

Abstract
This narrative review summarizes and integrates the available literature on PA and pain to: 1) Provide a brief overview of PA and summarize the key findings that have emerged in the study of PA and chronic pain; 2) Provide a theoretical foundation from which to understand how PA operates in the context of chronic pain; and 3) Highlight how the prevailing psychosocial treatments for chronic pain address PA in the therapeutic context, and offer suggestions for how future treatment development research can maximize the benefit of PA for patients with chronic pain. To that end, we review experimental studies that have assessed the association of evoked PA and pain sensitivity, as well as clinical studies that have assessed the association of naturally occurring PA and clinical pain in the context of chronic pain. The evidence suggests PA influences pain, over and above the influence of NA. We offer an “upward spiral” model of positive affect, resilience and pain self-management, which makes specific predictions that PA will buffer maladaptive cognitive and affective responses to pain, and promote active engagement in valued goals that enhance chronic pain self-management.
It is well established that pain is an aversive physical and emotional state. The high arousal negative affective responses to pain, such as anxiety and anger, are presumed to serve a protective function, motivating the individual to escape imminent threat (1;2). When experienced chronically, pain engenders an array of stable negative affective and behavioral styles that increase one’s vulnerability to depression and other mood disorders (3;4). The role of negative affect (NA) in chronic pain has been studied extensively and has been the topic of several reviews (5–7). Broadly, the data suggest that if psychosocial treatments for patients with chronic pain are successful in reducing NA, pain-related outcomes should improve. Research on emotions and health, however, have taught us that NA rarely influences health outcomes in isolation. Indeed, positive affect (PA) is psychometrically distinct from NA, and is associated with an array of health benefits (8), possibly owing to its reliable association with improved functioning in key biological systems, including the neuroendocrine and immune systems(9;10). PA, particularly in the past decade, has also been a target of investigation in pain research. However, to our knowledge, no review has summarized the key findings from the literature on PA and pain.
Such an undertaking is necessary, we believe, to help determine if and how therapeutic approaches targeting PA should be integrated in psychosocial treatments for chronic pain as a means for improving their efficacy. The overarching theme of current cognitive-behavioral approaches is to promote pain self-management by targeting and reducing negative affects and cognitions, but the modest effect sizes culled through decades of large and small trials (11) suggest that much of the variance in pain and pain-related outcomes remains to be addressed in treatment. Morley et al. (11) recently proposed that a paradigm shift for the treatment of pain is necessary and that, “Precise testable models are needed that link specific treatment procedures with specific psychological changes leading to hypothesized specific outcomes.” We support this clarion call, and have undertaken the present review with the goal of synthesizing the literature on PA and pain so as to better understand if and how PA enhancement strategies may be optimized in psychosocial treatments for chronic pain. Several existing psychosocial treatments for chronic pain (e.g., acceptance and commitment therapy (12); mindfulness-based stress reduction (13)) incorporate aspects of PA enhancement, and our hope is that this review will clarify which hypotheses should be tested to evaluate the efficacy of PA enhancement for patients with chronic pain.
In the present review, we: 1) Provide a brief overview of PA and summarize the key findings that have emerged in the study of PA and chronic pain; 2) Provide a theoretical foundation from which to understand how PA operates in the context of chronic pain; and 3) Highlight how the prevailing psychosocial treatments for chronic pain address PA in the therapeutic context, and offer suggestions for how future treatment development research can maximize the benefit of PA for patients with chronic pain. To this end, we searched the Google Scholar and PubMed databases for studies in which PA and pain had been experimentally manipulated, as well as studies of chronic pain in which PA was a primary measure. We employed the following search terms in various combinations: “pain,” “pain sensitivity,” “chronic pain,” or “quantitative sensory testing,” and “positive affect,” “positive mood,” or “positive emotion.” Reference sections of relevant studies were also scanned for content not identified by the original searches. Articles discussed in this review were chosen based on their relevance, in our judgment, to understanding the role of PA in chronic pain. No articles were chosen or excluded based on the direction of findings or lack of statistical significance.
The Influence of PA, Relative to NA, in the Experience of Pain
Measurement of PA
PA refers to a feeling state that may be characterized by pleasant moods or emotions that promote approach-oriented behaviors, or pleasant moods or emotions that instill a sense of relaxation, contentment, or serenity (14). PA may refer to pleasant feeling states of varying intensities and durations, ranging from mild states of contentment to overwhelmingly intense states of joy and bliss. The word “positive affect” may best be characterized as an umbrella term that encompasses “positive moods,” which are relatively stable pleasant feeling states of moderate intensity, and “positive emotions,” which are typically shorter-lived, higher intensity experiences of pleasure that represent discreet feelings.
PA is distinct from optimism (15), which is a future-oriented cognitive disposition that is associated with positive outcome expectancies. Optimism, which is most commonly measured with the Life Orientation Test-Revised (16), is reliably associated with lower pain sensitivity and adaptation to chronic pain. Readers are referred to a recent review of the association of optimism and pain for a more detailed summary (17). Although there is conceptual and psychometric overlap between optimism and PA—one who consistently expects positive outcomes may be more likely to find positive meaning and experience positive emotions in daily events—the principle distinction is that PA refers to moods and emotions, which are time-varying and may take on a variety of forms (e.g., high arousal vs. low arousal), whereas optimism refers to a cognitive style that is more stable and personality-driven. Furthermore, optimism may increase attention to negative health-related information (18), which is not a hypothesized result of experiencing PA. Consequently, increased bias toward negative health information may influence how optimism and pain are associated in certain contexts (e.g., via pain catastrophizing (19)).
“Resilience,” is another positive psychological term that should be distinguished from PA. In the chronic pain literature, resilience is typically conceptualized as the maintenance or recovery of healthful functioning through periods of physical, psychological, or social adversity (20;21). As we will discuss, PA is a factor that promotes resilience (22), but is not synonymous with resilience.
The most common method of measuring PA is through self-report. Perhaps the most ubiquitous measure, the Positive and Negative Affect Schedule (23), creates an index of PA by averaging across intensity ratings on 10 adjectives of positive valence. Elevations in PA on the PANAS generally reflect the extent to which one is activated or aroused. In addition to the PANAS, PA may been assessed by a variety of self-report instruments (for a review, see (24)). Among these, the Vigor subscale on the Profile of Mood States (POMS; (25)), which assesses high activation positive emotions, is perhaps the most similar in form and function to the PA scale on the PANAS. Other self-report methods include ratings of discreet positive emotional states, such as happiness, joy, or serenity (24). Although the majority of studies we will discuss measure PA through self-report, a variety of other assessment techniques have been investigated, including facial action coding (26), and psychophysiological recordings (27). As pain is commonly understood to be both an affective and physiological experience, it is important to note that the measurement of PA and NA in patients with chronic pain assesses one’s general emotional experience, which is likely to be influenced by ongoing pain, but may be influenced by other environmental and psychosocial inputs. Thus, PA and NA are unlikely to be perfectly correlated with pain. The residual variance in the affect-pain association forms the basis of the view that affect can be manipulated or improved through treatment, even when pain persists.
Experimental Manipulation of PA and Pain
The biopsychosocial model (28) holds that chronic pain is governed by an interacting set of endogenous (e.g., neurobiological) and exogenous (e.g., cognitive; emotional; behavioral; social) factors that sustain the subjective perception of painful somatic states. At perhaps its most basic level in humans, the influence of evoked PA on evoked or clinical pain can be demonstrated in controlled experimental studies. Indeed, numerous studies have experimentally demonstrated the benefits of induced PA on acute pain, with the general finding that PA inductions reduce pain sensitivity (See Table 1 for a selection of studies across nociceptive stimulus and affective induction modalities). Such effects have been observed in studies involving positive affective induction through the viewing of emotionally evocative images (e.g., 29;30;31;32;33;34;35;36), humorous film clips (37;38), romantic film clips (39), therapeutic suggestion (40), hypnotic suggestion (41), guided imagery (42), laughter (43), pleasant odors (44;45), pleasant music (35;46–50), and monetary reward (51). Recent work using the nociception flexion reflex design suggests that the effects of induced PA on pain may be spinally mediated (32;33;52). Neuroimaging has demonstrated that the effect of induced PA on pain is associated with activity in the anterior cingulate cortex, bilateral insula, right secondary somatosensory cortex, and left orbital frontal cortex (53). Together, these findings suggest that PA is integrated within a central pain modulatory network.
Table 1.
