

Abstract
The sacral percutaneous fixation has many advantages but can be associated with a significant exposure to X-ray radiation. Currently, sacroiliac screw fixation represents the only minimally invasive technique to stabilize the posterior pelvic ring. It is a technique that should be used by experienced surgeons. We present a practical review of important aspects of this technique.
Keywords: Minimally invasive surgery, percutaneous screw fixation, sacrum
INTRODUCTION
Sacroiliac screws (SISs) has been used since Vidal et al.[32] introduced its use in 1973. Since that, SIS has become a common technology in fixing pelvic posterior ring injuries.[11,37] SIS has made important progress in the treatment of posterior pelvic ring injury during the past 20 years. However, some clinical reports showed that conventional SIS may not universally result in sufficiently stable fixation.[37]
Currently, SIS fixation represents the only minimally invasive technique to stabilize the posterior pelvic ring.[20] For that reason, it is steadily gaining popularity, becoming one of the most commonly used techniques. Some indications for this technique include sacroiliac joint dislocations, sacral fractures, certain iliac crescent fractures and combinations of those injuries.[4,11] The sacrum, serving as the foundation of the spine, transmits the stress between spine and pelvis through sacroiliac joints.[35] Thus, the goal of surgical fixation is the reconstruction of the spine-pelvic-junction to allow early weight-bearing and to facilitate nursing care, particularly for multiple injured patients.[6]
To overcome the biomechanical limitations faced by the single iliac screw technique, the dual iliac screw technique was developed.[35] Have been demonstrated that the dual iliac screw technique provides good clinical results for patients with a partial or total sacrectomy with no iliac screw failure,[1,7,9] confirming the biomechanical advantage of dual over single iliac screw in restoring the stability of the lumbo-iliac fixation construct in vertical and rotational planes.[35] However, clinical practices caution that the dual iliac screw technique may increase bone stock loss, prominence of the instrumentation, and screw-rod connection difficulty as compared with the single iliac screw technique.[36]
The aim of this work is, through a nonexhaustive review of the literature expose current considerations about SIS fixation technique.
THE TECHNIQUE
Lengthened sacro-iliac screw
This technique obtains fixation by traversing bilateral sacroiliac joints and the sacral body, this technique can solve the problem of bilateral sacroiliac joint fractures and dislocations.[10,25] In the past were commonly used two techniques, the oblique method of SIS placement, in which the screw is obliquely aligned, directed inferiorly to superiorly and posteriorly to anteriorly, and the transverse alignment of the SIS through the sacral ala on both the inlet and outlet views of the sacrum. With the first technique was an increased the risk of unrecognized anterior protrusion of screws beyond the sacral body, and with the second-technique results in a smaller secured area of the sacral isthmus bone.[20] The current procedure technique is the SIS under fluoroscopic observation with the standard Matta projections anterior-posterior (a.p.), inlet, outlet [Figures 1 and 2].
Figure 1.
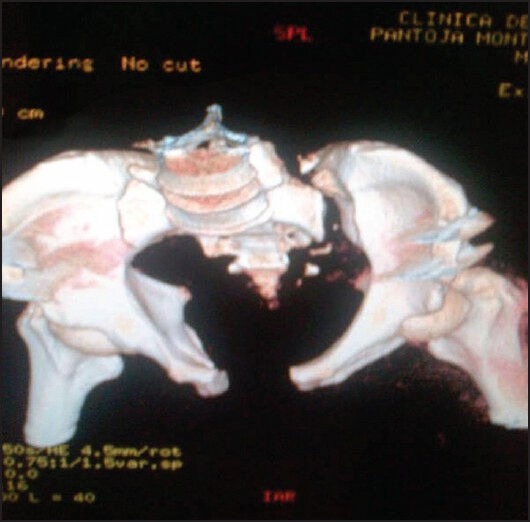
Computed tomography scan three-dimensional of sacral luxation
Figure 2.
