

Abstract
Aims:
To study the demographic factors associated with alcohol dependence syndrome so that the problems of alcohol related co morbidities can be prevented with appropriate preventive measures.
Materials and Methods:
The study was conducted in De-Addiction Clinic of the Department of Psychiatry, Mamata Medical College, Khammam, Andhra Pradesh from July 2008 to February 2009. Patient who fulfills criteria for alcohol dependence, according to diagnostic and statistical manual of mental disorders, fourth edition were included.
Results:
Mean age (standard deviation) at first drink was 18.93 (3.81) years and at onset of Alcohol dependence was 28.28 (6.55) years. The most common reason being given by the patients was financial strain (70% of the patients) due to alcohol use and its consequences. Educational qualification of 12th standard or above was seen only in 7.5%. Alcohol dependence syndrome was more common in unemployed, unskilled and semi-skilled patients. Majority of patients (80%) belonged to lower socio-economic class.
Conclusion:
Alcohol dependence syndrome and its related co morbidities can be minimized to a great extent if the educational and socio-economic standards are improved in countries like India where there is increase in alcohol consumption as a life style choice.
Keywords: Alcohol, alcohol dependence syndrome, socio-economic class
INTRODUCTION
Alcohol has been consumed in India for centuries. The pattern of drinking in India has undergone a change from occasional and ritualistic use to being a social event. These developments have raised concerns about the health and the social consequences of excessive drinking leading to dependence.
In the last decade there is a rapid increase in the number of city bars and nightclubs in India and as a result an undocumented rise in alcohol abuse amongst all the sections of the society. The percentage of the drinking population aged less than 21 years has increased from 2% to more than 14% in the past 15 years, according to studies in the southern state of Kerala by Alcohol and Drugs Information Center India, a non-governmental organization. What is of particular concern and an important indicator of health risks is that the signature pattern of alcohol consumption in India is frequent and heavy drinking. More than half of all drinkers fall into the criteria for hazardous drinking, which is characterized by bingeing and solitary consumption to the point of intoxication. Moreover, spirits account for 95% of the beverages drunk in India. The present study is carried out to look for the demographic factors associated with alcohol dependence syndrome so that the problems of alcohol related co morbidities can be prevented with appropriate preventive measures.
MATERIALS AND METHODS
The study was conducted in De-Addiction Clinic of the Department of Psychiatry, Mamata Medical College and Associated Mamata General Hospital, Khammam, Andhra Pradesh during the period from July 2008 to February 2009. All the subjects fulfilling the inclusion and exclusion criteria during the study period were included in this study.
Inclusion criteria
All male subjects presenting to the De-Addiction Clinic of the Mamata General Hospital with alcohol related problems were potential candidates for this study and they are enrolled into the study if they fulfill the following inclusion criteria:
Patient of age 18 years and above
Patient who fulfills criteria for alcohol dependence, according to diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV).
Exclusion criteria
Subjects with any of the following will not be included in the study:
Concurrent presence of other Substance Dependence, according to DSM-IV, other than Nicotine
Presence of any significant illness requiring intensive medical/Surgical management.
Patients fulfilling the selection criteria were admitted after obtaining informed consent and demographic details, history, general physical examination and mental status examination were recorded on a semi-structured proforma designed for the study. The severity of alcohol dependence was assessed using addiction severity index, 5th edition. The patients were than detoxified according to the standard clinical practice.
OBSERVATIONS AND RESULTS
A total of 68 male patients were registered at the De-Addiction Clinic, at the Department of Psychiatry, MMC and Mamata General Hospital, Khammam between the period July 1st, 2008 and February 28th 2009. Whereas a total of 63 patients met the DSM-IV criteria for alcohol dependence, 7 were excluded from the study as they met criteria for another drug dependence. The remaining 56 patients were each offered admission for further management, but 16 patients refused/did not come for admission. The remaining 40 patients were subsequently included in the study. Mean age at presentation was 37.2 (±8.51) years. The aged range was between 20 and 61 years.
DISCUSSION
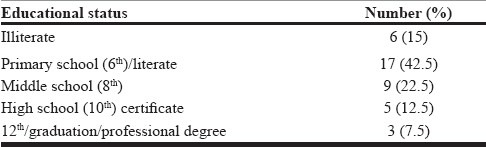
The mean age at presentation in the study was 37.2 (8.51) years. Mean age at presentation in various studies with similar design have ranged between 35 and 46 years.[1,2,3] This study found that 62% of patients were married at time of presentation [Figure 1]. In most western studies, the marital status of the patient has been most commonly found to be being separated or divorced, ranging between 43% and 60% respectively.[1,2,3,4,5,6] One large study in 2713 alcohol dependent patients however, reports higher rate of married patients than controls (57%).[7] The differences are possibly due to cultural differences. Sample in the current study came from a predominantly rural population, mostly from nuclear families. This reflects the population being catered to by the hospital where this study took place; an urban center with huge rural catchment area 32 (80%) [Table 1] patients had education less than high school level. Most of the studies have shown that most of the patients in similar clinical settings had education less than high school [Table 2].[2,3,8]
Figure 1.