Examples of Experimental Studies of Induced PA and Pain in Healthy Subjects
| Nociceptive Stimulus | Affect Conditions | PA < NA | PA < Neutral | Reference |
|---|---|---|---|---|
| Cold Pressor Pain Tolerance | Positive Music vs. Negative Music vs. Auditory Distraction vs. Silence | Yes* | No | Silvestrini et al. (42) |
| Cold Pressor Pain Tolerance | IAPS Positive vs. Negative vs. Neutral affective slides | Yes* | Yes† | de Wied & Verbaten (28) |
| Cold Pressor Pain Ratings | High arousal positive vs. low arousal positive vs. Neutral affective slides | Not Assessed | Men: Yes** Women: No |
Meagher et al. (25) |
| Cold Pressor Pain Ratings | Monetary reward vs. distraction without reward vs. no distraction | Not Assessed | Yes* (but only for high catastrophizers) | Verhoeven et al. (45) |
| Tonic Thermal Pain | Pleasant Odor vs. unpleasant odor | Unpleasantness: Yes* Intensity: No |
Not Assessed | Villemure et al. (38) |
| Tonic Thermal Pain | IAPS Positive, negative, and neutral pictures paired with thermal stimuli to condition future pain response | Unpleasantness: Yes* Intensity: Yes** |
Unpleasantness: No Intensity: Yes* |
Wunsch et al. (30) |
| Tonic Thermal Pain | Pleasant music vs. unpleasant music vs. silence | Yes* (effect for both pain unpleasantness and intensity) | Yes*** (effect for both pain unpleasantness and intensity) | Roy et al. (121) |
| Tonic Thermal Pain | Pleasant Odor vs. unpleasant odor | Unpleasantness: Yes* Intensity: No (effect correlated with brain activity in anterior cingulate cortex, thalamus, and somatosensory cortices) |
Not Assessed | Villemure et al. (38) |
| Electric Shocks | IAPS Positive vs. negative vs. neutral pictures | Intensity: Yes*** Somatosensory Evoked Potentials: Yes** (effects only significant for body-related images) |
Intensity: No Somatosensory Evoked Potentials: No |
Godhino et al. (24) |
| Nociception Flexion Reflex | IAPS Positive vs. negative vs. neutral pictures | Intensity: Yes*** NFR: Yes*** |
Intensity: Yes*** NFR: Yes* |
Rhudy et al. (26) |
| Nociception Flexion Reflex | IAPS Positive (Erotic) vs. negative vs. neutral pictures | Intensity: Yes* NFR: Yes* |
Intensity: Yes* NFR: Yes* |
Rhudy et al. (27) |
| Nociception Flexion Reflex | IAPS Positive vs. negative vs. neutral pictures | Intensity: Yes* NFR: Yes* |
Intensity: Yes* NFR: No |
Roy et al. (29) |
Note. PA < NA = Pain (or otherwise specified pain-related measure) is decreased in positive affect relative to negative affect condition; PA < Neutral = Pain (or otherwise specified pain-related measure) is decreased in positive affect relative to neutral condition; IAPS = International Affective Picture System
p < .10
p < .05
p < .01
p < .001
If the effects of induced PA on induced pain are indeed mediated through central pathways of pain processing, and not simply an epiphenomenon of testing, it is reasonable to hypothesize that PA may also have similar salutary effects on the everyday experience of chronic pain in natural socio-environmental contexts. There are now several studies that have investigated the association of PA and chronic pain within a biopsychosocial framework, and much of those data stem from repeated naturalistic assessments of affect, pain, and pain-related variables in the flow of daily life. These studies indicate that PA promotes both adaptive affective responses to pain and lower chronic pain itself (54–57). But the value of microlongitudinal studies with chronic pain cohorts extends beyond the simple question of whether PA and pain are correlated. Rather, such datasets have permitted the investigation of whether PA is a unique construct in chronic pain, or simply the opposite of NA.
Time-Varying Dynamics of PA and Pain
A longstanding controversy in the emotion literature is whether PA and NA are opposite sides of a bipolar continuum (58) or separate indices in a bivariate distribution of affect with a limited degree of overlap (59;60). The former view holds that, as an affect of a particular valence moves toward one extreme of the bipolar continuum, the other affect will diminish in kind. In contrast, the bivariate view holds that, under typical conditions, PA and NA will be only modestly correlated, suggesting that day-to-day spikes in PA may occur irrespective of the level of NA. The data largely support the latter view. As displayed in Table 2, across studies that have assessed both PA and NA in patients with chronic pain, the amount of shared variance is quite modest. Among studies using the PANAS, the amount of shared variance is typically between 8–10% for between-person estimates and 2–3% for within-person estimates. Notably, variation in PA-NA correlations in chronic pain samples appears to be related to measurement type (i.e., PANAS vs. other measures) and measurement strategy (e.g., post-intervention vs. follow-up).
Table 2.
Positive and negative affect correlations across studies.
| Study | Sample | Affect Measure | Correlation r |
|---|---|---|---|
| Zautra et al. (61) | RA (N = 93) | PANAS | Within-person: −.25 Between-person: −.28 |
| Zautra, et al. (62) | RA (N=81) and OA (N = 94) | PANAS | Within-person: −.21 |
| Potter et al. (63) | RA (N = 41) | PANAS | Within-person: −.15 |
| Zautra et al. (67) | RA Sample A (N = 218) RA Sample B (N = 196) RA Sample C (N = 138) |
PANAS | Sample A: −.25 Sample B: −.22 Sample C: −.28 |
| Park & Sonty (69) | General chronic pain (N = 106) | Vitality and Mental Health subscales of SF-36 | −.38‡ |
| Seebach et al. (71) | Cervical and lumbar spinal surgery (N = 141) | PANAS | −.61 (post-op) ‡ −.40 (3 month follow-up) ‡ |
| Finan et al. (72) | Knee OA (N = 151) | Items selected from the PANAS and the POMS; separately assessed in daily diary and lab | Diary Average: −.63 Lab: −.40 |
| Strand et al. (73) | RA (N = 43) | PANAS | Within-person: −.11 Between-person −.25 |
| Smith & Zautra (77) | RA (N = 82) and OA (N = 88) | PANAS | −.12 |
| Finan et al. 2010 (84) | FM (N = 46) | PANAS | −.27‡ |
| Kranz et al. (128) | General chronic pain (N = 150) | PANAS | −.30 |
Note. Correlations are provided for studies as a function of chronic pain group and measure. Within-person correlations refer to those estimated through time-variant data. All correlations not labeled “within-person” are between-person. RA = rheumatoid arthritis; OA = osteoarthritis; FM = fibromyalgia; PANAS = Positive and Negative Affect Schedule; POMS = Profile of Mood States;
Correlation was not provided in original manuscript, and was obtained through personal communication with manuscript authors.
The correlations presented in Table 2 by and large support the notion that PA and NA are separable affective states, a key aspect of the bivariate view of affect. The distinction between the bipolar and bivariate views is not trivial. If PA always increases when NA decreases, then attenuating pain or modifying maladaptive negative cognitions should stabilize the affective system and promote well-being. This represents a ‘one size fits all’ approach to treatment: remove the negative dimension and health and well-being will improve. But if PA and NA account for unique portions of variance, a more flexible treatment approach may be warranted, with individual treatments tailored to individual affective profiles. For patients with deficits in positive affectivity, interventions aimed at augmenting PA would be crucial for restoring function and an adaptive balance of positive and negative emotions in the face of chronic pain.
Zautra and colleagues (61–63) address the distinction between PA and NA for patients with chronic pain in their Dynamic Model of Affect (DMA). The DMA proposes that neither a strict bivariate nor strict bipolar view of affect appropriately characterizes the pattern of affective states in the context of chronic pain. Because chronic pain often manifests as a continuous ebb and flow of periods of elevated, normal, and attenuated pain, affective states are likely to be dynamically influenced by changes in environmental and physiological demands, as well as random, unpredictable fluctuations. As such, under periods of relative normalcy, PA and NA are only modestly correlated. However, under conditions of adversity, which include even minor elevations in pain, PA and NA fall to the poles of the affective continuum and evidence stronger negative coupling (62). This effect has been demonstrated in several microlongitudinal studies involving patients with rheumatoid arthritis, osteoarthritis, and fibromyalgia (64–66). Furthermore, using constrained paths in a structural equation model involving pain, pain coping, and affect in a sample of patients with rheumatoid arthritis, Zautra et al.(67) demonstrated that increased PA and NA were distinct affective responses to adaptive and maladaptive chronic pain coping behaviors, respectively.
The implication of this set of findings is that micro-stressors, such as transient fluctuations in pain, narrow one’s attention, thereby diminishing emotional complexity, defined as the ability to simultaneously experience and distinguish between affects of a different valence (68). Thus, increases in pain may constrain one’s attentional focus to negatively-valenced emotional states and stimuli. Yet, individual differences in the propensity to maintain PA through elevations in pain and NA have been identified and replicated (66), and suggest that, in spite of the possibility of enhanced negative coupling under situations of duress, many patients with chronic pain have the capacity to be resilient to the challenging physiological and social changes that emerge throughout the course of illness.
More recent work has shown that PA may be uniquely involved in the development of self-efficacy to cope with chronic pain. In a series of mediation models, Park & Sonty (69) showed that PA, but not NA, was a significant mediator in the relationship of coping self-efficacy and pain interference in daily life among a group of patients with a wide range of chronic pain conditions. PA also uniquely mediated the effect of trait psychological resilience on pain catastrophizing in a sample of older adults with chronic pain (70). Individuals high in trait resilience reported less daily variation in pain catastrophizing throughout a 14-day daily diary reporting period. But that effect was fully accounted for by PA such that trait resilience predicted greater daily PA, which in turn predicted attenuated daily pain catastrophizing. Importantly, an alternative model that substituted NA for PA did not find evidence for mediation, suggesting that daily increases in PA (relative to a person’s mean over time), to a greater extent than decreases in NA, promote adaptive cognitive coping with chronic pain.