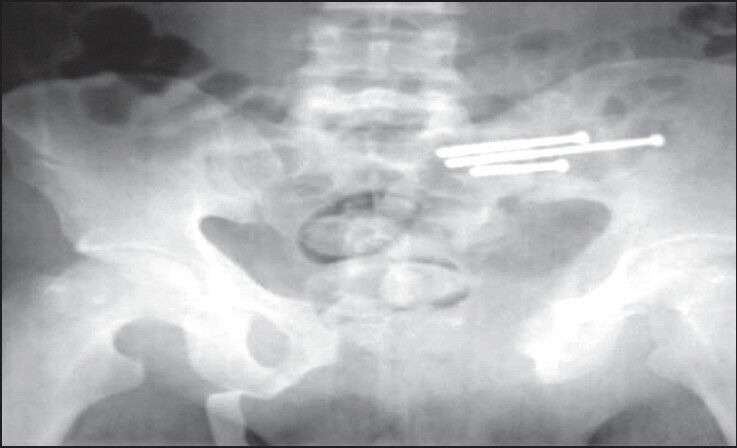
Intraoperative radiography showing transverse alignment of SIS fixation
Sacroiliac screw fixation is technically challenging and can be contraindicated depending on the shape of the sacrum.[15] The lack of direct visualization and limited tactile control complicate precise screw insertion.[13,26] The surgeon has to decide if an extrapolated implant position will match a secure inner-bony position orienting on planar fluoroscopic images in different projections. In addition, image interpretation is aggravated by the high degree of shape variability of the upper sacrum.[20] This circumstance unavoidably results in increased X-ray exposure for the patient and the surgeon due to more frequent application of image intensifier. Aberrant screw or wire placement can lead to significant complications, including injury to the fifth-lumbar nerve root, sacral venous plexus, iliac vessels, or cauda equina.[24]
Iliac screws offer advantages of improved bio-mechanics. They permit iliac crest bone harvesting and have shown to have high-fusion rates, in long fusions and are valuable for the use in high-grade spondylolisthesis.[17] There may, however, be hardware prominence and exposure may be somewhat difficult. As well, they offer advantages for correction of pelvic obliquity and for revision surgery and do not violate the sacroiliac joint. Disadvantages may occur, as a result, of difficulties in insertion.[17]
Have been reported rates of implant malposition of up to 18-25%,[4,11,12,25,30] which are potentially associated with iatrogenic neurovascular lesions. Lengthened SIS is more applicable to repair surgery after first failure of the SIS fixation,[3] but overall SIS fixation is indicated in nondisplaced unstable sacroiliac joint injuries or sacral fractures.[19]
In the experimental setup, have been demonstrated that two ipsilateral screws provide more biomechanical stability than the one.[34,38] However, using conventional fluoroscopy, many surgeons limit the placement of iliosacral screws to the pedicles of S1, as those of S2 are narrow and difficult to visualize [Figure 2].[21]
The screws are placed through the outer table of the ilium, through the S1 joint and into the lateral sacrum.[23] This bone channel has been well-described and regularly used in pelvic trauma applications for screw placement. It has also been performed with an open and percutaneous technique. With the development of adjunctive devices for Cotrel-Dubosset instrumentation, a monoblock was developed to use this trajectory for screw fixation.
Recently, Pan et al.[22] have introduced a SIS fixation guide and evaluated its efficacy in fixation of sacroiliac joint fracture-dislocations, they found that the minimally invasive guide can eliminate discrepancies resulting from the surgeon's own sensory input when inserting screws under the guidance of computed tomography (CT), making percutaneous iliosacral screw fixation more accurate, safe and simple. The use of a guide can curtail the surgical time to about 14 min.
Radiological considerations
As previously mentioned, is widely used the fluoroscopy control for the placement of the screws. This leads the technique being highly dependent on fluoroscopic technician, and on the operator's ability not only to interpret the fluoroscopic images but also to control wire placement based on this interpretation.[24] Using the conventional fluoroscopy-based technique, the drilling can only be controlled in one projection at once; thus, the position of the screws must be followed and adjusted under fluoroscopy in a.p., inlet, outlet and lateral projections. All this result in increased radiation exposure for the patient and the surgeon.[5] Have been reported injuries to nerve roots and the gluteal vessels in up to 3-15% of cases using this method.
