

Abstract
Cyanoacrylate injection is a recognised endoscopic treatment option for variceal haemorrhage. We describe a 34-year old man with hepatitis B cirrhosis who presented to the hospital with upper gastrointestinal haemorrhage from gastric and oesophageal varices. Haemostasis was achieved via cyanoacrylate injection sclerotherapy and banding. Ten days later, the patient developed acute hypoxia and fever. His chest radiograph showed wide-spread pulmonary shadowing. A non-contrast CT scan confirmed multiple emboli of injected glue material from the varix with parenchymal changes either suggesting acute lung injury or pulmonary oedema. He gradually recovered with supportive treatment and was discharged home. On follow-up, he remained asymptomatic from a chest perspective. This case report discusses the rare complication of pulmonary embolisation of cyanoacrylate glue from variceal injection sites and the diagnostic dilemmas involved. Emphasis is placed on the importance of maintaining high index of clinical suspicion when assessing patients with possible procedure related complications.
Background
Acute upper gastrointestinal (GI) bleeding is the most common GI emergency and accounts for 9000 deaths in the UK each year.1 Variceal bleeding accounts for 11% of acute upper GI bleeding and continues to be rising as a consequence of excess alcohol consumption in this country.1 In the 2007 UK audit, gastro-oesophageal varices was found in 20% of new admissions in the underage 60 group.1 Endoscopic haemostatic techniques have continued to develop over the years. However, variceal obturation with cyanoacrylate glue remains an effective treatment option albeit with the acknowledged risk of distal embolisation. Our case illustrates an atypical delayed presentation of pulmonary embolic complications in a ventilated patient who received large volume of cyanoacrylate injection for a bleeding gastric varix in a critical care setting. To the best of our knowledge, this is the fifth reported case in the UK2–5 and first report of such delayed onset glue embolism.
Case presentation
A 34-year-old man with hepatitis B cirrhosis presented to the emergency department with lethargy and multiple episodes of haematemesis. On arrival, he was hypotensive, tachycardic, icteric and encephalopathic. Physical examination revealed a distended abdomen with ascites and no other findings. His blood tests showed the following: haemoglobin 50 g/L, white cell count 25.7×109/L, prothrombin time 26.9 s, albumin 11 g/L, bilirubin 46 µml/L, alkaline phosphatase 357 µ/L, alanine transaminase 134 µ/L, urea 8.0 mmol/L and creatinine 197 µmol/L. His Child-Pugh score was C. He was transfused with packed red cells, fresh frozen plasma and cryoprecipitate and was transferred to the intensive care unit where he was subsequently intubated, ventilated and started on terlipressin. His upper GI endoscopy revealed several oesophageal varices, a blood-filled stomach and limited views of a fundal gastric varix. He received banding ligation to his oesophageal varices and haemostasis was achieved. The following day, he underwent a further endoscopy and received cyanoacrylate injection to the large gastric varix. In total, 4 mLs of cyanoacrylate glue mix (1:1 with lipiodol) was injected into two sites in the varix. The patient was haemodynamically stable postprocedure. He remained intubated and ventilated due to severe hepatic encephalopathy and received continuous veno-venous haemofiltration for severe acute kidney injury.
On day 10 of his admission, he developed a fever of 38.9°C, desaturated from 98% to 94% and became tachycardic. His oxygen requirements increased from a FiO2 of 0.4 to 0.7. On examination, he was found to have blood stained secretions in his tracheostomy tube and ventilatory circuit. There were wide-spread fine crepitations audible throughout his chest. A chest radiograph showed diffuse, bilateral opacity. A non-contrast CT scan showed diffuse bilateral ground glass changes and consolidation throughout the lower lobes. Linear hyper-densities were present within the pulmonary arteries and their branches with larger volume, tubular high densities within the distribution of infradiaphragmatic varices (figure 1A–C). These findings were in keeping with multiple emboli from the injected material in the varix with parenchymal changes suggesting either pulmonary oedema or acute lung injury. The patient was managed conservatively with intravenous diuretics. He was empirically started on broad-spectrum antibiotics for possible ventilator-associated pneumonia. Bronchoscopy with bronchoalveolar lavage showed frothy pink sputum in the airways and ruled out any clear source of haemorrhage. Echocardiogram showed normal left ventricular function and no cardiac abnormalities.
Figure 1.
