

Abstract
Background: Pain on mid sternotomy incision site after Coronary Artery Bypass Graft Surgery (CABG) is a common problem that causes sleep disturbance, delayed wound healing, and increased use of analgesic drugs. Massage therapy which is mostly performed by healthcare providers is a non-pharmacological approach for managing this pain. The present study aimed to determine the effect of massage therapy by patient’s companion on the severity of pain in post CABG patients.
Methods: In this randomized single-blind clinical trial, 70 post CABG patients were randomly divided into an intervention and a control group. The intervention group received massage by one of their relatives who was trained by an expert nurse. The control group, on the other hand, received routine care. The pain intensity was assessed by Visual Analogue Scale (VAS) before and immediately, 30, 60, and 120 minutes after the intervention. Then, the data were entered into the SPSS statistical software (version 16) and analyzed using repeated measures ANOVA and post-hoc test (Scheffe).
Results: At the beginning of the study, no significant difference was found between the two groups regarding the pain severity. In the intervention group, the pain severity significantly decreased in all the four time points after the intervention (P=0.001). However, no significant difference was observed in this regard in the control group.
Conclusion: Massage therapy by patient’s companion trained by a nurse was an effective strategy for pain management in post CABG patients. This could also promote the patient’s family participation in the process of care.
Trial Registration Number: IRCT201208218505N3.
Keywords: Massage Therapy, Companion, Pain, Coronary Artery Bypass Graft Surger
Introduction
Coronary Vascular Diseases (CVD) are the most prevalent heart diseases that are mostly treated using non-invasive methods. Although these therapeutic methods are effective, many sufferers may need vascular repair. Coronary Artery Bypass Graft surgery (CABGs) is one of the common and effective treatments for reduction or removal of cardiac angina.1 Considering the prevalent application of this therapeutic method throughout the world, we could claim that CABG provides an opportunity to increase the quality of life of thousands of patients every year.2
CABG is sometimes accompanied by some complications and problems, especially deep visceral and continuous pains that usually continue until two days after the surgery and then will be reduced gradually. These pains can delay the recovery and cause patient dissatisfaction.3-5 In spite of the noticeable growth of technology, musculoskeletal pain has remained as one of the psycho-physical health problems because it cannot be completely relieved by medicine.6 At present, narcotic sedatives are being used to relieve the pain, but they can lead to respiratory suppression and wide and non-preventable painlessness. Although using narcotic drugs in the patients who undergo heart surgery is necessary primarily, application of large amounts of such drugs delays the recovery and also increases the length of hospital stay.7
By recognition of risky patients and prevention of the side-effects, nurses play important roles in control of pain.8 Therefore, finding new methods to deal with such challenges is necessary for these patients.9 Massage therapy is accounted to be one of the methods of complementary medicine as well as one of the oldest methods of healthcare. The origin of massage therapy has been found in old texts of ancient China as well as in Hippocrates’ writings.10 Massage therapy was considerably spread during the last two decades. Studies have shown that massage therapy alone or accompanied by other complementary treatments was beneficial in reduction of pain and psychological distress.11 Massage has been used to reduce challenges, such as pain and stress which are the causes of anxiety in hospitalized patients.12,13 Yet, contradictory results have been obtained regarding the effect of massage therapy on pain. For instance, the results of a research showed that foot massage did not have any significant effects on pain among the patients undergoing heart surgery.14 Another research, however, reported the positive effect of foot reflexive massage on the sternotomy site on the severity of pain after CABGs.15 Therefore, more studies are required to be conducted on the effect of massage therapy in the patients undergoing cardiovascular surgery.16
Up to now, several studies have emphasized the effect of massage on reduction of pain and anxiety in cardiac patients.6,16,17 However, patients’ companions did not have any roles in doing the massage in any of the previous studies. Also, no studies have been performed on the effect of massage therapy by patients’ companions on the severity of pain caused by sternotomy after CABGs. Participation of relatives in the process of care has positive effects on the length of hospital stay as well as provision of care.18 The presence of family also constitutes an important source of support for better recovery.19,20 Of course, this will be effective if relatives are adequately informed about the patients’ conditions and appropriately trained by the medical and nursing staff.21 The present study aims to determine the effect of massage therapy by patients’ companions on the severity of sternotomy site pain in the patients undergoing CABGs.