Navigation systems have been introduced for traumatological indications, especially in the field of spine and pelvic surgery[2,8,14,27,29,31,33] With the aim to increase precision of screw positioning, various techniques for CT-guided/computer-navigated screw positioning were described.[16,18,28,30] The potential advantages of CT-guided placement of percutaneous hollow screws are that it is a simple operation, the screws are accurately located, there is less hemorrhage, minimal injuries and strong fixation is achieved.[22]
However, in the emergency room (ER) with patients in urgent need for early primary care, these time-consuming techniques are unsuitable. Thus, fluoroscopy provides a straightforward and inexpensive approach to intraoperative visualization.[21] Some techniques, such as Iso-C3D navigation demonstrates superiority to fluoroscopy navigation for SIS fixation in an experimental set-up designed to assess the accuracy.[5]
EVIDENCE
Comparing the stability of lengthened SIS and SIS for the treatment of bilateral vertical sacral fractures, Zhao et al.[37] in a finite element model of Tile C pelvic ring injury (bilateral type Denis II fracture of the sacrum) demonstrated that:
The stability of one lengthened SIS fixation in the S1 or S2 segment is superior to that of two bidirectional SIS in the same sacral segment
The stability of one lengthened SIS fixation in S1 and S2 segments, respectively, is superior to that of two bidirectional SIS fixation in S1 and S2 segments, respectively
The stability of one lengthened SIS fixation in S1 and S2 segments, respectively, is superior to that of one lengthened SIS fixation in the S1 or S2 segment
The stability of two bidirectional SIS fixation in S1 and S2 segments, respectively, is markedly superior to that of two bidirectional SIS fixation in the S1 or S2 segment and is also markedly superior to that of one SIS fixation in the S1 segment and one SIS fixation in the S2 segment
The vertical stability of the lengthened SIS or the SIS fixation in S2 is superior to that of S1
The rotational stability of the lengthened SIS or SIS fixation in S1 is superior to that of S2.
CONCLUSIONS
Sacroiliac screw fixation is a commonly used procedure for iliosacral joint fracture-dislocations and sacral fractures. Currently, the standard technique is the percutaneous iliosacral screw fixation under conventional C-arm fluoroscopy that often exposes the patient to prolonged radiation. Unfortunately, even experienced surgeons can have a high rate of screw malposition and nerve and vessel injuries, being that the reason because SIS fixation should be performed under better technology control, but in the ER setting, this could be laborious and can finish in a loss of time for the patient treatment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Acharya NK, Bijukachhe B, Kumar RJ, Menon VK. Ilio-lumbar fixation - the Amrita technique. J Spinal Disord Tech. 2008;21:493–9. doi: 10.1097/BSD.0b013e31815b5cc4. [DOI] [PubMed] [Google Scholar]
- 2.Bale RJ, Kovacs P, Dolati B, Hinterleithner C, Rosenberger RE. Stereotactic CT-guided percutaneous stabilization of posterior pelvic ring fractures: A preclinical cadaver study. J Vasc Interv Radiol. 2008;19:1093–8. doi: 10.1016/j.jvir.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 3.Beaulé PE, Antoniades J, Matta JM. Trans-sacral fixation for failed posterior fixation of the pelvic ring. Arch Orthop Trauma Surg. 2006;126:49–52. doi: 10.1007/s00402-005-0069-2. [DOI] [PubMed] [Google Scholar]
- 4.van den Bosch EW, van Zwienen CM, van Vugt AB. Fluoroscopic positioning of sacroiliac screws in 88 patients. J Trauma. 2002;53:44–8. doi: 10.1097/00005373-200207000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Citak M, Hüfner T, Geerling J, Kfuri M, Jr, Gänsslen A, Look V, et al. Navigated percutaneous pelvic sacroiliac screw fixation: Experimental comparison of accuracy between fluoroscopy and Iso-C3D navigation. Comput Aided Surg. 2006;11:209–13. doi: 10.3109/10929080600890015. [DOI] [PubMed] [Google Scholar]
