

Abstract
INTRODUCTION
Rett syndrome is a progressive neurodevelopment disorder in which MECP gene mutations are responsible and might be related to cancer.
PRESENTATION OF CASE
A 22 year-old girl with Rett syndrome was hospitalized for abdominal distention and shock. Abdominal tenderness and distention were revealed in physical examination. Radiological investigations revealed sigmoid volvulus and colonic obstruction. Sigmoid volvulus, sigmoid colon perforation due to sigmoid cancer with liver metastasis were observed at laparotomy. Hartman procedure performed. The patient died on the second postoperative day.
DISCUSSION
Rett syndrome has several gastrointestinal pathologies related with inadequate parasympathetic control. Genetic mutations in methyl-CpG-binding protein 2 (MECP2) which has role in several cancer mechanisms is the reason of Rett syndrome. Colon cancer with the underlying gastrointestinal pathologies complicated our case.
CONCLUSION
Rett syndrome patients need a high level of concern for gastrointestinal emergencies with cancer risk.
Keywords: Rett syndrome, Colon cancer, Sigmoid volvulus
1. Introduction
Rett syndrome is a progressive neurodevelopmental disorder of the gray matter of the brain. Rett syndrome is diagnosed with clinical findings which have been mentioned by Hagberg et al. in 1988 and last by Neul et al. in 2010.1 Clinical features of Rett syndrome includes autistic behaviors, stereotyped movements, mental retardation, breathing problems, abdominal distension, scoliosis, diminished sensitivity to pain and gastrointestinal motility disorders.1
Rett syndrome is a result of MECP2 (methyl-CpG-binding protein 2) gene mutations. The mutations of MECP2 are not only related with neurodevelopmental problems but also MECP2 has role in carcinogenesis.2 Although linkages between MECP2 expression changes and colon, prostate and breast cancer have been shown, there has not been published Rett syndrome case with cancer.3
Here in we report a 22 years old girl diagnosed as Rett syndrome presented with sigmoid volvulus, ileus who had been underwent operation and sigmoid tumor with liver metastasis was detected. The aim of this paper is to emphasize the importance of constipation in patients with Rett syndrome and mention the possible relationship between Rett syndrome and colon cancer.
2. Case report
A 22-year-old girl admitted with abdominal distention, vomiting, constipation and hyperventilation episodes lasting for 1 week. She was diagnosed as Rett syndrome at 3 years old. Seizure disorders, constipation and air swallowing were the major symptoms obtained from the medical history. Also it was learned from the family that the patient had difficulty in evacuation of stool from the rectum for a long time. The family was using rectal enema during constipation or rectal digitation for defecation. It was learned that there had been no stool discharge for 4 days. In her physical examination, abdominal distension, abdominal tenderness, rebound, septic appearance were revealed. Bloody discharge was observed in rectal examination. Increased sphincter tonus was palpated in rectal examination. Turgol-tonus was decreased. Abdominal X-ray showed dilated bowel segments with air-fluid levels. There is a coffee-bean sign on the lower left quadrant indicating sigmoid volvulus (Picture 1). The patient was diagnosed as acute abdomen due to sigmoid volvulus. Preoperative laboratory evaluation including coagulation function and liver function were normal. Blood Urea Nitrogen, creatinine, white blood cell count, serum sodium, blood glucose, and plasma CRP levels were increased. Blood gases showed acute metabolic acidosis. Electrocardiography showed sinus tachycardia with 500 ms QT interval. In the urgent laparotomy, sigmoid volvulus was seen. There was a 2 cm hard mass below the twisting point resembling colon tumor (Picture 2). In the abdominal exploration, there were several hard nodular lesions in the liver. Hartman procedure and liver biopsy were performed. In the postoperative period, the patient was followed with septic shock. Although intensive care management was given, pulmonary and cardiac functions deteriorated and the patient suddenly died on the second postoperative day. Pathology result was musinous adenocarinoma with a diameter of 3 cm. Liver mass pathology revealed adenocarcinoma metastasis. Although permission is taken from the relatives for the study, no further genetic analysis was performed because of the refusal of the relatives.
Picture 1.
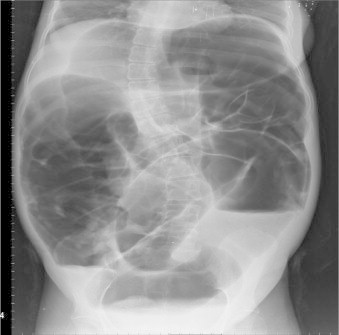
The abdominal X-ray evaluation of the Rett syndrome patient. Dilated colon segments are seen on the X-ray. Dilated small intestine is also observed. There a colonic loupe on the left lower quadrant. Scoliosis is seen on the abdominal X-ray.
Picture 2.
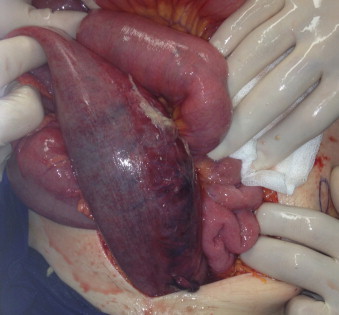
Sigmoid colon tumor located at the twisting point of sigmoid volvulus. Dilated colon is observed just proximal to sigmoid colon tumor.
3. Discussion
Rett syndrome is characterized by early neurological regression that severely affects motor, cognitive and communication skills. The immature neuronal network due to MECP gene mutation may lead inadequate parasympathetic control. For this reason neurodevelopment disorder not only affect the cognition but also the digestive system also. Oromotor or upper gastrointestinal dysfunction is observed in 75% of cases consist of esophageal dysmotility (46%), delayed esophageal emptying, esophageal atony, gastroesophageal reflux (23%), gastric dismotility (69%), excessive air swallowing, difficulty in swallowing.4 While decreased intestine motility results in constipation, air swallowing leads bloating of the abdomen. There are reported cases in which emergency operations were performed due to gastrointestinal pathologies.5 Our case is an example for chronic constipation and swallowing problems of Rett syndrome. Lack of defecation for 4 days with continuing air swallowing had led increased bowel gas and abdominal distension.