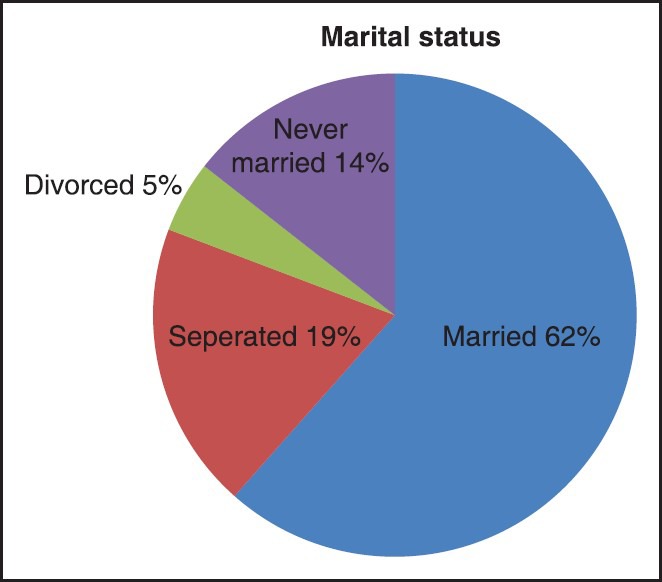
Showing the marital status of the individuals
Table 1.
Type and background of family
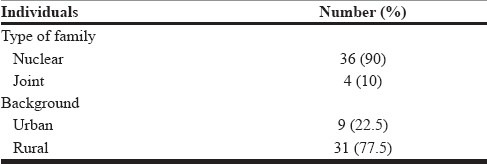
Table 2.
The educational status of the individuals
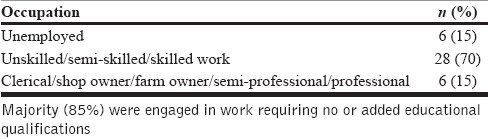
Rate for various forms of employment was 85%, involving mostly unskilled or skilled work. Previous studies have reported an equal percentage of patients who are unemployed or are gainfully employed.[2,3,6] The current study had higher rates of patients who were employed, but mostly involved in work that did not require much education and hence, comparison becomes difficult [Table 3].
Table 3.
Occupation
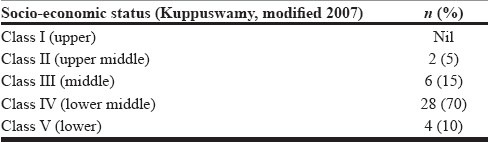
The majority of patients in the study belonged to the lower middle and middle socio-economic class. Other studies too have reported their patient population as belonging to lower middle to lower class [Table 4].[3]
Table 4.
Socio-economic
Mean age at which first drink of alcohol (in any form or amount) was taken is 18.9 years [Table 5]. The mean age at getting intoxicated by the alcohol for the first time (i.e., feeling the effects of alcohol, or taking an equivalent of 80-90 ml or more of alcohol in one setting or within a brief period of approximately 1-2 h) was 19.8 years. A study among in-patients[8] reported the mean age at first consumption to be 15.4 years and at regular consumption to be 23.1 years. The Collaborative Study of the Genetics Alcoholism (COGA) group[7] found the mean age at onset of alcoholism was 25 years [Table 5].
Table 5.
Drinking history
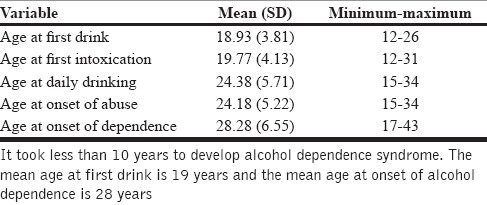
The mean age at onset Alcohol abuse was 24 years and at onset of alcohol dependence (according to DSM-IV) was 28.3 years. A study by Powell et al., had found mean age at onset of drinking was 17.3 years, while age at problem-level drinking was 30.4 years.[3] This study seems comparable to these latter studies.
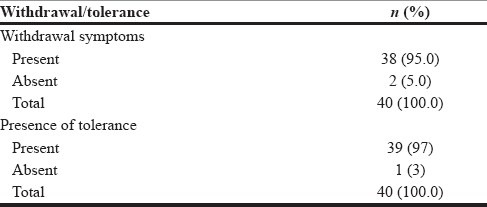
Majority of patients had presence of withdrawal symptoms (95%) and tolerance (95.5%) [Table 6]. DSM-IV indicates that diagnoses of substance dependence should be further characterized with regard to the presence of a physiological component. COGA study[7] found that such a distinction predicated more physiological complications and more alcohol-related emotional/psychiatric symptoms such as depression and anxiety. The sample in this study thus represents a higher severity across the whole group.