- 6.Dawei T, Na L, Jun L, Wei J, Lin C. A novel fixation system for sacroiliac dislocation fracture: Internal fixation system design and biomechanics analysis. Clin Biomech (Bristol, Avon) 2013;28:129–33. doi: 10.1016/j.clinbiomech.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 7.Dickey ID, Hugate RR, Jr, Fuchs B, Yaszemski MJ, Sim FH. Reconstruction after total sacrectomy: Early experience with a new surgical technique. Clin Orthop Relat Res. 2005;438:42–50. doi: 10.1097/01.blo.0000180054.76969.41. [DOI] [PubMed] [Google Scholar]
- 8.Frank M, Dedek T. Percutaneous iliosacral screw placement using a radiolucent drive. Acta Orthop Belg. 2012;78:519–22. [PubMed] [Google Scholar]
- 9.Fujibayashi S, Neo M, Nakamura T. Palliative dual iliac screw fixation for lumbosacral metastasis. Technical note. J Neurosurg Spine. 2007;7:99–102. doi: 10.3171/SPI-07/07/099. [DOI] [PubMed] [Google Scholar]
- 10.Gardner MJ, Routt ML., Jr Transiliac-transsacral screws for posterior pelvic stabilization. J Orthop Trauma. 2011;25:378–84. doi: 10.1097/BOT.0b013e3181e47fad. [DOI] [PubMed] [Google Scholar]
- 11.Giannoudis PV, Papadokostakis G, Alpantaki K, Kontakis G, Chalidis B. Is the lateral sacral fluoroscopic view essential for accurate percutaneous sacroiliac screw insertion. An experimental study? Injury. 2008;39:875–80. doi: 10.1016/j.injury.2008.01.049. [DOI] [PubMed] [Google Scholar]
- 12.Gänsslen A, Hüfner T, Krettek C. Percutaneous iliosacral screw fixation of unstable pelvic injuries by conventional fluoroscopy. Oper Orthop Traumatol. 2006;18:225–44. doi: 10.1007/s00064-006-1173-3. [DOI] [PubMed] [Google Scholar]
- 13.Hilgert RE, Finn J, Egbers HJ. Technique for percutaneous iliosacral screw insertion with conventional C-arm radiography. Unfallchirurg. 2005;108:954, 956–60. doi: 10.1007/s00113-005-0967-3. [DOI] [PubMed] [Google Scholar]
- 14.Iguchi T, Ogawa K, Doi T, Miyasho K, Munetomo K, Hiraki T, et al. Computed tomography fluoroscopy-guided placement of iliosacral screws in patients with unstable posterior pelvic fractures. Skeletal Radiol. 2010;39:701–5. doi: 10.1007/s00256-009-0826-3. [DOI] [PubMed] [Google Scholar]
- 15.Ilharreborde B, Breitel D, Lenoir T, Mosnier T, Skalli W, Guigui P, et al. Pelvic ring fractures internal fixation: Iliosacral screws versus sacroiliac hinge fixation. Orthop Traumatol Surg Res. 2009;95:563–7. doi: 10.1016/j.otsr.2009.08.002. [DOI] [PubMed] [Google Scholar]
- 16.Konrad G, Zwingmann J, Kotter E, Südkamp N, Oberst M. Variability of the screw position after 3D-navigated sacroiliac screw fixation. Influence of the surgeon's experience with the navigation technique. Unfallchirurg. 2010;113:29–35. doi: 10.1007/s00113-008-1546-1. [DOI] [PubMed] [Google Scholar]
- 17.Kostuik JP. Spinopelvic fixation. Neurol India. 2005;53:483–8. doi: 10.4103/0028-3886.22618. [DOI] [PubMed] [Google Scholar]
- 18.Kraus MD, Krischak G, Keppler P, Gebhard FT, Schuetz UH. Can computer-assisted surgery reduce the effective dose for spinal fusion and sacroiliac screw insertion? Clin Orthop Relat Res. 2010;468:2419–29. doi: 10.1007/s11999-010-1393-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mendel T, Noser H, Wohlrab D, Stock K, Radetzki F. The lateral sacral triangle - A decision support for secure transverse sacroiliac screw insertion. Injury. 2011;42:1164–70. doi: 10.1016/j.injury.2010.03.016. [DOI] [PubMed] [Google Scholar]
- 20.Mendel T, Radetzki F, Wohlrab D, Stock K, Hofmann GO, Noser H. CT-based 3-D visualisation of secure bone corridors and optimal trajectories for sacroiliac screws. Injury. 2013;44:957–63. doi: 10.1016/j.injury.2012.11.013. [DOI] [PubMed] [Google Scholar]
- 21.Osterhoff G, Ossendorf C, Wanner GA, Simmen HP, Werner CM. Posterior screw fixation in rotationally unstable pelvic ring injuries. Injury. 2011;42:992–6. doi: 10.1016/j.injury.2011.04.005. [DOI] [PubMed] [Google Scholar]
- 22.Pan WB, Liang JB, Wang B, Chen GF, Hong HX, Li QY, et al. The invention of an iliosacral screw fixation guide and its preliminary clinical application. Orthop Surg. 2012;4:55–9. doi: 10.1111/j.1757-7861.2011.00162.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Polly DW, Jr, Latta LL. Spinopelvic fixation biomechanics. Semin Spine Surg. 2004;16:101–6. [Google Scholar]