Materials and Methods
This randomized, single-blind, controlled trial was conducted on the patients hospitalized in open heart surgery wards of Nemazee and Shahid Faghihy teaching hospitals, Shiraz, Iran between November 2012 and March 2013. Considering the power of 0.8 and Altman monogram, a 70- subject sample size was determined for the study. Nevertheless, considering the probable loss during the study, 78 eligible patients were enrolled into the study and divided into two groups. Among these patients, 6 were not willing to participate in the study and 4 discontinued their participation due to severe pain and need for analgesic drugs.
Based on consultation with the patients’ physician the day before the operation, the researcher recognized if the patients met the inclusion criteria and invited them to take part in the research. The inclusion criteria of the study were being candidate for CABGs, being willing to participate in the research, being 18-70 years old, being hospitalized for at least 3 days after the operation, being oriented to time, place, and person, not having used narcotics and alcoholic drinks during the last two months, not having the history of nervous, neurovascular, psychiatric, and respiratory disturbances, and not suffering from coagulation disorders. On the other hand, the exclusion criteria of the study were reduction of level of consciousness, instability in hemodynamic status, unwillingness to continue cooperation, presence of coagulation problems (according to the natural limit of INR,PT), increase in the period of connection to pump to more than four hours, and suffering from chronic and malignant pain. The subjects were selected using convenient sampling and those who met the inclusion criteria were allocated to the intervention or control groups through block randomization. At first, the objectives of the research were explained to the patients and written informed consents were obtained. On the third day after the operation, the patients were examined by their physician and, in case of confirmation, were included in the study.
In the intervention group, one of the patients’ relatives who had active attendance at the time of hospitalization was selected and invited. The patients’ companions were then trained regarding massage therapy through face-to-face discussion, an educational CD, and practice by simulation. It should be noted that the training period varied from 60 to 90 minutes according to the companions’ learning abilities. After all, the participants’ competency in massage therapy was approved by a trained nurse. The intervention was performed when the patients were transferred from ICU to cardiac surgery ward on the third day after the operation. The patients who had severe pain and needed analgesics were excluded from the study. The study patients’ demographic characteristics were recorded in a data recording form. Thereafter, their severity of pain was assessed using McGill’s Visual Analogue Scale (VAS) whose validity and reliability have been confirmed previously. VAS is a beneficial tool to evaluate patients’ pain after surgery.22 This instrument is like a ruler numerated from zero to ten. Accordingly, scores of 1-3, 4-6, 7-9, and 10 represent mild, moderate, severe, and intolerable pain, respectively. The instruction for use of VAS was explained to the patients on the first day of hospitalization. In the intervention group, massage therapy was carried out by Thailand classic method by patients’ companions under the nurse’s supervision in a private room for 30 minutes. The procedure was carried out by soaking hands with sweet almond oil which is the most common oil applied in massage therapy23 and massage was done at back, lumber, shoulders, arms, forearms, the palm and fingers of both hands, thigh, foreleg (except for donor places), soles, insteps and fingers of feet, abdomen, and neck muscles according to the patients’ tolerance. The severity of the patients’ pain was reassessed and recorded immediately, 30 minutes, 60 minutes, and two hours after the intervention. The control group, however, received the routine care on the third day of operation and their pain scores were recorded at the same time intervals as the intervention group. Of course, the nurse and the patients’ companions were present at the patients’ bedsides for 30 minutes to provide similar conditions to the intervention group. It should be mentioned that pain was assessed by a researcher who had no information about the study groups. In addition, the ward’s routine care was performed for both groups (figure 1). The intervention group patients’ satisfaction from massage therapy was assessed using a 5-point Likert scale ranging from very low to very much.
Figure 1.