Defecation is a complex mechanism coordinated by autonomic and somatic innervations. Excitatory and inhibitory components of parasympathetic pathways have important roles in colonic propulsive activity and relaxation for adequate defecation.6 In our study there was increased anal sphincter tonus and history of rectal digitation for defecation. This might have been result of inadequate parasympathetic control of Rett syndrome. It might be speculated that uncoordinated parasympathetic innervation might be seen in Rett syndrome. This might be a subject of future studies. Habits of the family in order to cure the constipation of the patient might have been well-intentioned behavior, but this led late admission to the hospital. As the patients with Rett syndrome have decreased pain sensation, our patient admitted to the hospital till when she had become septic shock.7 Septic shock complicated the situation of the patient.
The majority of Rett patients are known to have mutations in MECP2. The interactions of MECP2 with nucleus result in deacetylation of histones and chromatin condensation, which leads to repression of transcription.8 An additional role for MECP2 during carcinogenesis has recently been described in several studies. The hypermethylation of tumor suppressor gene promoters is a well-characterized event in carcinogenesis like hepatocellular carcinoma.9 Hypermethylation of tumor suppressor genes in cancer has been associated with MECP2.2 Colonic carcinoma showed strong MECP2 expression. In the study of Darwanto et al.,10 there has been close relation between MECP2 function and colon cancer. However there has not been any reported Rett syndrome with colon cancer before. Time required for cancer occurrence may not be achieved in recent cases or our case might be sporadic. Our case is the first reported Rett syndrome with colon cancer. Our case might be sporadic case but close relationship between cancer and Rett syndrome might be also. For this reason future researches are needed.
4. Conclusion
Rett syndrome and cancer have common genetic mutations. Coexistence of colon cancer and Rett syndrome is presented in our case. A high level of concern should be taken in patients with Rett syndrome.
Conflict of interest
No conflict of interest.
Funding
No funding support.
Ethical approval
Written informed consent was taken from the parents of the patient.
Authors contributions
U.Y., A.G., G.P. collected the data, searched the literature.
U.Y., A.G. wrote the article.
G.P., E.O. controlled the article.
Key learning points
-
•
Although not seen before, Rett syndrome and cancer has common genetic ground.
-
•
Several findings of Rett syndrome might mask the coexistence of cancer and should be suspected by the physician.
References
- 1.Neul J.L., Kaufmann W.E., Glaze D.G., Christodulou J., Clarke A.J. Rett syndrome: revised diagnostic criteria and nomenclature. Ann Neurol. 2010;68:944–950. doi: 10.1002/ana.22124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Adkins N.L., Georgel P.T. MeCP2: structure and function. Biochem Cell Biol. 2011;89:1–11. doi: 10.1139/O10-112. [DOI] [PubMed] [Google Scholar]
- 3.Bernard D., Gil J., Dumont P., Rizzo S., Monte D., Quatannens B. The methyl-CpG-binding protein MECP is required for prostate cancer cell growth. Oncogene. 2006;25(9):1358–1366. doi: 10.1038/sj.onc.1209179. [DOI] [PubMed] [Google Scholar]
- 4.Motil K.J., Schultz R.J., Browning K., Trautwein L., Glaze D.G. Oropharyngeal dysfunction and gastroesophageal dysmotility are present in girls and women with Rett syndrome. J Pediatr Gastroenterol Nutr. 1999;29:31–37. doi: 10.1097/00005176-199907000-00010. [DOI] [PubMed] [Google Scholar]
- 5.Asezer A., Yagcı M.A., Hatipolu A.R. The management of gastric perforation in a girl with Rett syndrome: report of a case. Brain Dev. 2011;33:83–85. doi: 10.1016/j.braindev.2010.01.005. [DOI] [PubMed] [Google Scholar]
- 6.Gonella J., Bouvier M., Blanquet F. Extrinsic nervous control of motility of small and large intestines and related sphincters. Physiol Rev. 1987;67:902–961. doi: 10.1152/physrev.1987.67.3.902. [DOI] [PubMed] [Google Scholar]
- 7.Devarakonda K.M., Lowthian D., Raghavendra T. A case of Rett syndrome with reduced pain sensitivity. Paediatr Anaesth. 2009;19(June (6)):625–627. doi: 10.1111/j.1460-9592.2009.03018.x. [DOI] [PubMed] [Google Scholar]
- 8.Wan M., Zhao K., Francke U. MECP2 truncating mutations cause histone H4 hyperacetylation in Rett syndrome. Hum Mol Genet. 2001;10:1085–1092. doi: 10.1093/hmg/10.10.1085. [DOI] [PubMed] [Google Scholar]
- 9.Bakker J., Lin X., Nelson W.G. Methyl-CpG binding domain protein 2 represses transcription from hypermethylated (pi-class glutathione S-transferase gene promoters in hepatocellular carcinoma cells. J Biol Chem. 2002;277:22573–22580. doi: 10.1074/jbc.M203009200. [DOI] [PubMed] [Google Scholar]
- 10.Darwanto A., Kitazawwa R., Maeda S., Kitazawa S. MeCP2 and promoter methylation cooperatively regulate E-cadherin gene expression in colorectal carcinoma. Cancer Sci. 2003;94:442–447. doi: 10.1111/j.1349-7006.2003.tb01462.x. [DOI] [PMC free article] [PubMed] [Google Scholar]