Seebach et al. (71), too, reported distinctly different effects of PA and NA in a longitudinal study of spinal surgery patients. Whereas pre-surgery PA and NA were not related to post-surgery outcomes, post-surgery PA, but not NA, significantly predicted higher postoperative functional status at 3 month follow-up. In contrast, post-surgery NA, but not PA, significantly predicted pain interference and disability at 3 month follow-up.
The amount of shared versus non-shared variance between PA and NA in the prediction of pain may depend on the temporal stability of measurement. Stable, or trait-level, affects should be most closely associated with the most salient and reliable affective stimulus in one’s immediate environment. Thus, patients with chronic pain who are reliably high in NA may be likely to report reliably high pain levels. If PA were simply the mirror image of NA, then individuals with reliably lower trait PA scores should evidence similar associations with clinical pain. A recent diary study with osteoarthritis patients suggested this is not the case. In fact, stable (i.e., trait) NA accounted for a 3-fold greater difference in average pain reports than stable PA(72). In contrast, though, state PA accounted for a greater proportion of variance in both clinical and experimental pain than state NA, demonstrating that day-to-day changes in PA are critically important to the experience of pain. Together, the results suggest that PA and NA have unique and distinguishable roles in modulating the experience of chronic pain.
PA Buffers the Harmful Effects of Pain
The general finding that PA and NA account for unique portions of variance in predicting pain and pain-related outcomes is important because it helps clarify that both PA and NA should be assessed in patients with chronic pain. But how, if at all, does PA modulate the experience of pain? Among fibromyalgia and osteoarthritis patients (n = 124), multilevel modeling showed that weekly elevations in PA above the average within-person levels buffered the effect of pain on NA such that the weekly coupling of pain and NA was attenuated when PA was high (66). Furthermore, across 11 weeks, average PA levels were significantly associated with lower clinical pain reports (66). These findings were replicated in a smaller study of rheumatoid arthritis patients (n = 43), whereby weekly elevations in PA attenuated the weekly coupling coefficient of pain and NA (73). In an experimental analog of these studies, the affective component of pain (i.e., pain unpleasantness) was reduced following a cold pressor task among women with higher, relative to lower, pre-task PA (74). Together, these studies demonstrate that PA is not merely distinct from NA, but also may blunt the otherwise sharp spikes in NA that accompany dynamic fluctuations in pain in the flow of daily life. Notably, however, a large cross-sectional study of fibromyalgia patients failed to find a buffering effect of PA on the association of pain and NA (75). This suggests that the relations between PA, NA, and pain may vary depending on the temporal dynamics of measurement (72).
PA has also been shown to buffer the effect of pain on physical function in osteoarthritis. In a large cohort study of knee osteoarthritis patients, those with high pain and high trait PA walked a significantly greater number of steps (nearly 1200) per day than patients with high pain and low PA (76). Interestingly, osteoarthritis patients with high PA walked an equivalent number of steps per day whether they had high knee pain or no knee pain at all (76).
PA is associated with prosocial behavior in chronic pain
Accummulating evidence suggests that social factors should be considered in models explicating the role of PA in chronic pain. Smith & Zautra (77) demonstrated that PA is an antecedent of positive social engagement among patients with rheumatoid arthritis and osteoarthritis. In a multi-cohort weekly diary study of patients with rheumatoid arthritis (n = 82) and osteoarthritis (n = 88), patients who reported more PA and were higher in an empirically derived psychological resilience factor reported a greater number of positive social interactions through an 11-week weekly diary than those who were lower in resilience.
PA may also arise from adaptive social engagements for patients with chronic pain. A recent study used multilevel structural equation modeling to show that daily increases in positive interpersonal events buffered the effect of daily pain on daily PA (and daily NA) in patients with fibromyalgia and osteoarthritis (78). In the same dataset, Taylor et al.(79) demonstrated that marital/partner relationship quality predicts increased PA, and that patients with a life partner exhibited more adaptive pain-related changes in PA throughout a 30-day daily diary than unpartnered patients.
Although ample evidence indicates that stressful psychosocial events decrease PA among patients with chronic pain (64), emotional disclosure of those events is associated with an increase in PA among patients with chronic pelvic pain who are high in NA (80). Such disclosure may facilitate the experience of PA by integrating stressful events within patients’ autobiographical narratives, allowing for positive reappraisal of such events (81), and promoting a sense of coherence (82) and the experience of PA. Together, this evidence suggests that PA is woven into the fabric of our social lives, bolstered by healthy relationships, and amplified by the therapeutic resolution of stressful psychosocial events. These factors, in turn, may dampen the experience of pain and buffer individuals from pain-related disability.
The Role of PA Differs Across Chronic Pain Disorders
The general finding that PA is negatively associated with pain appears to vary as a function of diagnosis. Weekly diary analyses have revealed that patients with fibromyalgia report greater daily pain and stress than age- and sex-matched patients with osteoarthritis, and that PA accounts for the greatest amount of variance in those group differences (65). Interestingly, fibromyalgia patients reported significantly lower PA, but not NA, than osteoarthritis patients across 12 weekly assessments. Furthermore, weekly (65) and daily (83) analyses show that elevations in pain result in greater reductions in PA for patients with fibromyalgia compared to osteoarthritis. Van Middendorp et al. (75) found complementary evidence in a large study comparing fibromyalgia patients and healthy controls, showing that a large PA deficit was evident even in fibromyalgia patients without comorbid medical or psychiatric disorders.
The deficient functioning of PA in fibromyalgia patients has also been observed in controlled laboratory experiments. Despite reporting improved mood while viewing positive affective images, fibromyalgia patients’ pain ratings to laser stimuli were not reduced when presented concomitantly with positive images, whereas healthy controls showed the typical linear gradient of decreased pain sensitivity with positive relative to negative stimuli (53). Rhudy et al. (52) similarly revealed that fibromyalgia patients’ pain ratings and NFR threshold were unchanged under positive relative to negative affective picture presentation, suggesting an overall damping of the processes regulating the emotional modulation of both pain and spinal nociception.
We know of only one study that has investigated biological correlates of the fibromyalgia PA deficit. Finan et al. (84) found that the loss of PA on high pain days was amplified in fibromyalgia patients with a catechol-O-methyltransferase genotype conferring low dopamine metabolism (met158met), suggesting that the association of pain and PA in fibromyalgia may be regulated by dopaminergic neurotransmission. Wood and colleagues (85–87) have demonstrated that dopaminergic neurotransmission—particularly phasic dopamine firing—is altered in fibromyalgia. As the met158met allele is associated with diminished phasic dopamine firing (88), which has in turn been shown to directly regulate the experience of PA (89;90), it is possible that the general PA deficit in FM is undergirded by a chronic impairment in dopaminergic activity.
Conceptual model for PA enhancement in chronic pain
A reasonable conclusion from the evidence presented above is that PA has a diffuse range of benefits for patients with chronic pain, and appears to operate with some degree of independence from NA. It follows that standard assessment of patient functioning should include a targeted evaluation of PA that may otherwise be missed in brief depression screeners commonly employed in clinical settings. But, to what end would clinicians seek to increase their understanding of a patient’s PA? There are currently no empirically-supported practices that aim to directly enhance PA among patients with chronic pain. The need for a targeted PA-based intervention is underscored by a growing body of evidence suggesting that patient motivation, readiness to change, and coping self-efficacy—all of which are promoted by PA (91–94)—are key factors in the long-term success of chronic pain self-management(95).
PA interventions have been developed and tested in other clinical contexts. For example, Moskowitz et al. (96) developed a PA intervention for patients with newly diagnosed HIV that exclusively focuses on techniques to enhance PA, including noticing and capitalizing on positive events, feeling gratitude, cultivating mindful awareness, positive reappraisal, focusing on personal strengths, learning to create attainable goals, and engaging in acts of kindness. Well-being therapy (97;98) utilizes CBT techniques to focus patients’ attention on positive personal attributes and environmental circumstances during daily life, and has demonstrated efficacy in patients with affective disorders. Solution-focused therapy guides patients to “search for exceptions” to psychological distress and life problems, and in so doing, enables them to identify and engage with situations, actions, and attitudes linked with the experience of well-being and positive change (99;100).
A recent adaptation of an intervention originally developed to treat addiction, Mindfulness-Oriented Recovery Enhancement (MORE)(101), unites complementary aspects of mindfulness training, cognitive reappraisal, and positive psychological principles into an integrative treatment strategy designed to disrupt the cycle of somatic distress and maladaptive cognitive-affective states common to chronic pain. MORE aims to directly stimulate PA by promoting savoring of natural rewards. Evidence from an early stage RCT involving chronic pain patients suggests that MORE may be efficacious for diminishing pain attentional bias and enhancing perceived control over pain (101). Recent findings from this preliminary trial suggest that MORE decreases pain severity and functional impairment (102), and reduces desire for opioid analgesics by enhancing autonomic responsiveness to positive emotional stimuli (102). A larger randomized clinical trial of MORE as a treatment for chronic pain is currently under way.