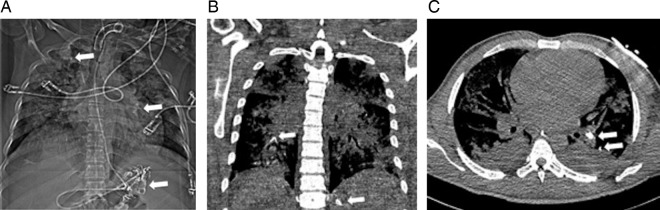
(A) Non-contrast CT (scout view). Diffuse, bilateral consolidation and white arrows indicate small areas of high density projected over left hilum and right apex, with a larger quantity of serpiginous, high-density material distributed in the left upper quadrant. (B and C) Selected non-contrast CT images (coronal and axial slices respectively). White arrows show small, linear hyperdensities distributed within central and pulmonary arterial branches, and infradiaphragmatic varices.
Outcome and follow-up
Over the next 4–5 days, his oxygen requirements decreased. A repeat chest radiograph showed resolution of the parenchymal changes. He was successfully weaned off the ventilator and was extubated. Prior to discharge home, his surveillance endoscopy showed ulceration from sclerotherapy and no further bleeding. During his outpatient follow-up, he remained asymptomatic from a chest point of view.
Discussion
The guidelines published by the British Gastroenterology Society in 2001 recommend band ligation as first line treatment for gastro-oesophageal varices. However, in difficult banding or uncontrolled bleeding, other treatment options such as endoscopic sclerotherapy, tissue adhesives or transjugular intrahepatic portosystemic shunt (TIPSS) can be considered.6 The recent guidelines by the Scottish Intercollegiate Guidelines Network in 2008,7 the report from the Baveno V consensus workshop in 2010,8 and the National Institute for Health and Care Excellence guidelines in 20129 recommend that in patients with confirmed gastric variceal haemorrhage to have endoscopic treatment preferably with cyanoacrylate injection. Studies have suggested that cyanoacrylate injection is more cost- effective than TIPSS.10 11
N-butyl-cyanoacrylate is a watery solution that polymerises almost immediately on contact with blood, thus securing a rapid haemostasis. It is mixed with lipiodol, an oil base agent to delay polymerisation in order to minimise adherence to injecting needles and endoscopes but at the risk of distal embolisation that are potentially catastrophic.12 The embolic adverse effects reported so far include pulmonary embolism, splenic infarction, splenic vein and portal vein thrombosis and recurrent sepsis caused by glue emboli acting as a septic source.2–5 13–28 Other more common risks associated with cyanoacrylate injection treatment include transient fever and pain, early rebleeding due to necrosis around the injection site, incomplete varix obliteration, tissue necrosis leading to deep ulceration and occasional perforation.12 In our case, pulmonary embolism was observed and this is our focus of discussion.
The pathophysiology of glue migration can be complex. Most gastric varices receive blood supply from short gastric and epiploic veins which drains to the left renal vein via a large gastrorenal shunt.21 Injected cyanoacrylate can migrate from the gastric varices via the gastrorenal and splenorenal veins into the inferior vena cava, right heart and pulmonary circulation. The lungs act as a filter to most emboli, however, systemic embolisation to the spleen, cerebral and coronary arteries can occur through arteriovenous pulmonary shunt or paradoxical embolisation via patent foramen ovale or atrial septal defect.21 An alternative migration pathway is via the superior vena cava and the azygos vein but Depuey et al proposed that this occurs more commonly with oesophageal than cardial or gastric varices.20 In the case reported here, it is difficult to have complete diagnostic certainty when it comes to predicting the pathway of glue migration which resulted in the multiple pulmonary emboli; however from figure 2, it is likely that cyanoacrylate travelled through a gastrorenal shunt as embolic material can be seen in splenorenal varices.
Figure 2.
