal neuralgia caused by a cerebellopontine-angle lipoma : case report. Surg Neurol. 1995;44:33–35. doi: 10.1016/0090-3019(95)00056-9. [DOI] [PubMed] [Google Scholar]
- 6.Kawashima M, Matsushima T, Inoue T, Mineta T, Masuoka J, Hirakawa N. Microvascular decompression for glossopharyngeal neuralgia through the transcondylar fossa (supracondylar transjugular tubercle) approach. Neurosurgery. 2010;66(6 Suppl Operative):275–280. doi: 10.1227/01.NEU.0000369662.36524.CF. discussion 280. [DOI] [PubMed] [Google Scholar]
- 7.Kondo A. Follow-up results of using microvascular decompression for treatment of glossopharyngeal neuralgia. J Neurosurg. 1998;88:221–225. doi: 10.3171/jns.1998.88.2.0221. [DOI] [PubMed] [Google Scholar]
- 8.Moretti R, Torre P, Antonello RM, Bava A, Cazzato G. Gabapentin treatment of glossopharyngeal neuralgia : a follow-up of four years of a single case. Eur J Pain. 2002;6:403–407. doi: 10.1016/s1090-3801(02)00026-5. [DOI] [PubMed] [Google Scholar]
- 9.Mukherjee P, Street I, Irving RM. Intracranial lipomas affecting the cerebellopontine angle and internal auditory canal : a case series. Otol Neurotol. 2011;32:670–675. doi: 10.1097/MAO.0b013e31821179e0. [DOI] [PubMed] [Google Scholar]
- 10.Patel A, Kassam A, Horowitz M, Chang YF. Microvascular decompression in the management of glossopharyngeal neuralgia : analysis of 217 cases. Neurosurgery. 2002;50:705–710. doi: 10.1097/00006123-200204000-00004. discussion 710-711. [DOI] [PubMed] [Google Scholar]
- 11.Resnick DK, Jannetta PJ, Bissonnette D, Jho HD, Lanzino G. Microvascular decompression for glossopharyngeal neuralgia. Neurosurgery. 1995;36:64–68. doi: 10.1227/00006123-199501000-00008. discussion 68-69. [DOI] [PubMed] [Google Scholar]
- 12.Stanic S, Franklin SD, Pappas CT, Stern RL. Gamma knife radiosurgery for recurrent glossopharyngeal neuralgia after microvascular decompression. Stereotact Funct Neurosurg. 2012;90:188–191. doi: 10.1159/000338089. [DOI] [PubMed] [Google Scholar]
- 13.Stieber VW, Bourland JD, Ellis TL. Glossopharyngeal neuralgia treated with gamma knife surgery : treatment outcome and failure analysis. Case report. J Neurosurg. 2005;102(Suppl):155–157. doi: 10.3171/jns.2005.102.s_supplement.0155. [DOI] [PubMed] [Google Scholar]
- 14.White JR, Carlson ML, Van Gompel JJ, Neff BA, Driscoll CL, Lane JI, et al. Lipomas of the cerebellopontine angle and internal auditory canal : Primum Non Nocere. Laryngoscope. 2013;123:1531–1536. doi: 10.1002/lary.23882. [DOI] [PubMed] [Google Scholar]
- 15.Yilmaz N, Unal O, Kiymaz N, Yilmaz C, Etlik O. Intracranial lipomas--a clinical study. Clin Neurol Neurosurg. 2006;108:363–368. doi: 10.1016/j.clineuro.2005.04.003. [DOI] [PubMed] [Google Scholar]
- 16.Yomo S, Arkha Y, Donnet A, Régis J. Gamma Knife surgery for glossopharyngeal neuralgia : report of 2 cases. J Neurosurg. 2009;110:559–563. doi: 10.3171/2008.8.17641. [DOI] [PubMed] [Google Scholar]
- 17.Zimmermann M, Kellermann S, Gerlach R, Seifert V. Cerebellopontine angle lipoma : case report and review of the literature. Acta Neurochir (Wien) 1999;141:1347–1351. doi: 10.1007/s007010050440. [DOI] [PubMed] [Google Scholar]