The potential utility of PA as a treatment target for chronic pain may be best understood within a more general conceptual framework explicating the role of PA in cognition, behavior, and health - the Broaden-and- Build Theory of Positive Emotions(103;104). Under that model, NA is thought to narrow the scope of attention and cognition(105;106) to support rapid, automatic enactment of bottom-up, habitual, defensive responses (e.g., flight, flight, freeze(107)), whereas PA exerts countervailing effects on cognition and behavior(108). Cognitive narrowing in response to negative emotions stemming from an exacerbation of chronic pain (e.g., anger, fear) may be seen as a conserved adaptation, in that it may aid in efficiently allocating resources to the critical goal of survival (i.e., escaping the source of the injury). However, when an immediate threat has passed, chronic negative emotionality can be counterproductive, fostering perseverative cognition and behavioral avoidance (109), and stress-induced health consequences, including proinflammatory and anti-immune responses that impede healing(110;111).
The Broaden-and- Build Theory plots an alternative course for affective and behavioral responses to pain. It asserts that PA reverses cognitive narrowing by facilitating individuals’ access to higher-level associations and a wider-than-usual range of ideas and sensory information. This hypothesis has been tested in an array of observational, experimental, and clinical studies which demonstrate that positive emotions result in expanded attention and enhanced problem solving(112). As a consequence of such broadened cognitive processing, PA fosters flexible responses to situational challenges (such as those presented by the need to adapt to chronic pain) by promoting exploratory and novel behaviors. In these ways, PA expands thought-action repertoires and consequently enhances the development of durable intra- and interpersonal resources, such as psychological resilience, social connectivity, and physical health(113–115). Further, PA down-regulates the effects of lingering negative affective states on stress physiology by exerting compensatory effects on sympathetic nervous system functions that, when unregulated, energize and support bodily enactment of defensive reactions (116;117). Hence, even transient increases in PA may have a sustained impact on adaptive functioning in the face of chronic pain by broadening the scope of cognition and behavior, building durable psychosocial assets, and tempering physiological stress reactivity to foster emotional, social, and physical wellbeing.
How might PA be durably enhanced in the clinical context? The three most widely researched and empirically-supported psychosocial treatments that have been adapted for chronic pain are cognitive-behavioral therapy for pain (CBT-P)(118), acceptance and commitment therapy (ACT)(119–122), and mindfulness-based stress reduction (MBSR)(123;124). Elements of these intervention strategies have been shown to engender PA and enhance health. For example, CBT-P places an emphasis on relaxation, positive reappraisal, benefit finding, and scheduling of pleasant activities (125;126). Although these therapeutic foci may promote PA, they are typically presented to patients within the general theme of minimizing negative appraisals of pain. To our knowledge, the positive psychology elements of CBT-P have not been extracted and tested against the components aimed at reducing negative cognitions and emotions. As a consequence, it is unclear if the “PA dose” of CBT-P is sufficient or could be enhanced with a more deliberate focus.
ACT places an emphasis on psychological flexibility (12;127), and promotes PA through encouraging activity engagement and goal pursuit (128). Given its roots in value-based goal pursuit, if ACT is successful, patients should feel more energetic, happier, and more vital. However, because ACT focuses on such a diverse array of contextual processes (12), such as cognitive diffusion, acceptance, and “self-as-context,” enhanced PA may be a byproduct of ACT for some patients, but not others.
MBSR emphasizes the cultivation of equanimity and present-focused awareness (129). Like ACT, patients may experience positive emotions such as calm or vigor following MBSR, but they may be just as likely to take away from the MBSR experience a primary state of nonjudgement of negative events/appraisals, which may not be correlated with positive emotional state.
Thus, a larger question remains about whether interventions like CBT, ACT, and MBSR can or should be adapted to place a primary emphasis in treatment on PA enhancement as pathway to improved chronic pain symptoms. Future investigations should determine whether interventions that aim to generate PA improve pain and pain-related outcomes via specific PA-related mechanisms, and whether effect sizes and durations are larger than can be achieved under current CBT, ACT, or MBSR formats. Such PA-related mechanisms are outlined in Figure 1, which presents a conceptual model through which positive psychological mechanisms are proposed to promote PA and resilience to chronic pain by: a) fostering mindfulness as a means of disengaging from cognitive fixation on pain and NA (130); b) broadening the scope of attention and cognition to encompass non-painful stimuli and experiences (117;118;125;131;132); c) motivating adaptive pain coping behaviors, including increased engagement in social activities and stimulating, novel experiences (95;133); d) promoting positive reappraisal of stressors, as well as reappraisal of painful stimuli and the experience of pain itself(134;135); and e) enhancing savoring (i.e., noticing enjoyment) of pleasurable objects, events, and positive emotions themselves (129). These factors may be mutually and reciprocally reinforcing, enhancing one another in an upward spiral, while diminishing the negative emotions and somatic distress inherent in chronic pain.
Figure 1. Hypothesized upward spiral model of positive affect, resilience and pain self-management.
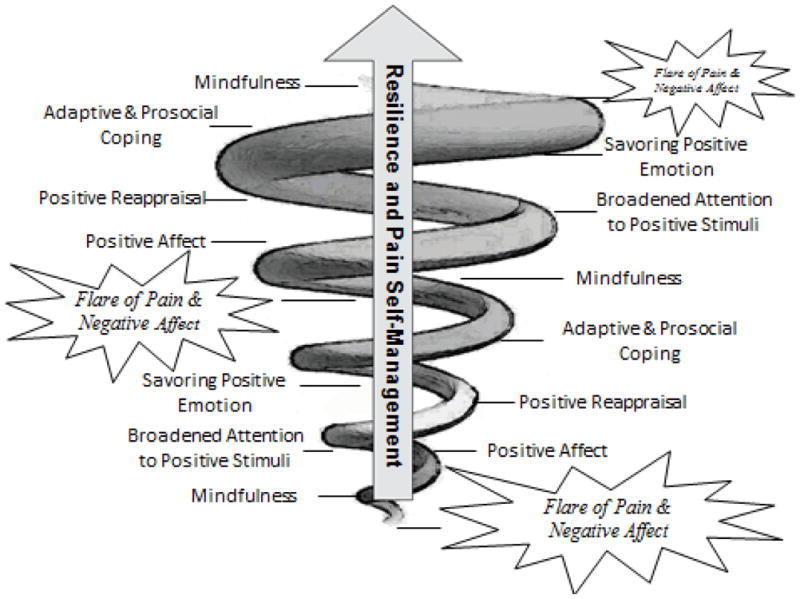
Interventions may ameliorate chronic pain and attendant negative affect (represented by progressively smaller pain and negative affect nodes as the spiral grows from bottom to top) by enhancing individual skills that promote positive affect. Such therapeutic processes may drive the upward spiral towards resilience and the ability to self-manage future pain flares by buffering individuals from the negative affective consequences of pain, decreasing pain sensitivity, and promoting prosocial behavior.
Such upward spirals have been observed in prospective observational studies in which higher initial levels of positive emotions are prospectively associated with having a more broadened mindset, which is in turn predictive of increased positive emotions in the future(131;136). Conversely, other research suggests that having a broadened mindset is prospectively associated with greater use of cognitive coping strategies that enhance PA, which are in turn predictive of having a broadened mindset(135). Moreover, such reciprocal influences have been observed in studies indicating that high levels of vagal tone, an index of flexible parasympathetic regulation of sympathetic stress reactivity, are prospectively associated with more frequent experiences of PA and enhanced prosocial connectivity(137). In turn, PA has been shown to increase vagal tone (138). Thus, PA, broadened attention and cognition, adaptive and prosocial behavior, and physiological self-regulation may be viewed as mutually-reinforcing components of upward spirals of positive affectivity. Upward spirals are evident when PA expands people’s mindsets and increases autonomic flexibility, facilitating positive reappraisals of stressful life events and promoting attention to pleasurable, rewarding, or meaningful experiences (112). By enhancing awareness of positive experiences and perspectives, PA may increase access to new contextual information with which to reappraise current circumstances and reframe them as benign, meaningful, or even beneficial.
In light of its association with enhanced regulation of attention and emotion(139), the practice of mindfulness is theorized to enhance positive reappraisal through a number of mechanisms(134;135). First, mindfulness may facilitate decentering or attentional disengagement from initial negative appraisals, which disrupts negative emotional reactions to adverse experiences and circumstances. Next, possibly by activating brain regions involved in PA (e.g., left prefrontal cortex(140)) mindfulness induces positive emotions like contentment or joy(141–143), and thereby may expand attention to encompass previously unattended sensory or semantic information. Because PA broadens the scope of cognition(132) and tunes information processing to detect stimuli that are congruent with the prevailing positive affective state (144), when mindfulness practice induces positive emotions, awareness may be selectively tuned to process positive contextual information. Positive features of the event, circumstance, or context which had been previously unnoticed now become accessible to consciousness as the “stuff” of which positive reappraisals are made. Navigating adversity through this “mindful reappraisal” process may ameliorate chronic negative emotionality, enhance self-efficacy, and promote well-being by establishing a sense of coherence and meaning in life(82).