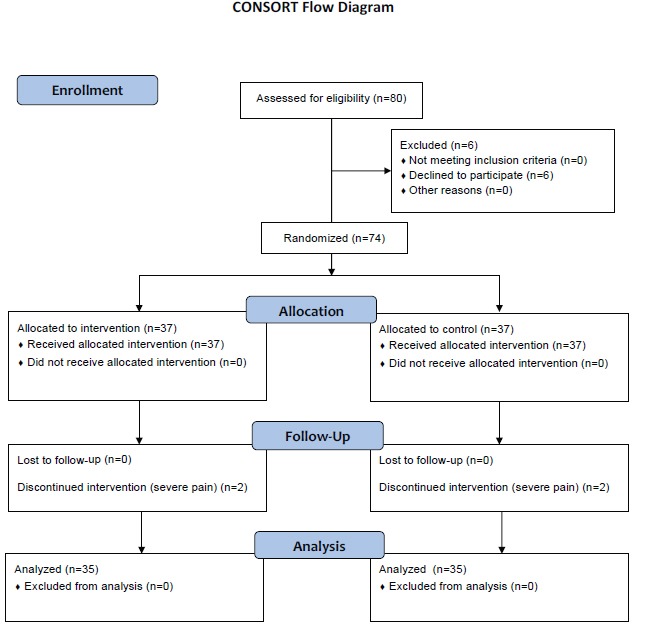
Design and protocol of the study.
After all, the data were entered into the SPSS statistical software (V. 16) and analyzed using independent t-test, paired t-test, and repeated measures Analysis of Variance (ANOVA) with schefe post hoc test. Besides, P<0.05 was considered as statistically significant.
Ethical Considerations
This study was approved by the Research Vice-chancellor and Ethics Committee of Shiraz University of Medical Sciences (Ct-6260(. All the research samples signed written informed consents and were ascertained that their individual information would remain confidential and their participating in the study was voluntary.
Results
Out of the 70 participants, 38 (54.3%) were male and 32 (45.7%) were female. The mean age of the study samples was 59.77±7.28 years and 91.4% (n=64) of them were married. The mean age of the patients in the intervention and control groups was 59.28±7.11 and 60.25±7.52 years, respectively. Most of the participants’ companions in the research (68.6%) were the patients’ children and the remaining were other relatives. At the beginning of the study, no significant difference was observed between the two groups regarding the demographic characteristics, including age, sex, level of education, and marital status (table 1). In addition, the mean and standard error of the severity of pain was 6.56±1.74 and 7.11±1.82 in the intervention and the control group, respectively, and the difference was not statistically significant. However, the results of paired t-test showed a significant reduction in the intervention group’s mean score of pain immediately, 30, 60, and 120 minutes after the intervention compared to before the intervention (P=0.001). The highest reduction in pain was observed 60 minutes after the intervention. On the other hand, no significant difference was observed between the control group’s mean scores of pain before and after the intervention. The results of repeated measures ANOVA showed that the severity of pain among the intervention group participants who received massage by their companions was significantly lower compared to the control group (P=0.001). Mean and standard deviation of pain severity in the two groups at various time intervals and the difference between the two groups have been presented in table 2.
Table 1.
Demographic characteristics of the patients in the intervention and the control group
| Variables | Characteristics | Groups | P value | |
|---|---|---|---|---|
|
Intervention
No. (%) |
Control
No. (%) |
|||
| Sex | Male | 19 (54.3) | 19 (54.3) | 0.860 |
| Female | 16 (45.7) | 16 (45.7) | ||
| Marital status | Married | 32 (91.4) | 32 (91.4) | 0.754 |
| Single or widowed | 3 (8.6) | 3 (8.6) | ||
| Level of education | Illiterate | 14 (40) | 16 (37.1) | 0.215 |
| Elementary and secondary | 20 (57.1) | 16 (37.1) | ||
| High school or above | 1 (2.9) | 3 (8.8) | ||
Table 2.
Comparison of pain intensity in the 5 time intervals in the two groups (mean±SD)
|
Groups
Period |
Before the intervention | Immediately after the intervention | 30 minutes after the intervention | 60 minutes after the intervention | 120 minutes after the intervention |
|---|---|---|---|---|---|
| intervention | 6.56±1.74 | 3.41±1.77 | 3.01±1.78 | 2.82±1.83 | 3.25±1.91 |
| Control | 7.11±1.82 | 7.07±1.81 | 7.09±1.81 | 7.13±1.71 | 7.17±1.71 |
P-Repeated measures ANOVA for main effect of intervention and time is statistically significant (P=0.001)
All the patients in the intervention group were satisfied with massage therapy; such a way that 60.0% and 40.0% of these patients described their satisfaction rate as “very much” and “much”, respectively.