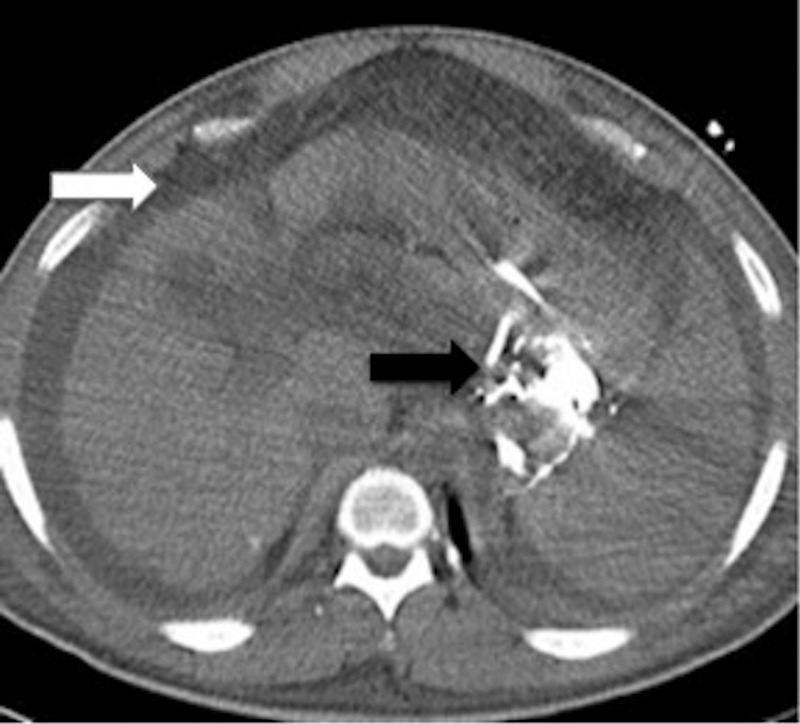
Non-contrast axial CT slice through the upper abdomen. Black arrow shows high-density cyanoacrylate material within splenorenal varices, and white arrow shows perihepatic ascites.
The exact rate of glue migration remains largely unknown. This is limited by the lack of routine postprocedural chest imaging or investigations for patients with mild hypoxaemia. There are very few studies analysing the risk factors for embolisation from glue injection. Hwang et al found that the volume of cyanoacrylate injected is associated with the risk of pulmonary embolism. In the retrospective study, 6 of 140 patients (4.3%) were given a mean volume of more than 4.2 mLs as compared to 1.8 mLs for those without pulmonary embolism. Four of the six patients were symptomatic from pulmonary embolism.29 Alexander et al reported volume and speed of injection and the size of gastric varices as risk factors for embolisation.13 Larger gastric varices have higher blood flow rates and are known to be associated with gastrorenal shunts predisposing them to pulmonary embolism. Irisawa et al concluded that altering the ratio of cyanoacrylate to lipiodol affects the rate at which the tissue adhesive polymerises; however, it remains difficult to prevent some migration beyond the bleeding varix.30 In the case reported here, the likely cause for pulmonary glue embolism was related to a combination of large volume cyanoacrylate injection used as well as the presence of large gastric varices with gastrorenal shunt.
Fatal and non-fatal cases of pulmonary glue embolism have been published worldwide. A spectrum of clinical presentations ranging from asymptomatic to sudden death has been reported so far. These included pleuritic chest pain, dyspnoea, cough, fever, tachycardia, hypoxia and cardiorespiratory arrest.2–4 13 14 17 18 20 21 24 When the patient is symptomatic, chest radiograph or non-contrast CT will aid the diagnosis. However, cyanoacrylate glue emboli are difficult to diagnose with CT pulmonary angiography as the intravenous contrast medium may mask the emboli. The onset of respiratory deterioration tends to occur minutes to hours after cyanoacrylate injection. In our patient, the deterioration was only apparent 10 days after the injection, which is rare. We hypothesise this could be because the stability of cyanoacrylate is different underventilated and filtered conditions in comparison to those patients without invasive organ support. The treatment for pulmonary glue embolism is supportive and there is no recognised role for anticoagulation or thrombolysis. Embolic consequences resolve with time by an unknown mechanism, as cyanoacrylate is not known to break down clots. Largely, symptomatic patients who survived were followed up with resolution of symptoms. Despite the clinical improvement, it has been noted that radiographic features of glue emboli can persist.13
Other alternative tissue adhesives available are fibrin glue and thrombin. Although less widely used, several studies have described good haemostatic results and are generally well tolerated.31–34 However, as with any blood product, potential adverse effects include anaphylaxis, antibody formation against fibrinogen and thrombin leading to coagulopathy and bleeding, and infectious disease transmission. Systemic embolisation may also occur due to inadvertent intra-arterial injection of fibrin glue or thrombin.12
Learning points.
Pulmonary glue embolism is rare but can be potentially fatal. As clinicians, it is important to have a high index of clinical suspicion in patients with unexpected cardiorespiratory deterioration during or after endoscopic procedure.
It is important to recognise that the onset of respiratory deterioration can be delayed.