Future studies should aim to test the components of this conceptual model through rigorous experimental and clinical research methods. Prospective designs may be employed to investigate the causal ordering of the nodes displayed in Figure 1. As evidenced in the figure, we believe that it is unlikely that pain and NA will disappear after one begins to engage in PA-enhancement strategies such as mindfulness, positive reappraisal, and savoring. Rather, the expectation is that consistent engagement in these strategies will gradually attenuate the experience of pain and NA. Because pain and NA restrict the range of attention, one may hypothesize that the attention-broadening effects of cultivated PA will increase as the experience of pain and NA diminishes over time. Future studies will need to evaluate this hypothesis at multiple levels of pain severity, as it is currently unclear if PA enhancement effects would be greater at the mild or severe end of the pain spectrum. Such hypotheses may be readily tested through ecological momentary assessment methods that capture a high volume of daily experiences (both positive and negative), and individual reactions to them (both positive and negative) in real time. Time-lagged dynamical systems modeling (145) could be used to determine if the intensity of PA accelerates with increased use of skills such as mindfulness, positive reappraisal, and savoring. Furthermore, recent advances in smartphone technology may permit interventional messaging strategies to encourage use of key positive coping skills when they are needed most.
Limitations
The present review has some limitations that deserve mention. First, it is a narrative review, and consequently does not provide a quantitative summary of data across studies. Owing to the wide variety of methods and study designs used to investigate the association of PA and pain, we did not believe a meta-analysis would have been an appropriate tool to communicate the goals of this review. Our goal was to build a theoretical model by summarizing a wide variety of research from both experimental and clinical settings that assessed acute (induced) pain and emotion as well as repeated measures of these variables over time. This approach does not permit standardized, generalizable estimates of targeted effects, which would have to be pooled across many similar studies. Second, this review does not address questions related to temporal precedence of pain and PA. To our knowledge, this issue has not been systematically investigated and should be taken up in future prospective studies to determine if pain and PA are reciprocally associated, or adhere more closely to a unidirectional relationship.
Summary and Conclusions
Substantial evidence in multiple chronic pain cohorts and in controlled experimental studies indicates that higher PA attenuates both the perception of pain and the negative affective response to pain, whereas the absence of PA exposes vulnerable (e.g., low resiliency) patients to poor pain-related outcomes. Additionally, convincing evidence indicates that PA and NA are distinct constructs, and the effects of PA on pain, and vice versa, are different from those of NA and pain. Taken together, these findings support the initiative to develop interventions that specifically target PA. Our conceptual model offers an array of therapeutic processes that promote PA, and may be tested against, or in concert with, existing therapeutic mechanisms (e.g., NA reduction strategies) to determine when and how PA versus NA-based therapeutic strategies should be deployed in the course of treatment for chronic pain. Such an effort would be responsive to recent calls for increased attention to precise, theoretically-driven hypotheses in testing psychosocial treatments for chronic pain (11). The theoretical models we have discussed in this article, and our own upward spiral model of positive affect, resilience and pain self-management coalesce around the general prediction that PA is a viable target for the treatment of chronic pain, and offer specific predictions that PA will buffer maladaptive cognitive and affective responses to pain, and promote active engagement in valued mindsets and goals that enhance chronic pain self-management.
Acknowledgments
The authors wish to acknowledge funding from NIH/NINR 1P30 NR014131 (PHF) and NIH R03DA032517 (ELG).
Contributor Information
Patrick H. Finan, Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine
Eric L. Garland, Hunstman Cancer Institute, University of Utah
Reference List
- 1.Harmon-Jones E. Anger and the behavioral approach system. Personality and Individual differences. 2003;35:995–1005. [Google Scholar]
- 2.Carver CS, Harmon-Jones E. Anger is an approach-related affect: evidence and implications. Psychol Bull. 2009;135:183. doi: 10.1037/a0013965. [DOI] [PubMed] [Google Scholar]
- 3.Geisser ME, Roth RS, Theisen ME, et al. Negative affect, self-report of depressive symptoms, and clinical depression: relation to the experience of chronic pain. The Clinical journal of pain. 2000;16:110–20. doi: 10.1097/00002508-200006000-00004. [DOI] [PubMed] [Google Scholar]
- 4.Banks SM, Kerns RD. Explaining high rates of depression in chronic pain: a diathesis-stress framework. Psychol Bull. 1996;119:95. [Google Scholar]
- 5.Janssen SA. Negative affect and sensitization to pain. Scand J Psychol. 2002;43:131–7. doi: 10.1111/1467-9450.00278. [DOI] [PubMed] [Google Scholar]
- 6.Shackman AJ, Salomons TV, Slagter HA, et al. The integration of negative affect, pain and cognitive control in the cingulate cortex. Nature Reviews Neuroscience. 2011;12:154–67. doi: 10.1038/nrn2994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wiech K, Tracey I. The influence of negative emotions on pain: behavioral effects and neural mechanisms. Neuroimage. 2009;47:987–94. doi: 10.1016/j.neuroimage.2009.05.059. [DOI] [PubMed] [Google Scholar]
- 8.Pressman SD, Cohen S. Does positive affect influence health? Psychol Bull. 2005;131:925. doi: 10.1037/0033-2909.131.6.925. [DOI] [PubMed] [Google Scholar]
- 9.Segerstrom SC, Sephton SE. Optimistic Expectancies and Cell-Mediated Immunity The Role of Positive Affect. Psychological science. 2010;21:448–55. doi: 10.1177/0956797610362061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Steptoe A, Dockray S, Wardle J. Positive affect and psychobiological processes relevant to health. J Pers. 2009;77:1747–76. doi: 10.1111/j.1467-6494.2009.00599.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Morley S, Williams A, Eccleston C. Examining the evidence of psychological treatments for chronic pain: time for a paradigm shift? Pain. 2013 doi: 10.1016/j.pain.2013.05.049. In Press. [DOI] [PubMed] [Google Scholar]
- 12.Hayes SC, Luoma JB, Bond FW, et al. Acceptance and commitment therapy: Model, processes and outcomes. Behav Res Ther. 2006;44:1–25. doi: 10.1016/j.brat.2005.06.006. [DOI] [PubMed] [Google Scholar]
- 13.Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4:33–47. doi: 10.1016/0163-8343(82)90026-3. [DOI] [PubMed] [Google Scholar]
- 14.Fredrickson BL, Cohn MA. Positive Emotions. In: Lewis M, Haviland-Jones JM, Feldman Barrett L, editors. Handbook of Emotions. 3. New York: The Guilford Press; 2008. pp. 777–96. [Google Scholar]
- 15.Chang EC, Maydeu-Olivares A, D’Zurilla TJ. Optimism and pessimism as partially independent constructs: Relationship to positive and negative affectivity and psychological well-being. Personality and Individual differences. 1997;23:433–40. [Google Scholar]
- 16.Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the Life Orientation Test. J Pers Soc Psychol. 1994;67:1063. doi: 10.1037//0022-3514.67.6.1063. [DOI] [PubMed] [Google Scholar]
- 17.Goodin BR, Bulls HW. Optimism and the Experience of Pain: Benefits of Seeing the Glass as Half Full. Current pain and headache reports. 2013;17:1–9. doi: 10.1007/s11916-013-0329-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Aspinwall LG, Brunhart SM. What I do know won’t hurt me: Optimism, attention to negative information, coping, and health. 2000 [Google Scholar]
- 19.Hood A, Pulvers K, Carrillo J, et al. Positive traits linked to less pain through lower pain catastrophizing. Personality and Individual differences. 2012;52:401–5. doi: 10.1016/j.paid.2011.10.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Karoly P, Ruehlman LS. Psychological resilience and its correlates in chronic pain: findings from a national community sample. Pain. 2006;123:90–7. doi: 10.1016/j.pain.2006.02.014. [DOI] [PubMed] [Google Scholar]
