

Abstract
Study Design:
Prospective single-center study.
Objective:
To analyze the efficacy and safety of a new technique of global vertebral correction with convex rod rotation performed on the patients with adolescent idiopathic scoliosis.
Summary of Background Data:
Surgical goal is to obtain an optimal curve correction in scoliosis surgery. There are various correction techniques. This report describes a new technique of global vertebral correction with convex rod rotation.
Materials and Methods:
A total of 12 consecutive patients with Lenke type I adolescent idiopathic scoliosis and managed by convex rod rotation technique between years 2012 and 2013 having more than 1 year follow-up were included. Mean age was 14.5 (range = 13-17 years) years at the time of operation. The hospital charts were reviewed for demographic data. Measurements of curve magnitude and balance were made on 36-inch standing anteroposterior and lateral radiographs taken before surgery and at most recent follow up to assess deformity correction, spinal balance, and complications related to the instrumentation.
Results:
Preoperative coronal plane major curve of 62° (range = 50°-72°) with flexibility of less than 30% was corrected to 11.5°(range = 10°-14°) showing a 81% scoliosis correction at the final follow-up. Coronal imbalance was improved 72% at the most recent follow-up assessment. No complications were found.
Conclusion:
The new technique of global vertebral correction with Ucar's convex rod rotation is an effective technique. This method is a vertebral rotation procedure from convex side and it allows to put screws easily to the concave side.
Keywords: Correction technique, rod rotation, scoliosis
INTRODUCTION
Scoliosis is a sideways curvature of the spine that occurs most often during the growth spurt just before puberty. It is a complex three-dimensional deformity of the spine with scoliosis in the coronal plane, lordosis or kyphosis in the sagittal plane and rotational deformity in the axial plane. Advanced cases may need surgery to keep the scoliosis from worsening and to straighten severe cases of scoliosis.[1] Scoliosis surgery is one of the most demanding surgical procedures in spine surgery. The aim with scoliosis surgery is to correct the curve and to hold it in a corrected position while a bony fusion occurs.[1,2] Currently there are various common curve correction techniques used in adolescent idiopathic scoliosis (AIS).[3,4,5,6,7,8,9,10] The following are the methods for adolescent idiopathic scoliosis reviewed in chronological order:
Harrington system (Distraction-compression)
Luque instrumentation system
CD instrumentation system (Simple rod rotation)
Rod Translation
Cantilever bending technique
Direct vertebral rotation
Vertebral co-planar alignment and
Simultaneous double rod rotation.
We reported a new technique called Ucar's Convex Rod Rotation (UCRR) which was not determined before. Our aim to show that global vertebral correction with UCRR could be used effectively in surgery for adolescent idiopathic scoliosis.
MATERIALS AND METHODS
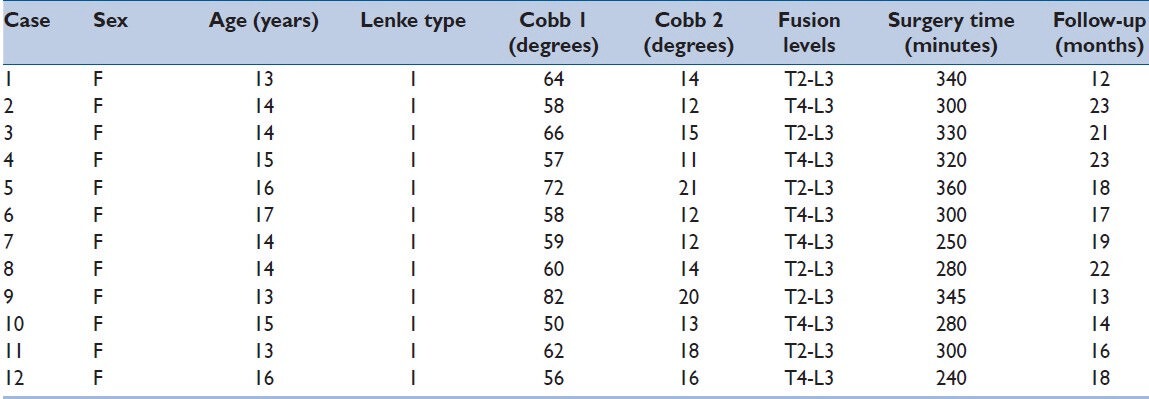
This is a prospective analysis of 12 consecutive patients with Lenke type I adolescent idiopathic scoliosis and managed by convex rod rotation technique between years 2012 and 2013. All patients were female with a mean age of 14.5 (range = 13-17 years) years at the time of operation [Table 1]. The hospital charts were reviewed for demographic data. Measurements of curve magnitude and balance were made on 36-inch standing anteroposterior and lateral radiographs taken before surgery and at most recent follow-up to assess deformity correction, spinal balance, and complications related to the instrumentation. The coronal curve was measured by the Cobb method. Coronal balance was measured as the distance between the C7 plumb line and the central sacral line. Global sagittal alignment was evaluated by standing lateral radiograph. The angle between the upper endplate of T2 and the lower endplate of T12 was measured as the global thoracic kyphosis, and the angle between the upper endplate of L1 and the upper endplate of S1 was measured as global lumbar lordosis. The distance between the vertical line drawn from the anteroinferior corner of the C7 body and the posterior superior corner of the S1 body was also measured as the sagittal balance.