It is possible that this complication is underdiagnosed in the asymptomatic or mildly symptomatic group of patients.
Consider alternative strategies of treatment for variceal bleeding in the critically ill patient with large varices requiring large volumes of sclerosant.
Acknowledgments
The authors would like to thank the team at John Farman Unit for looking after the patient.
Footnotes
Contributors: JRYC performed literature review and drafted the manuscript. AB edited images and revised the manuscript WG and JH were involved in the case and revised manuscript, JH revised manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hearnshaw SA, Logan RF, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 2011;60:1327–35 [DOI] [PubMed] [Google Scholar]
- 2.Palejwala AA, Smart HL, Hughes M. Multiple pulmonary glue emboli following gastric variceal obliteration. Endoscopy 2000;32:S1–2 [DOI] [PubMed] [Google Scholar]
- 3.Berry PA, Cross TJ, Orr DW. Clinical challenges and images in GI. Pulmonary embolization of histoacryl “glue” causing hypoxia and cardiovascular instability. Gastroenterology 2007;133:1413, 748 [DOI] [PubMed] [Google Scholar]
- 4.Habib SF, Muhammad R, Koulaouzidis A, et al. Pulmonary embolism after sclerotherapy treatment of bleeding varices. Ann Hepatol 2008;7:91–3 [PubMed] [Google Scholar]
- 5.Hamad N, Stephens J, Maskell GF, et al. Case report: thromboembolic and septic complications of migrated cyanoacrylate injected for bleeding gastric varices. Br J Radiol 2008;81:e263–5 [DOI] [PubMed] [Google Scholar]
- 6.Jalan R, Hayes PC. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. British Society of Gastroenterology. Gut 2000;46(Suppl 3–4):III1–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Scottish Intercollegiate Guidelines Network. Management of acute upper and lower gastrointestinal bleeding. A national clinical guideline. http://www.sign.ac.uk/pdf/sign105.pdf (accessed 2 Mar 2014)
- 8.de Franchis R. Revising consensus in portal hypertension: report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol 2010;53:762–8 [DOI] [PubMed] [Google Scholar]
- 9.National Institute for Health and Clinical Excellence. Acute upper gastrointestinal bleeding: management. http://www.nice.org.uk/guidance/cg141/resources/guidance-acute-upper-gastrointestinal-bleeding-management-pdf (accessed 2 Aug 2014)
- 10.Mahadeva S, Bellamy MC, Kessel D, et al. Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepatic portosystemic shunt in the management of acute gastric variceal bleeding. Am J Gastroenterol 2003;98:2688–93 [DOI] [PubMed] [Google Scholar]
- 11.Greenwald BD, Caldwell SH, Hespenheide EE, et al. N-2-butyl-cyanoacrylate for bleeding gastric varices: a United States pilot study and cost analysis. Am J Gastroenterol 2003;98:1982–8 [DOI] [PubMed] [Google Scholar]
- 12.Bhat YM, Banerjee S, Barth BA, et al. Tissue adhesives: cyanoacrylate glue and fibrin sealant. Gastrointest Endosc 2013;78:209–15 [DOI] [PubMed] [Google Scholar]
- 13.Alexander S, Korman MG, Sievert W. Cyanoacrylate in the treatment of gastric varices complicated by multiple pulmonary emboli. Intern Med J 2006;36:462–5 [DOI] [PubMed] [Google Scholar]
- 14.Ashraf P, Haqqi SA, Shaikh H, et al. Glue embolism: a rare cause of pulmonary embolism. JCPSP 2011;21:574–6 [PubMed] [Google Scholar]
- 15.Chang CJ, Shiau YT, Chen TL, et al. Pyogenic portal vein thrombosis as a reservoir of persistent septicemia after cyanoacrylate injection for bleeding gastric varices. Digestion 2008;78:139–43 [DOI] [PubMed] [Google Scholar]
- 16.Cheng PN, Sheu BS, Chen CY, et al. Splenic infarction after histoacryl injection for bleeding gastric varices. Gastrointest Endosc 1998;48:426–7 [DOI] [PubMed] [Google Scholar]