Discussion
The results of this study showed that offering the patients’ companions to participate in taking care of the patient after being sufficiently trained regarding massage therapy was effective in reducing the severity of pain in post CABG patients. This finding has been supported by other researches, as well. Some studies conducted on heart surgery patients have indicated the significant effect of massage therapy on reduction of stress, anxiety, and pain.6,16,17 In another study, massage therapy was performed on 53 inpatients at medical, surgical, and obstetric wards for a period of 30 minutes in one session or more. The results showed that the intervention was effective in reduction of pain and improvement of quality of sleep, tranquility, recovery period, and healing process.24 Also, numerous studies on massage therapy in cancer patients have demonstrated its significant effects on perceived stress, quality of life, and common symptoms, such as pain, nausea, anxiety, mood disturbance, fatigue, and disturbed sleep. A large study on 1,290 patients revealed that a single massage reduced the symptoms levels by 21-52 %.25
Moreover, several studies have shown the significant effects of patients’ companions’ participation in care process on the quality of life and the related indexes in hospitalized patients.26,27 The results of two studies carried out in this area reported that massage therapy by companions as well as nurses was effective in reduction of anxiety, systolic blood pressure, heart rate, and respiratory rate among the male patients hospitalized in CCU.28,29 The results of another study indicated that doing acquainted sensory stimulations by patients’ companions during the first six days of admission of patients with brain trauma at ICU increased the level of consciousness compared to the control group.27 Also, use of organized sensory stimulation by family members led to a significant increase in the level of consciousness and cognitive behavior state in brain injured patients.30
The effect of interpersonal relationships as a contributing factor to the benefits of massage should also be considered. After experiencing a major surgery and a stressful situation in a surgical ward, patients can benefit from the attention of a family member providing support and comfort.31 The findings of the current study showed that participation of the patients’ relatives in the care process eliminated the pain, eventually increasing the patients’ and companions’ satisfaction. According to the results of the previous studies, the active support of relatives in the treatment process is highly valuable.32 In our socio-cultural context, familial relationships influence the whole dimensions of life of individuals, especially in illness and crisis.33
Furthermore, involvement of patients’ companions as family caregivers in massage therapy can lead to continuation of this effective intervention after discharging from the hospital. Of course, appropriate education and training must be considered by nurses with respect to patient safety and provision of effective care.34
Conclusion
This study revealed new information about the effectiveness of massage therapy by patients’ companions that could be observed by the nursing personnel in order to train the companions and recommend such treatments to patients. The study results showed that massage therapy could be safely and effectively delivered by the companions in cardiothoracic surgical ward, leading to significant reductions in pain and patient satisfaction. Yet, further studies are recommended to assess the effect of massage therapy on these patients’ severity of pain in longer time periods.
Acknowledgment
This manuscript was extracted from Fazlollah Rast’s M.Sc. thesis in nursing which was financially supported by the Research vice-chancellor of Shiraz University of Medical Sciences (grant No. 91-6260). The authors would like to appreciate all the nursing personnel of the heart surgery ward of Nemazee and Shahid Faghihi hospitals in Shiraz for their cooperation and all the individuals who helped in carrying out this research. They are also grateful for Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for improving the use of English in the manuscript.
Conflict of Interest: None declared.