Table 1.
Demographic and surgical data
SURGICAL TECHNIQUE
Firstly, the pedicle screws were inserted on convex side. Secondly, the screws were connected with a rod contoured to the shape of the deformity. Plugs were applied between the screws and the rod but not tightened. The rod was now rotated toward the convexity of the curve. After tightening the plugs on convex side we inserted screws on concave side easily. Second contoured rod was replaced to the concavity of the curve. Before tightening the plugs direkt vertebral rotation manoeuvre was done for all instrumented levels. Finally, the rods secured to the screws [Figure 1]. All surgeries were performed under motor-evoked potential monitoring and additionally wake up test was applied.
Figure 1.
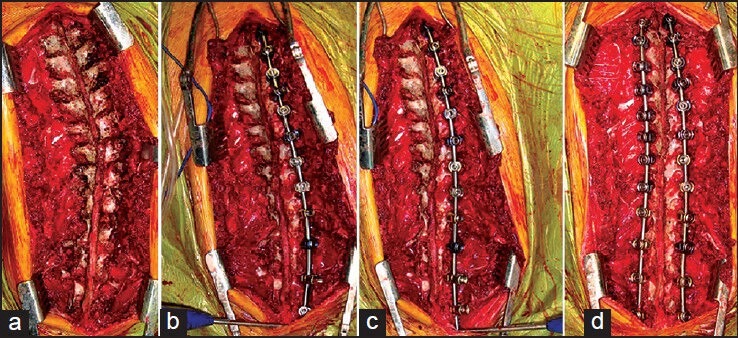
Per-operative images of Ucar's Convex Rod Rotation technique. (a) Before screwing. (b) A contoured rod is applied to the convexity of the curve after screwing the convex side. (c) The rod is rotated towards the convexity of the curve. (d) Second contoured rod is applied to the concavity of the curve after screwing the concave side
RESULTS
The minimum follow-up was 12 months, average of 18 (range = 12-23 months) months. The preoperative coronal plane major curve of 62° (range = 50°-72°) with flexibility of less than 30% was corrected to 14.8° (range = 11°-21°) showing a 76% scoliosis correction at the final follow-up [Figure 2]. Coronal imbalance was improved 80% at the most recent follow-up assessment. Both the data of preoperative and postoperative were shown in Table 1. All patients after surgery showed their baseline neurologic status. No complications were observed in the patients in both postoperatively and final follow-up.
Figure 2.