- 21.Sturgeon JA, Zautra AJ. Resilience: a new paradigm for adaptation to chronic pain. Curr Pain Headache Rep. 2010;14:105–12. doi: 10.1007/s11916-010-0095-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Fredrickson BL, Tugade MM, Waugh CE, et al. What good are positive emotions in crises? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J Pers Soc Psychol. 2003;84:365–76. doi: 10.1037//0022-3514.84.2.365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54:1063–70. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- 24.Gray EK, Watson D. Assessing positive and negative affect via self-report. In: Coan JA, Allen JB, editors. Handbook of Emotion Elicitation and Assessment. New York: Oxford University Press; 2007. pp. 171–83. [Google Scholar]
- 25.McNair DM, Lorr M, Droppleman LF. Manual: Profile of Mood States. San Diego: Educational and Industrial Testing Service; 1971. [Google Scholar]
- 26.Ekman P, Rosenberg EL. What the face reveals: Basic and applied studies of spontaneous expression using the Facial Action Coding System (FACS) Oxford University Press; 1997. [Google Scholar]
- 27.Larsen JT, Bernston GG, Poehlmann KM, et al. The psychophysiology of emotion. In: Lewis M, Haviland-Jones JM, Feldman Barrett L, editors. Handbook of Emotions. New York: The Guilford Press; 2008. pp. 180–95. [Google Scholar]
- 28.Gatchel RJ, Peng YB, Peters ML, et al. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133:581–624. doi: 10.1037/0033-2909.133.4.581. [DOI] [PubMed] [Google Scholar]
- 29.Arnold BS, Alpers GW, Suss H, et al. Affective pain modulation in fibromyalgia, somatoform pain disorder, back pain, and healthy controls. European Journal of Pain. 2008;12:329–38. doi: 10.1016/j.ejpain.2007.06.007. [DOI] [PubMed] [Google Scholar]
- 30.Godinho F, Frot M, Perchet C, et al. Pain influences hedonic assessment of visual inputs. Eur J Neurosci. 2008;27:2219–28. doi: 10.1111/j.1460-9568.2008.06196.x. [DOI] [PubMed] [Google Scholar]
- 31.Meagher MW, Arnau RC, Rhudy JL. Pain and emotion: effects of affective picture modulation. Psychosom Med. 2001;63:79–90. doi: 10.1097/00006842-200101000-00010. [DOI] [PubMed] [Google Scholar]
- 32.Rhudy JL, Williams AE, McCabe KM, et al. Affective modulation of nociception at spinal and supraspinal levels. Psychophysiology. 2005;42:579–87. doi: 10.1111/j.1469-8986.2005.00313.x. [DOI] [PubMed] [Google Scholar]
- 33.Rhudy JL, Williams AE, McCabe KM, et al. Emotional control of nociceptive reactions (ECON): do affective valence and arousal play a role? Pain. 2008;136:250–61. doi: 10.1016/j.pain.2007.06.031. [DOI] [PubMed] [Google Scholar]
- 34.de WM, Verbaten MN. Affective pictures processing, attention, and pain tolerance. Pain. 2001;90:163–72. doi: 10.1016/s0304-3959(00)00400-0. [DOI] [PubMed] [Google Scholar]
- 35.Roy M, Piche M, Chen JI, et al. Cerebral and spinal modulation of pain by emotions. Proc Natl Acad Sci U S A. 2009;106:20900–5. doi: 10.1073/pnas.0904706106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wunsch A, Philippot P, Plaghki L. Affective associative learning modifies the sensory perception of nociceptive stimuli without participant’s awareness. Pain. 2003;102:27–38. doi: 10.1016/s0304-3959(02)00331-7. [DOI] [PubMed] [Google Scholar]
- 37.Nevo O, Keinan G, Teshimovsky-Arditi M. Humor and pain tolerance. In: Kuipers G, editor. Humor. 1. De Gruyter; 1993. pp. 71–88. [Google Scholar]
- 38.Weisenberg M, Raz T, Hener T. The influence of film-induced mood on pain perception. Pain. 1998;76:365–75. doi: 10.1016/S0304-3959(98)00069-4. [DOI] [PubMed] [Google Scholar]
- 39.Zillmann D, de Wied M, King-Jablonski C, et al. Drama-induced affect and pain sensitivity. Psychosom Med. 1996;58:333–41. doi: 10.1097/00006842-199607000-00006. [DOI] [PubMed] [Google Scholar]
- 40.Zelman DC, Howland EW, Nichols SN, et al. The effects of induced mood on laboratory pain. Pain. 1991;46:105–11. doi: 10.1016/0304-3959(91)90040-5. [DOI] [PubMed] [Google Scholar]
- 41.Rainville P, Bao QVH, Christien P. Pain-related emotions modulate experimental pain perception and autonomic responses. Pain. 2005;118:306–18. doi: 10.1016/j.pain.2005.08.022. [DOI] [PubMed] [Google Scholar]
- 42.Bruehl S, Carlson CR, McCubbin JA. Two brief interventions for acute pain. Pain. 1993;54:29–36. doi: 10.1016/0304-3959(93)90096-8. [DOI] [PubMed] [Google Scholar]
- 43.Cogan R, Cogan D, Waltz W, et al. Effects of laughter and relaxation on discomfort thresholds. J Behav Med. 1987;10:139–44. doi: 10.1007/BF00846422. [DOI] [PubMed] [Google Scholar]
- 44.Villemure C, Bushnell MC. Mood influences supraspinal pain processing separately from attention. J Neurosci. 2009;29:705–15. doi: 10.1523/JNEUROSCI.3822-08.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Villemure C, Slotnick BM, Bushnell MC. Effects of odors on pain perception: deciphering the roles of emotion and attention. Pain. 2003;106:101–8. doi: 10.1016/s0304-3959(03)00297-5. [DOI] [PubMed] [Google Scholar]
- 46.Hekmat HM, Hertel JB. Pain attenuating effects of preferred versus non-preferred music interventions. Psychology of Music. 1993;21:163–73. [Google Scholar]
- 47.Roy M, Peretz I, Rainville P. Emotional valence contributes to music-induced analgesia. Pain. 2008;134:140–7. doi: 10.1016/j.pain.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 48.Silvestrini N, Piguet V, Cedraschi C, et al. Music and Auditory Distraction Reduce Pain Emotional or Attentional Effects? Music and Medicine. 2011;3:264–70. [Google Scholar]
- 49.Tang NK, Salkovskis PM, Hodges A, et al. Effects of mood on pain responses and pain tolerance: An experimental study in chronic back pain patients. Pain. 2008;138:392–401. doi: 10.1016/j.pain.2008.01.018. [DOI] [PubMed] [Google Scholar]
- 50.Roy M, Lebuis A, Hugueville L, et al. Spinal modulation of nociception by music. European Journal of Pain. 2012;16:870–7. doi: 10.1002/j.1532-2149.2011.00030.x. [DOI] [PubMed] [Google Scholar]
- 51.Verhoeven K, Crombez G, Eccleston C, et al. The role of motivation in distracting attention away from pain: an experimental study. Pain. 2010;149:229–34. doi: 10.1016/j.pain.2010.01.019. [DOI] [PubMed] [Google Scholar]
- 52.Rhudy JL, DelVentura JL, Terry EL, et al. Emotional modulation of pain and spinal nociception in fibromyalgia. Pain. 2013 doi: 10.1016/j.pain.2013.03.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kamping S, Bomba IC, Kanske P, et al. Deficient modulation of pain by a positive emotional context in fibromyalgia patients. Pain. 2013 doi: 10.1016/j.pain.2013.06.003. In Press. [DOI] [PubMed] [Google Scholar]
- 54.Connelly M, Keefe FJ, Affleck G, et al. Effects of day-to-day affect regulation on the pain experience of patients with rheumatoid arthritis. Pain. 2007;131:162–70. doi: 10.1016/j.pain.2007.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Litt MD, Shafer D, Napolitano C. Momentary mood and coping processes in TMD pain. Health Psychol. 2004;23:354. doi: 10.1037/0278-6133.23.4.354. [DOI] [PubMed] [Google Scholar]
- 56.Litt MD, Shafer DM, Ibanez CR, et al. Momentary pain and coping in temporomandibular disorder pain: exploring mechanisms of cognitive behavioral treatment for chronic pain. Pain. 2009;145:160–8. doi: 10.1016/j.pain.2009.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Strand EB, Kerns RD, Christie A, et al. Higher levels of pain readiness to change and more positive affect reduce pain reports: a weekly assessment study on arthritis patients. Pain. 2007;127:204–13. doi: 10.1016/j.pain.2006.08.015. [DOI] [PubMed] [Google Scholar]
- 58.Feldman Barrett L, Russell JA. Independence and bipolarity in the structure of current affect. J Pers Soc Psychol. 1998;74:967. [Google Scholar]
- 59.Larsen JT, McGraw AP, Cacioppo JT. Can people feel happy and sad at the same time? J Pers Soc Psychol. 2001;81:684. [PubMed] [Google Scholar]
- 60.Watson D. Intraindividual and interindividual analyses of positive and negative affect: their relation to health complaints, perceived stress, and daily activities. J Pers Soc Psychol. 1988;54:1020–30. doi: 10.1037//0022-3514.54.6.1020. [DOI] [PubMed] [Google Scholar]
- 61.Zautra AJ, Affleck GG, Tennen H, et al. Dynamic approaches to emotions and stress in everyday life: Bolger and Zuckerman reloaded with positive as well as negative affects. J Pers. 2005;73:1511–38. doi: 10.1111/j.0022-3506.2005.00357.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Zautra A, Smith B, Affleck G, et al. Examinations of chronic pain and affect relationships: Applications of a dynamic model of affect. J Consult Clin Psychol. 2001;69:786. doi: 10.1037//0022-006x.69.5.786. [DOI] [PubMed] [Google Scholar]
- 63.Potter PT, Zautra AJ, Reich JW. Stressful events and information processing dispositions moderate the relationship between positive and negative affect: Implications for pain patients. Ann Behav Med. 2000;22:191–8. doi: 10.1007/BF02895113. [DOI] [PubMed] [Google Scholar]