References
- 1.Smeltzer S, Bare B. In: Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. 11th ed. Bare B, Hinkle J, et al., editors. Phildelphia: Lippincott Williams & Wilkins; 2008. [Google Scholar]
- 2.Llioyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics- 2010 update: A report from the American Heart Association. Circulation. 2010;12:e46–e215. doi: 10.1161/CIRCULATIONAHA.109.192667. [DOI] [PubMed] [Google Scholar]
- 3.Ferguson JA. Pain following coronary artery bypass grafting: an exploration of contributing actors. Intensive Crit Care Nurs. 1992;8:153–62. doi: 10.1016/0964-3397(92)90022-c. [DOI] [PubMed] [Google Scholar]
- 4.Mueller XM, Tinguely F, Tevaerai HT, et al. Pain location, distribution, and intensity after cardiac surgery. Chest. 2000;118:391–6. doi: 10.1378/chest.118.2.391. [DOI] [PubMed] [Google Scholar]
- 5.Shih FJ, Chu SH, Yu PJ, et al. Turning points of recovery from cardiac surgery during the intensive care unit transition. Heart Lung. 1997;26:99–108. doi: 10.1016/s0147-9563(97)90069-8. [DOI] [PubMed] [Google Scholar]
- 6.Kshettry VR, Carole LF, Henly SJ, et al. Complementary alternative medical therapies for heart surgery patients: feasibility, safety, and impact. Ann Thorac Surg. 2006;81:201–5. doi: 10.1016/j.athoracsur.2005.06.016. [DOI] [PubMed] [Google Scholar]
- 7.Oderda GM, Said Q, Evans RS, et al. Opioid-related adverse drug events in surgical hospitalizations: Impact on costs and length of stay. Annals of Pharmacotherapy. 2007;41:400–6. doi: 10.1345/aph.1H386. [DOI] [PubMed] [Google Scholar]
- 8.Jarzyna D, Jungquist CR, Pasero C, et al. American Society for Pain Management Nursing Guidelines on Monitoring for Opioid-Induced Sedation and Respiratory Depression. Pain Management Nursing. 2011;12:118–45. doi: 10.1016/j.pmn.2011.06.008. [DOI] [PubMed] [Google Scholar]
- 9.Wang AT, Sundt TM 3rd, Cutshall SM, Bauer BA. Massage therapy after cardiac surgery. Semin Thorac Cardiovasc Surg. 2010;22:225–9. doi: 10.1053/j.semtcvs.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 10.Noah Calvert R. The history of massage: An illustrated survey from around the world. Rochester: Healing Arts Press; 2002. [Google Scholar]
- 11.Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280:1569–75. doi: 10.1001/jama.280.18.1569. [DOI] [PubMed] [Google Scholar]
- 12.Lindsay GM, Smith LN, Hanlon P, Wheatley DJ. Coronary artery disease patients’ perception of their health and expectations of benefit following coronary artery bypass grafting. J Adv Nurs. 2000;32:1412–21. doi: 10.1046/j.1365-2648.2000.01621.x. [DOI] [PubMed] [Google Scholar]
- 13.Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Rep. 2008;12:1–23. [PubMed] [Google Scholar]
- 14.Hattan J, King L, Griffiths P. The impact of foot massage and guided relaxation following cardiac surgery: a randomized controlled trial. J Adv Nurs. 2002;37:199–207. doi: 10.1046/j.1365-2648.2002.02083.x. [DOI] [PubMed] [Google Scholar]
- 15.Sadeghi Shermeh M, Bozorgzad P, Ghafourian A, et al. Effect of foot reflexology on sternotomy pain after coronary artery bypass graft surgery. Iranian Journal of Critical Care Nursing Summer. 2009;2:51–4. [Google Scholar]
- 16.Wentworth LJ, Briese LJ, Timimi FK, et al. Massage Therapy Reduces Tension, Anxiety, and Pain in Patients Awaiting Invasive Cardiovascular Procedures. Prog Cardiovasc Nurs. 2009;24:155–61. doi: 10.1111/j.1751-7117.2009.00054.x. [DOI] [PubMed] [Google Scholar]
- 17.Cutshall SM, Wentworth LJ, Engen D, et al. Effect of massage therapy on pain, anxiety, and tension in cardiac surgical patients: a pilot study. Complement Ther Clin Pract. 2010;16:92–5. doi: 10.1016/j.ctcp.2009.10.006. [DOI] [PubMed] [Google Scholar]