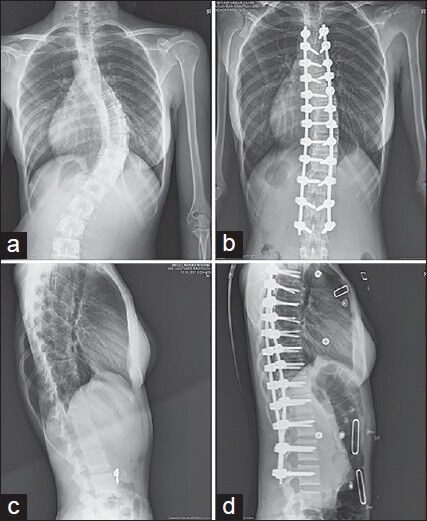
X-rays of the case 2. (a) Pre-operative X-ray (AP). (b) Post-operative X-ray (AP). (c) Pre-operative X-ray (Lateral). (d) Post-operative X-ray (Lateral)
DISCUSSION
Various surgical treatments for scoliosis were reported until now. The posterior approach has been the gold standard for years and continues to be a surgical procedure applicable to most patients since first introduced by Paul Harrington.[3] In the second generation instrumentation system developed by Cotrel and Dubousset,[4] correction was attempted by the rod-rotation maneuver. Currently various common curve correction techniques were used in AIS. The previous correction techniques were discussed in chronological order in this discussion section. The advantages and disadvantages of our technique were determined.
Distraction-compression technique in Harrington instrumentation system was primarily designed to apply distraction to the spine.[3] Harrington introduced a metal spinal system of instrumentation that assisted with straightening the spine, as well as holding it rigid while fusion took place in 1962. It marked the beginning of the great era of corrective scoliosis surgery for a long time.
Luque instrumentation system was reported in 1982.[5] Luque used laminar wires and rods to correct the deformity. A further advantage was that the contoured Luque rods were much more effective in preserving the normal sagittal profile of the spine, especially in the thoracolumbar and lumbar regions. The major defect of the Luque system was that it had no effect on derotating the vertebrae in the thoracic region, and had only a moderate effect in the thoracolumbar and lumbar regions.
Cotrel and Dubousset developed an instrumentation system pedicle screws and rods called CD instrumentation in 1988.[4] It was based on the realization of the three dimensional nature of the deformity with Simple rod rotation technique. In recent years all-screw systems have become the gold-standard technique for adolescent idiopathic scoliosis after CD instrumentation system. This technique did not only provide better lateral and frontal curve correction, but also a significant correction of vertebral rotation.
Another method in which the rod translation maneuver technique was used by Delorme in 1999 for obtaining reduction rather than a rotation maneuver.[6] The instrumented vertebrae were gradually translated toward the rod with the help of specialized instruments such as the persuader or with pedicle screw extensions.
Cantilever bending technique was reported by Chang in 2003.[7] In this correction technique six groups of pedicle screws were inserted on the upper, apical, and lower segments on both sides of a curve. The aim of this method was to correct the deformity on coronal plane by using a powerful corrective force. After the pedicle screw was positioned, a prebent rod was locked to the pedicle screws on the convex side. As two lever arms in the coronal plane, two long in situ benders were secured to the convex side of the rod in the coronal plane. The lever arms were brought closer to each other and a powerful corrective force was generated to correct the curve in the coronal plane.
Lee introduced a new concept in 2004 called Direct Vertebral Rotation which could effectively correct a substantial amount of rotational malalignment in scoliosis.[8] DVR was introduced as a procedure done along with the rod rotation maneuver. The concept was to correct vertebral rotation by application of a posterior force in the direction opposite to that of the deformity. After pedicle screws were applied and rod rotation was done to correct the coronal and sagittal deformity, torque was applied to the pedicle screws using long screw derotators on both concave and convex sides of the curve. Spinous process' were rotated to the convexity of the curve at the apical and juxtaapical vertebrae. In our cases we used DVR technique after rod rotation.
Vallespir introduced the vertebral coplanar alignment technique in 2008.[9] He claimed simultaneous recreation of coronal and sagittal profile along with correction of rotational deformity is achieved by the use of slotted longitudinal tubes attached to pedicle screws and aligning them linearly. In VCA, the pedicle screws were inserted in all vertebrae in the both sides. Then the correction was done by the convex side screws like our technique. However in our technique; firstly, the pedicle screws were inserted in all vertebrae in convex side. Secondly, rod rotation maneuver was done by the convex side screws. Finally, the concave side screws were inserted more easily.