- 24.Riehl J, Widmaier J. A simulator model for sacroiliac screw placement. J Surg Educ. 2012;69:282–5. doi: 10.1016/j.jsurg.2011.10.012. [DOI] [PubMed] [Google Scholar]
- 25.Routt ML, Jr, Kregor PJ, Simonian PT, Mayo KA. Early results of percutaneous iliosacral screws placed with the patient in the supine position. J Orthop Trauma. 1995;9:207–14. doi: 10.1097/00005131-199506000-00005. [DOI] [PubMed] [Google Scholar]
- 26.Routt ML, Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: Early complications of the percutaneous technique. J Orthop Trauma. 1997;11:584–9. doi: 10.1097/00005131-199711000-00007. [DOI] [PubMed] [Google Scholar]
- 27.Sciulli RL, Daffner RH, Altman DT, Altman GT, Sewecke JJ. CT-guided iliosacral screw placement: Technique and clinical experience. AJR Am J Roentgenol. 2007;188:W181–92. doi: 10.2214/AJR.05.0479. [DOI] [PubMed] [Google Scholar]
- 28.Sun YQ, Citak M, Kendoff D, Gansslen A, Krettek C, Hufner T. Navigated percutaneous placement of iliosacral screws using intra-operative three-dimensional imaging. Zhonghua Yi Xue Za Zhi. 2008;88:3226–9. [PubMed] [Google Scholar]
- 29.Tjardes T, Paffrath T, Baethis H, Shafizadeh S, Steinhausen E, Steinbuechel T, et al. Computer assisted percutaneous placement of augmented iliosacral screws: A reasonable alternative to sacroplasty. Spine (Phila Pa 1976) 2008;33:1497–500. doi: 10.1097/BRS.0b013e318175c25c. [DOI] [PubMed] [Google Scholar]
- 30.Tonetti J, Cazal C, Eid A, Badulescu A, Martinez T, Vouaillat H, et al. Neurological damage in pelvic injuries: A continuous prospective series of 50 pelvic injuries treated with an iliosacral lag screw. Rev Chir Orthop Reparatrice Appar Mot. 2004;90:122–31. doi: 10.1016/s0035-1040(04)70033-1. [DOI] [PubMed] [Google Scholar]
- 31.Trumm CG, Rubenbauer B, Piltz S, Reiser MF, Hoffmann RT. Screw placement and osteoplasty under computed tomographic-fluoroscopic guidance in a case of advanced metastatic destruction of the iliosacral joint. Cardiovasc Intervent Radiol. 2011;34(Suppl 2):S288–93. doi: 10.1007/s00270-009-9716-2. [DOI] [PubMed] [Google Scholar]
- 32.Vidal J, Allieu Y, Fassio B, Adrey J, Goalard C. Spondylolisthesis: Reduction with Harrington's rods. Rev Chir Orthop Reparatrice Appar Mot. 1973;59:21–41. [PubMed] [Google Scholar]
- 33.Wang MY, Williams S, Mummaneni PV, Sherman JD. Minimally invasive percutaneous iliac screws: Initial 24 case experience with CT confirmation. J Spinal Disord Tech. 2012 doi: 10.1097/BSD.0b013e3182733c43. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 34.Yinger K, Scalise J, Olson SA, Bay BK, Finkemeier CG. Biomechanical comparison of posterior pelvic ring fixation. J Orthop Trauma. 2003;17:481–7. doi: 10.1097/00005131-200308000-00002. [DOI] [PubMed] [Google Scholar]
- 35.Yu BS, Zhuang XM, Zheng ZM, Li ZM, Wang TP, Lu WW. Biomechanical advantages of dual over single iliac screws in lumbo-iliac fixation construct. Eur Spine J. 2010;19:1121–8. doi: 10.1007/s00586-010-1343-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yu BS, Zhuang XM, Li ZM, Zheng ZM, Zhou ZY, Zou XN, et al. Biomechanical effects of the extent of sacrectomy on the stability of lumbo-iliac reconstruction using iliac screw techniques: What level of sacrectomy requires the bilateral dual iliac screw technique? Clin Biomech (Bristol, Avon) 2010;25:867–72. doi: 10.1016/j.clinbiomech.2010.06.012. [DOI] [PubMed] [Google Scholar]
- 37.Zhao Y, Li J, Wang D, Liu Y, Tan J, Zhang S. Comparison of stability of two kinds of sacro-iliac screws in the fixation of bilateral sacral fractures in a finite element model. Injury. 2012;43:490–4. doi: 10.1016/j.injury.2011.12.023. [DOI] [PubMed] [Google Scholar]
- 38.van Zwienen CM, van den Bosch EW, Snijders CJ, Kleinrensink GJ, van Vugt AB. Biomechanical comparison of sacroiliac screw techniques for unstable pelvic ring fractures. J Orthop Trauma. 2004;18:589–95. doi: 10.1097/00005131-200410000-00002. [DOI] [PubMed] [Google Scholar]