- 64.Davis MC, Zautra AJ, Smith BW. Chronic pain, stress, and the dynamics of affective differentiation. J Pers. 2004;72:1133–59. doi: 10.1111/j.1467-6494.2004.00293.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Zautra AJ, Fasman R, Reich JW, et al. Fibromyalgia: evidence for deficits in positive affect regulation. Psychosom Med. 2005;67:147–55. doi: 10.1097/01.psy.0000146328.52009.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Zautra AJ, Johnson LM, Davis MC. Positive affect as a source of resilience for women in chronic pain. J Consult Clin Psychol. 2005;73:212–20. doi: 10.1037/0022-006X.73.2.212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Zautra AJ, Burleson MH, Smith CA, et al. Arthritis and perceptions of quality of life: an examination of positive and negative affect in rheumatoid arthritis patients. Health Psychol. 1995;14:399. doi: 10.1037//0278-6133.14.5.399. [DOI] [PubMed] [Google Scholar]
- 68.Salovey P, Mayer JD. Emotional intelligence. Imagination, cognition and personality. 1989;9:185–211. [Google Scholar]
- 69.Park SH, Sonty N. Positive affect mediates the relationship between pain-related coping efficacy and interference in social functioning. The Journal of Pain. 2010;11:1267–73. doi: 10.1016/j.jpain.2010.02.023. [DOI] [PubMed] [Google Scholar]
- 70.Ong AD, Bergeman CS, Bisconti TL, et al. Psychological resilience, positive emotions, and successful adaptation to stress in later life. J Pers Soc Psychol. 2006;91:730. doi: 10.1037/0022-3514.91.4.730. [DOI] [PubMed] [Google Scholar]
- 71.Seebach CL, Kirkhart M, Lating JM, et al. Examining the role of positive and negative affect in recovery from spine surgery. Pain. 2012;153:518–25. doi: 10.1016/j.pain.2011.10.012. [DOI] [PubMed] [Google Scholar]
- 72.Finan PH, Quartana PJ, Smith MT. Positive and Negative Affect Dimensions in Chronic Knee Osteoarthritis: Effects on Clinical and Laboratory Pain. Psychosom Med. 2013;75:463–70. doi: 10.1097/PSY.0b013e31828ef1d6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Strand EB, Zautra AJ, Thoresen M, et al. Positive affect as a factor of resilience in the pain-negative affect relationship in patients with rheumatoid arthritis. J Psychosom Res. 2006;60:477–84. doi: 10.1016/j.jpsychores.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 74.Ruiz-Aranda D, Salguero JMn, Fernández-Berrocal P. Emotional regulation and acute pain perception in women. The Journal of Pain. 2010;11:564–9. doi: 10.1016/j.jpain.2009.09.011. [DOI] [PubMed] [Google Scholar]
- 75.van Middendorp H, Lumley MA, Jacobs JW, et al. Emotions and emotional approach and avoidance strategies in fibromyalgia. J Psychosom Res. 2008;64:159–67. doi: 10.1016/j.jpsychores.2007.08.009. [DOI] [PubMed] [Google Scholar]
- 76.White DK, Keysor JJ, Neogi T, et al. When it hurts, a positive attitude may help: association of positive affect with daily walking in knee osteoarthritis. Results from a multicenter longitudinal cohort study. Arthritis Care & Research. 2012;64:1312–9. doi: 10.1002/acr.21694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Smith BW, Zautra AJ. Vulnerability and resilience in women with arthritis: test of a two-factor model. J Consult Clin Psychol. 2008;76:799–810. doi: 10.1037/0022-006X.76.5.799. [DOI] [PubMed] [Google Scholar]
- 78.Sturgeon JA, Zautra AJ, Arewasikporn A. A multilevel structural equation modeling analysis of vulnerabilities and resilience resources influencing affective adaptation to chronic pain. PAIN. 2013 doi: 10.1016/j.pain.2013.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Taylor SS, Davis MC, Zautra AJ. Relationship status and quality moderate daily pain-related changes in physical disability, affect, and cognitions in women with chronic pain. Pain. 2012 doi: 10.1016/j.pain.2012.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Norman SA, Lumley MA, Dooley JA, et al. For whom does it work? Moderators of the effects of written emotional disclosure in a randomized trial among women with chronic pelvic pain. Psychosom Med. 2004;66:174–83. doi: 10.1097/01.psy.0000116979.77753.74. [DOI] [PubMed] [Google Scholar]
- 81.Lazarus RS, Folkman S. Stress, appraisal, and coping. Springer Publishing Company; 1984. [Google Scholar]
- 82.Antonovsky A. Unraveling the mystery of health: How people manage stress and stay well. Jossey-Bass; 1987. [Google Scholar]
- 83.Finan PH, Zautra AJ, Davis MC. Daily affect relations in fibromyalgia patients reveal positive affective disturbance. Psychosom Med. 2009;71:474–82. doi: 10.1097/PSY.0b013e31819e0a8b. [DOI] [PubMed] [Google Scholar]
- 84.Finan PH, Zautra AJ, Davis MC, et al. Genetic influences on the dynamics of pain and affect in fibromyalgia. Health Psychol. 2010;29:134–42. doi: 10.1037/a0018647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Wood PB, Schweinhardt P, Jaeger E, et al. Fibromyalgia patients show an abnormal dopamine response to pain. Eur J Neurosci. 2007;25:3576–82. doi: 10.1111/j.1460-9568.2007.05623.x. [DOI] [PubMed] [Google Scholar]
- 86.Wood PB. Role of central dopamine in pain and analgesia. Expert Rev Neurother. 2008;8:781–97. doi: 10.1586/14737175.8.5.781. [DOI] [PubMed] [Google Scholar]
- 87.Wood PB, Glabus MF, Simpson R. Changes in gray matter density in fibromyalgia: correlation with dopamine metabolism. The Journal of Pain. 2009;10:609–18. doi: 10.1016/j.jpain.2008.12.008. [DOI] [PubMed] [Google Scholar]
- 88.Bilder RM, Volavka J, Lachman HM, et al. The catechol-O-methyltransferase polymorphism: relations to the tonic-phasic dopamine hypothesis and neuropsychiatric phenotypes. Neuropsychopharmacology. 2004 doi: 10.1038/sj.npp.1300542. [DOI] [PubMed] [Google Scholar]
- 89.Ashby FG, Isen AM, Turken AU. A neuropsychological theory of positive affect and its influence on cognition. Psychol Rev. 1999;106:529–50. doi: 10.1037/0033-295x.106.3.529. [DOI] [PubMed] [Google Scholar]
- 90.Schultz W. Getting formal with dopamine and reward. Neuron. 2002;36:241–63. doi: 10.1016/s0896-6273(02)00967-4. [DOI] [PubMed] [Google Scholar]
- 91.Elliot AJ, Thrash TM. Approach-avoidance motivation in personality: approach and avoidance temperaments and goals. J Pers Soc Psychol. 2002;82:804. doi: 10.1037//0022-3514.82.5.804. [DOI] [PubMed] [Google Scholar]
- 92.Erez A, Isen AM. The influence of positive affect on the components of expectancy motivation. J Appl Psychol. 2002;87:1055. doi: 10.1037/0021-9010.87.6.1055. [DOI] [PubMed] [Google Scholar]
- 93.Lyubomirsky S. Why are some people happier than others? The role of cognitive and motivational processes in well-being. Am Psychol. 2001;56:239. [PubMed] [Google Scholar]
- 94.Lyubomirsky S, King L, Diener E. The benefits of frequent positive affect: does happiness lead to success? Psychol Bull. 2005;131:803–55. doi: 10.1037/0033-2909.131.6.803. [DOI] [PubMed] [Google Scholar]
- 95.Jensen MP, Nielson WR, Kerns RD. Toward the development of a motivational model of pain self-management. J Pain. 2003;4:477–92. doi: 10.1016/s1526-5900(03)00779-x. [DOI] [PubMed] [Google Scholar]
- 96.Moskowitz JT, Hult JR, Duncan LG, et al. A Positive Affect Intervention for People Experiencing Health-Related Stress:Development and non-Randomized Pilot Test. J Health Psychol. 2011 doi: 10.1177/1359105311425275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Fava GA, Ruini C. Development and characteristics of a well-being enhancing psychotherapeutic strategy: well-being therapy. J Behav Ther Exp Psychiatry. 2003;34:45–63. doi: 10.1016/s0005-7916(03)00019-3. [DOI] [PubMed] [Google Scholar]
- 98.Fava GA, Tomba E. Increasing Psychological Well–Being and Resilience by Psychotherapeutic Methods. J Pers. 2009;77:1903–34. doi: 10.1111/j.1467-6494.2009.00604.x. [DOI] [PubMed] [Google Scholar]
- 99.De Shazer S. Clues: Investigating solutions in brief therapy. WW Norton & Co; 1988. [Google Scholar]
- 100.Fitzpatrick MR, Stalikas A. Positive emotions as generators of therapeutic change. Journal of Psychotherapy Integration. 2008;18:137. [Google Scholar]
- 101.Garland EL, Howland EW. Mindfulness-Oriented Recovery Enhancement reduces pain attentional bias in chronic pain patients. Psychother Psychosom. 2013 doi: 10.1159/000348868. [DOI] [PubMed] [Google Scholar]
- 102.Garland E, Manusov EG, Froeliger B, et al. Mindfulness-oriented recovery enhancement for chronic pain and prescription opioid misuse: Results from an early stage randomized controlled trial. J Consult Clin Psychol. 2014 doi: 10.1037/a0035798. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Fredrickson BL. What good are positive emotions? Review of general psychology. 1998;2:300. doi: 10.1037/1089-2680.2.3.300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Fredrickson BL. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am Psychol. 2001;56:218. doi: 10.1037//0003-066x.56.3.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Schmitz TW, De Rosa E, Anderson AK. Opposing influences of affective state valence on visual cortical encoding. The Journal of neuroscience. 2009;29:7199–207. doi: 10.1523/JNEUROSCI.5387-08.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Talarico JM, LaBar KS, Rubin DC. Emotional intensity predicts autobiographical memory experience. Memory & Cognition. 2004;32:1118–32. doi: 10.3758/bf03196886. [DOI] [PubMed] [Google Scholar]