Simultaneous double rod rotation technique was determined by Ito in 2010.[10] In this technique, unlike the prior, the rods were introduced on both sides of the curve and simultaneously rotated, brought about synchronous correction of the coronal as well as the sagittal profiles. This coupling of forces created a rotational moment at the apical vertebra which tended to derotate it.
As the disease progresses, the vertebrae and spinous processes in the area of the major curve rotate toward the concavity of the curve. On the concave side of the curve, the ribs are close together. On the convex side, they are widely separated. The vertebrae and intervertebral discs are decreased in height on the concave side. The pedicles are more thin. As the vertebral bodies rotate, the spinous processes deviate more and more to the concave side. Due to these pathologies, inserting screw to the concave side is more difficult and risky.
The most important difference of our technique was inserting the pedicle screws to the convex side firstly. While the screws were inserting to concave side firstly in all surgical techniques, in our technique the screws were inserted to convex side as a priority. When convex rod rotation maneuver was done concave side was screwed more easily. Whereby it could be considered to shorten the surgery time.
In conclusion, this is a preliminary report about a new method for surgical correction of adolescent idiopathic scoliosis, which allows a three-dimensional correction. In this study, our technique has shown good correction of the coronal curve and apical derotation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Hamzaoglu A, Talu U, Tezer M, Mirzanli C, Domanic U, Goksan SB. Assessment of curve flexibility in adolescent idiopathic scoliosis. Spine. 2005;30:1637–42. doi: 10.1097/01.brs.0000170580.92177.d2. [DOI] [PubMed] [Google Scholar]
- 2.Shakil H, Iqbal ZA, Al-Ghadir AH. Scoliosis: Review of types of curves, etiological theories and conservative treatment. J Back Musculoskelet Rehabil. 2014;27:111–5. doi: 10.3233/BMR-130438. [DOI] [PubMed] [Google Scholar]
- 3.Harrington PR. Treatment of scoliosis: Correction and internal fixation by spine instrumentation. J Bone Joint Surg Am. 1962;44:591–610. [PubMed] [Google Scholar]
- 4.Cotrel Y, Dubousset J, Guillaumat M. New universal instrumentation in spinal surgery. Clin Orthop. 1988;227:10–23. [PubMed] [Google Scholar]
- 5.Luque ER. Segmental spinal instrumentation for correction of scoliosis. Clin Orthop l. 982;;63:192–8. [PubMed] [Google Scholar]
- 6.Delorme S, Labelle H, Aubin CE, de Guise JA, Rivard CH, Poitras B, et al. Intraoperative comparison of two instrumentation techniques for the correction of adolescent idiopathic scoliosis. Rod rotation and translation. Spine. 1999;24:2011–7. doi: 10.1097/00007632-199910010-00009. [DOI] [PubMed] [Google Scholar]
- 7.Chang KW, Chang KI, Wu CM. Enhanced capacity for spontaneous correction of lumbar curve in the treatment of major thoracic-compensatory C modifier lumbar curve pattern in idiopathic scoliosis. Spine. 2007;32:3020–9. doi: 10.1097/BRS.0b013e31815cdde3. [DOI] [PubMed] [Google Scholar]
- 8.Lee SM, Suk SI, Chung ER. Direct vertebral rotation: A new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis. Spine. 2004;29:343–9. doi: 10.1097/01.brs.0000109991.88149.19. [DOI] [PubMed] [Google Scholar]
- 9.Vallespir GP, Flores JB, Trigueros IS, Sierra EH, Fernández PD, Olaverri JC, et al. Vertebral coplanar alignment: A standardized technique for three dimensional correction in scoliosis surgery: Technical description and preliminary results in Lenke type 1 curves. Spine. 2008;33:1588–97. doi: 10.1097/BRS.0b013e3181788704. [DOI] [PubMed] [Google Scholar]
- 10.Ito M, Abumi K, Kotani Y, Takahata M, Sudo H, Hojo Y, et al. Simultaneous double-rod rotation technique in posterior instrumentation surgery for correction of adolescent idiopathic scoliosis. J Neurosurg Spine. 2010;12:293–300. doi: 10.3171/2009.9.SPINE09377. [DOI] [PubMed] [Google Scholar]