- 18.Simpson T. Visitors’ verbal behavior with coronary care unit patients. West J Nurs Research. 1992;14:482–97. doi: 10.1177/019394599201400405. [DOI] [PubMed] [Google Scholar]
- 19.Locatelli F, Vecchio Del, Manzoni C. Morbidity and mortality on maintenance haemodialysis. Nephron. 1998;80:380–95. doi: 10.1159/000045210. [DOI] [PubMed] [Google Scholar]
- 20.Gurklis JA, Menke EM. Chronic haemodialysis patients’ perceptions of stress, coping, and social support. American Nephrology Nurses’ Association Journal. 1995;22:381–8. [PubMed] [Google Scholar]
- 21.Bellou P, Gerogianni KG. The contribution of family in the care of patient in the hospital. Health Science Journal. 2007;1(3) [Google Scholar]
- 22.Fabbri E, Villa G, Mabrouk M, et al. McGill pain questionnaire: A multi-dimensional verbal scale assessing postoperative changes in pain symptoms associated with severe endometriosis. J Obstet Gynaecol Res. 2009;35:753–60. doi: 10.1111/j.1447-0756.2008.00994.x. [DOI] [PubMed] [Google Scholar]
- 23.About.com, Alternative Medicine: Which Massage Oil is Best? [Internet] New York: Wong C; 2011. [cited 2013 Feb 22]. Available from: http://altmedicine.about.com/od/massage/a/massage_oil.htm. [Google Scholar]
- 24.Adams R, White B, Beckett C. The effects of massage therapy on pain management in the acute care setting. Int J Ther Massage Bodyw. 2010;3:4–11. [PMC free article] [PubMed] [Google Scholar]
- 25.Collinge W, Kahn J, Walton T, et al. Touch, Caring, and Cancer: randomized controlled trialof a multimedia caregiver education program. Support Care Cancer. 2013;21:1405–14. doi: 10.1007/s00520-012-1682-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Badiee Z, Samsamshariat Sh, Pourmorshed P. Massage Therapy by Mother or Nurse: Effect on Weight Gain in Premature Infants. J Isfahan Med School. 2011;29:804–10. [In Persian] [Google Scholar]
- 27.Hasanzadeh F, Esmaily H, Ehsaee MR, Hoseini Azizi T. The impact of familiar sensory stimulation on level of Consciousness in patients with head injury in ICU. Journal of North Khorasan University of Medical Sciences. 2012;4:121–33. [In Persian] [Google Scholar]
- 28.Adib-Hajbaghery M, Rajabi-Beheshtabad R, Abasi A, Azizi-Fini E. The Effect of Massage Therapy by a Nurse and the Patient’s Companion on the Anxiety of Male Patients Hospitalized in CCU: A Clinical Trial. Iranian Journal of Nursing. 2012;25:72–83. [Google Scholar]
- 29.Adib-Hajbaghery M, Abasi A, Rajabi-Beheshtabad R, Azizi-Fini I. The Effects of Massage Therapy by the Patient’s Relative on Vital Signs of Males Admitted in CCU. Nurs Midwifery Stud. 2012;1:16–21. [Google Scholar]
- 30.Alizade FSH, Moatary M. Comparison of the effect of organized sensory stimulation program in the nurse and family on LOC and ognition behavior state in brain injured. MSc nursing thesis. Shiraz (Iran): Shiraz University of Medical Sciences; 2001. p. 146. [Google Scholar]
- 31.Braun LA, Stanguts C, Casanelia L, et al. Massage therapy for cardiac surgery patients- a randomized trial. The Journal of Thoracic and Cardiovascular Surgery. 2012;144:1453–9. doi: 10.1016/j.jtcvs.2012.04.027. [DOI] [PubMed] [Google Scholar]
- 32.Romanowski M. Issues that Need to be Addressed in Massage Therapy. Nurs Midwifery Stud. 2012;1:109–10. [Google Scholar]
- 33.Jalali B. Iranian Families. In: McGoldrick M, Giordano J, Garcia-Preto N, editors. Ethnicity and family therapy. 3rd ed. New York: Guilford Press; 2005. pp. 451–65. [Google Scholar]
- 23.AHRQ, Agency for Healthcare Research and Quality : Hughes RG. Patient safety and quality: An evidence-based handbook for nurses. [Internet] Rockville, US: Hughes RG; 2008. [cited 2008 April 1]. Available from: http://www.ahrq.gov/legacy/qual/nurseshdbk. [PubMed] [Google Scholar]