- 107.Frijda NH. The laws of emotion. Am Psychol. 1988;43:349. doi: 10.1037//0003-066x.43.5.349. [DOI] [PubMed] [Google Scholar]
- 108.Talarico JM, Berntsen D, Rubin DC. Positive emotions enhance recall of peripheral details. Cognition and Emotion. 2009;23:380–98. doi: 10.1080/02699930801993999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Edwards RR, Cahalan C, Mensing G, et al. Pain, catastrophizing, and depression in the rheumatic diseases. Nature Reviews Rheumatology. 2011;7:216–24. doi: 10.1038/nrrheum.2011.2. [DOI] [PubMed] [Google Scholar]
- 110.Brosschot JF, Gerin W, Thayer JF. The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. J Psychosom Res. 2006;60:113–24. doi: 10.1016/j.jpsychores.2005.06.074. [DOI] [PubMed] [Google Scholar]
- 111.Thayer JF, Brosschot JF. Psychosomatics and psychopathology: looking up and down from the brain. Psychoneuroendocrinology. 2005;30:1050–8. doi: 10.1016/j.psyneuen.2005.04.014. [DOI] [PubMed] [Google Scholar]
- 112.Garland EL, Fredrickson B, Kring AM, et al. Upward spirals of positive emotions counter downward spirals of negativity: Insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clin Psychol Rev. 2010;30:849–64. doi: 10.1016/j.cpr.2010.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Cohn MA, Fredrickson BL, Brown SL, et al. Happiness unpacked: positive emotions increase life satisfaction by building resilience. Emotion. 2009;9:361. doi: 10.1037/a0015952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Fredrickson BL, Cohn MA, Coffey KA, et al. Open hearts build lives: positive emotions, induced through loving-kindness meditation, build consequential personal resources. J Pers Soc Psychol. 2008;95:1045. doi: 10.1037/a0013262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Waugh CE, Fredrickson BL. Nice to know you: Positive emotions, self–other overlap, and complex understanding in the formation of a new relationship. The Journal of Positive Psychology. 2006;1:93–106. doi: 10.1080/17439760500510569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Fredrickson L, Levenson RW. Positive emotions speed recovery from the cardiovascular sequelae of negative emotions. Cognition & Emotion. 1998;12:191–220. doi: 10.1080/026999398379718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Fredrickson BL, Mancuso RA, Branigan C, et al. The undoing effect of positive emotions. Motivation and Emotion. 2000;24:237–58. doi: 10.1023/a:1010796329158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80:1–13. doi: 10.1016/s0304-3959(98)00255-3. [DOI] [PubMed] [Google Scholar]
- 119.Dahl J, Wilson KG, Nilsson A. Acceptance and commitment therapy and the treatment of persons at risk for long-term disability resulting from stress and pain symptoms: A preliminary randomized trial. Behavior therapy. 2004;35:785–801. [Google Scholar]
- 120.McCracken LM, Sato A, Taylor GJ. A Trial of a Brief Group-Based Form of Acceptance and Commitment Therapy (ACT) for Chronic Pain in General Practice: Pilot Outcome and Process Results. The Journal of Pain. 2013 doi: 10.1016/j.jpain.2013.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Wicksell RK, Kemani M, Jensen K, et al. Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial. European Journal of Pain. 2012 doi: 10.1002/j.1532-2149.2012.00224.x. [DOI] [PubMed] [Google Scholar]
- 122.Wetherell JL, Afari N, Rutledge T, et al. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain. 2011;152:2098–107. doi: 10.1016/j.pain.2011.05.016. [DOI] [PubMed] [Google Scholar]
- 123.Grossman P, Tiefenthaler-Gilmer U, Raysz A, et al. Mindfulness training as an intervention for fibromyalgia: evidence of postintervention and 3-year follow-up benefits in well-being. Psychother Psychosom. 2007;76:226–33. doi: 10.1159/000101501. [DOI] [PubMed] [Google Scholar]
- 124.Pradhan EK, Baumgarten M, Langenberg P, et al. Effect of Mindfulness–Based stress reduction in rheumatoid arthritis patients. Arthritis Care & Research. 2007;57:1134–42. doi: 10.1002/art.23010. [DOI] [PubMed] [Google Scholar]
- 125.MacPhillamy DJ, Lewinsohn PM. The pleasant events schedule: Studies on reliability, validity, and scale intercorrelation. J Consult Clin Psychol. 1982;50:363. [Google Scholar]
- 126.Tennen H, Affleck G. Benefit-finding and benefit-reminding. In: Snyder CR, Lopez SJ, editors. Handbook of Positive Psychology. New York: Oxford University Press; 2002. pp. 584–97. [Google Scholar]
- 127.Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010;30:865–78. doi: 10.1016/j.cpr.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Kranz D, Bollinger A, Nilges P. Chronic pain acceptance and affective well–being: A coping perspective. European Journal of Pain. 2010;14:1021–5. doi: 10.1016/j.ejpain.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 129.Jose PE, Lim BT, Bryant FB. Does savoring increase happiness? A daily diary study. The Journal of Positive Psychology. 2012;7:176–87. [Google Scholar]
- 130.Hamilton NA, Kitzman H, Guyotte S. Enhancing health and emotion: Mindfulness as a missing link between cognitive therapy and positive psychology. Journal of Cognitive Psychotherapy. 2006;20:123–34. [Google Scholar]
- 131.Fredrickson BL, Joiner T. Positive emotions trigger upward spirals toward emotional well-being. Psychological science. 2002;13:172–5. doi: 10.1111/1467-9280.00431. [DOI] [PubMed] [Google Scholar]
- 132.Fredrickson BL, Branigan C. Positive emotions broaden the scope of attention and thought-action repertoires. Cognition & Emotion. 2005;19:313–32. doi: 10.1080/02699930441000238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Jensen MP, Nielson WR, Turner JA, et al. Readiness to self-manage pain is associated with coping and with psychological and physical functioning among patients with chronic pain. Pain. 2003;104:529–37. doi: 10.1016/S0304-3959(03)00092-7. [DOI] [PubMed] [Google Scholar]
- 134.Garland E, Gaylord S, Park J. The role of mindfulness in positive reappraisal. Explore: The Journal of Science and Healing. 2009;5:37–44. doi: 10.1016/j.explore.2008.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Garland EL, Gaylord SA, Fredrickson BL. Positive reappraisal mediates the stress-reductive effects of mindfulness: An upward spiral process. Mindfulness. 2011;2:59–67. [Google Scholar]
- 136.Burns AB, Brown JS, Sachs-Ericsson N, et al. Upward spirals of positive emotion and coping: Replication, extension, and initial exploration of neurochemical substrates. Personality and Individual differences. 2008;44:360–70. doi: 10.1016/j.paid.2007.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Kok BE, Fredrickson BL. Upward spirals of the heart: Autonomic flexibility, as indexed by vagal tone, reciprocally and prospectively predicts positive emotions and social connectedness. Biol Psychol. 2010;85:432–6. doi: 10.1016/j.biopsycho.2010.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Kok BE, Coffey KA, Cohn MA, et al. How Positive Emotions Build Physical Health Perceived Positive Social Connections Account for the Upward Spiral Between Positive Emotions and Vagal Tone. Psychological science. 2013 doi: 10.1177/0956797612470827. [DOI] [PubMed] [Google Scholar]
- 139.Holzel BK, Lazar SW, Gard T, et al. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science. 2011;6:537–59. doi: 10.1177/1745691611419671. [DOI] [PubMed] [Google Scholar]
- 140.Davidson RJ. What does the prefrontal cortex “do” in affect: perspectives on frontal EEG asymmetry research. Biol Psychol. 2004;67:219–34. doi: 10.1016/j.biopsycho.2004.03.008. [DOI] [PubMed] [Google Scholar]
- 141.Geschwind N, Peeters F, Drukker M, et al. Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression: a randomized controlled trial. J Consult Clin Psychol. 2011;79:618. doi: 10.1037/a0024595. [DOI] [PubMed] [Google Scholar]
- 142.Jislin-Goldberg T, Tanay G, Bernstein A. Mindfulness and positive affect: cross-sectional, prospective intervention, and real-time relations. The Journal of Positive Psychology. 2012;7:349–61. [Google Scholar]
- 143.Schroevers MJ, Brandsma R. Is learning mindfulness associated with improved affect after mindfulness–based cognitive therapy? Br J Psychol. 2010;101:95–107. doi: 10.1348/000712609X424195. [DOI] [PubMed] [Google Scholar]
- 144.Friedman RS, Forster J. Implicit affective cues and attentional tuning: an integrative review. Psychol Bull. 2010;136:875. doi: 10.1037/a0020495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Butner J, Amazeen PG, Mulvey GM. Multilevel modeling of two cyclical processes: extending differential structural equation modeling to nonlinear coupled systems. Psychological methods. 2005;10:159. doi: 10.1037/1082-989X.10.2.159. [DOI] [PubMed] [Google Scholar]