Table 6.
Withdrawal symptoms and tolerance
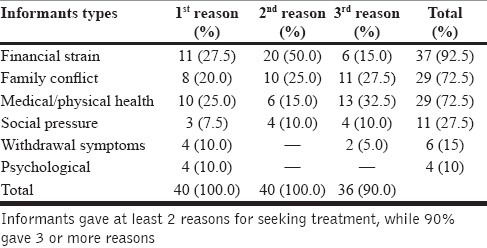
In this study, the patients and key informants were asked to enumerate reasons for seeking current treatment [Tables 7 and 8]. Based on the compilation of various reasons, these could be grouped into certain categories. On analysis, financial strain due to alcohol use was most commonly attributed for current treatment seeking by both patients (70%) and key informants (92.5%), though the patients mostly denied it as their first reason. This was followed by presence of family conflicts and concern about physical health (65% each), followed by seeking treatment due to social pressure (35%), experiencing withdrawal symptoms (25%), or psychological reasons (22.5%′ feelings of guilt, low mood, etc.). Most of the patients had more than 2 reasons for seeking treatment and this was comparable to reasons provided by the key informats. This was a unique effort in this study to incorporate such clinical parameters into the assessment, as it seems to yield similar severity status. Studies reported similarly reasons for admission to current treatment in which decision by the patient was the most common reason (73-76% of patients), while other reasons included medical condition (12%) and employer pressure (8%)[8] but stopped short of further analysis.
Table 7.
Reasons for seeking treatment
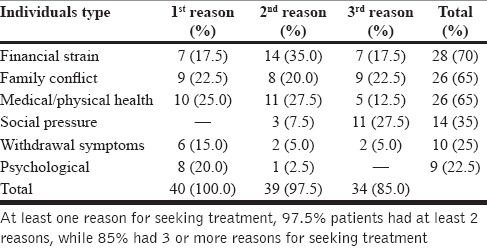
Table 8.
Informants reasons for seeking treatment
CONCLUSION
Mean age at first drink was 18.9 years and age at onset of Alcohol dependence was 28.3 years. The alcohol dependence syndrome was more common in low socio-economic class and people with education up to high school level. Measures to improve the education and socio-economic standards in the rural areas are urgently needed to control the alcohol abuse and related co morbidities.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Hesselbrock MN, Meyer RE, Keener JJ. Psychopathology in hospitalized alcoholics. Arch Gen Psychiatry. 1985;42:1050–5. doi: 10.1001/archpsyc.1985.01790340028004. [DOI] [PubMed] [Google Scholar]
- 2.Ross HE, Glaser FB, Germanson T. The prevalence of psychiatric disorders in patients with alcohol and other drug problems. Arch Gen Psychiatry. 1988;45:1023–31. doi: 10.1001/archpsyc.1988.01800350057008. [DOI] [PubMed] [Google Scholar]
- 3.Powell BJ, Penick EC, Nickel EJ, Liskow BI, Riesenmy KD, Campion SL, et al. Outcomes of co-morbid alcoholic men: A 1-year follow-up. Alcohol Clin Exp Res. 1992;16:131–8. doi: 10.1111/j.1530-0277.1992.tb00649.x. [DOI] [PubMed] [Google Scholar]
- 4.Powell BJ, Penick EC, Othmer E, Bingham SF, Rice AS. Prevalence of additional psychiatric syndromes among male alcoholics. J Clin Psychiatry. 1982;43:404–7. [PubMed] [Google Scholar]
- 5.Kranzler HR, Del Boca FK, Rounsaville BJ. Comorbid psychiatric diagnosis predicts three-year outcomes in alcoholics: A posttreatment natural history study. J Stud Alcohol. 1996;57:619–26. doi: 10.15288/jsa.1996.57.619. [DOI] [PubMed] [Google Scholar]
- 6.Schuckit MA, Tipp JE, Bucholz KK, Nurnberger JI, Jr, Hesselbrock VM, Crowe RR, et al. The life-time rates of three major mood disorders and four major anxiety disorders in alcoholics and controls. Addiction. 1997;92:1289–304. [PubMed] [Google Scholar]
- 7.Schneider U, Altmann A, Baumann M, Bernzen J, Bertz B, Bimber U, et al. Comorbid anxiety and affective disorder in alcohol-dependent patients seeking treatment: The first Multicentre Study in Germany. Alcohol Alcohol. 2001;36:219–23. doi: 10.1093/alcalc/36.3.219. [DOI] [PubMed] [Google Scholar]
- 8.Driessen M, Veltrup C, Wetterling T, John U, Dilling H. Axis I and axis II comorbidity in alcohol dependence and the two types of alcoholism. Alcohol Clin Exp Res. 1998;22:77–86. [PubMed] [Google Scholar]