- 17.Javed A, Salamat A. N-butyl-2-cyanoacrylate and lipoidol pulmonary embolism (glue embolism). JAMC, Abbottabad 2008;20:143–5 [PubMed] [Google Scholar]
- 18.Kazi S, Spanger M, Lubel J. Education and imaging: gastrointestinal: pulmonary embolism of cyanoacrylate glue following endoscopic injection of gastric varices. J Gastroenterol Hepatol 2012;27:1874. [DOI] [PubMed] [Google Scholar]
- 19.Liu CH, Tsai FC, Liang PC, et al. Splenic vein thrombosis and Klebsiella pneumoniae septicemia after endoscopic gastric variceal obturation therapy with N-butyl-2-cyanoacrylate. Gastrointest Endosc 2006;63:336–8 [DOI] [PubMed] [Google Scholar]
- 20.Marion-Audibert AM, Schoeffler M, Wallet F, et al. Acute fatal pulmonary embolism during cyanoacrylate injection in gastric varices. Gastroenterol Clin Biol 2008;32:926–30 [DOI] [PubMed] [Google Scholar]
- 21.Rickman OB, Utz JP, Aughenbaugh GL, et al. Pulmonary embolization of 2-octyl cyanoacrylate after endoscopic injection therapy for gastric variceal bleeding. Mayo Clin Proc 2004;79:1455–8 [DOI] [PubMed] [Google Scholar]
- 22.Saracco G, Giordanino C, Roberto N, et al. Fatal multiple systemic embolisms after injection of cyanoacrylate in bleeding gastric varices of a patient who was noncirrhotic but with idiopathic portal hypertension. Gastrointest Endosc. 2007;65:345–7 [DOI] [PubMed] [Google Scholar]
- 23.Shim CS, Cho YD, Kim JO, et al. A case of portal and splenic vein thrombosis after Histoacryl injection therapy in gastric varices. Endoscopy 1996;28:461. [DOI] [PubMed] [Google Scholar]
- 24.Singer AD, Fananapazir G, Maufa F, et al. Pulmonary embolism following 2-octyl-cyanoacrylate/lipiodol injection for obliteration of gastric varices: an imaging perspective. J Radiol Case Rep 2012;6:17–22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tan YM, Goh KL, Kamarulzaman A, et al. Multiple systemic embolisms with septicemia after gastric variceal obliteration with cyanoacrylate. Gastrointest Endosc 2002;55:276–8 [DOI] [PubMed] [Google Scholar]
- 26.Wahl P, Lammer F, Conen D, et al. Septic complications after injection of N-butyl-2-cyanoacrylate: report of two cases and review. Gastrointest Endosc 2004; 59:911–16 [DOI] [PubMed] [Google Scholar]
- 27.Wright G, Matull WR, Zambreanu L, et al. Recurrent bacteremia due to retained embolized glue following variceal obliteration. Endoscopy 2009;41(Suppl 2): E56–7 [DOI] [PubMed] [Google Scholar]
- 28.Yu LK, Hsu CW, Tseng JH, et al. Splenic infarction complicated by splenic artery occlusion after N-butyl-2-cyanoacrylate injection for gastric varices: case report. Gastrointest Endosc 2005;61:343–5 [DOI] [PubMed] [Google Scholar]
- 29.Hwang SS, Kim HH, Park SH, et al. N-butyl-2-cyanoacrylate pulmonary embolism after endoscopic injection sclerotherapy for gastric variceal bleeding. J Comput Assist Tomogr 2001;25:16–22 [DOI] [PubMed] [Google Scholar]
- 30.Matsumoto A, Takimoto K, Inokuchi H. Prevention of systemic embolization associated with treatment of gastric fundal varices. Mayo Clin Proc 2005; 80:705. [DOI] [PubMed] [Google Scholar]
- 31.Datta D, Vlavianos P, Alisa A, et al. Use of fibrin glue (beriplast) in the management of bleeding gastric varices. Endoscopy 2003;35:675–8 [DOI] [PubMed] [Google Scholar]
- 32.Przemioslo RT, McNair A, Williams R. Thrombin is effective in arresting bleeding from gastric variceal hemorrhage. Dig Dis Sci 1999;44:778–81 [DOI] [PubMed] [Google Scholar]
- 33.Ramesh J, Limdi JK, Sharma V, et al. The use of thrombin injections in the management of bleeding gastric varices: a single-center experience. Gastrointest Endosc 2008;68:877–82 [DOI] [PubMed] [Google Scholar]
- 34.Yang WL, Tripathi D, Therapondos G, et al. Endoscopic use of human thrombin in bleeding gastric varices. Am J Gastroenterol 2002;97:1381–5 [DOI] [PubMed] [Google Scholar]