

Description
Sialolithiasis is a pathological disease involving the major salivary glands and their ducts. More than 80% of sialoliths occur in the submandibular gland, 4–10% in the parotid gland and 17% in minor salivary glands. Among the minor salivary glands, the most common locations are upper lip (49.2%), inner aspect of cheeks (37.3%), lower lip (5.5%), vestibule (4.7%), palate and tongue (1.6%).1 2 However, the presence of a sialolith in palatal minor salivary glands is extremely rare. Only two to three cases have been reported in the literature during 1970–1980.3
A 26-year-old man presented to the department with difficulty in swallowing and pain in the throat region of 1 month duration. On palpation, presence of a firm swelling on the mucosal surface of the soft palate was discovered. The patient also had limited tongue movement as the mass pressed against it. Clinical examination revealed the presence of a firm swelling in the left posterolateral area of the soft palate (figure 1). Occlusal and lateral oblique radiographs were taken and appeared normal. A differential diagnosis of tonsilolith or peritonsillar abscess (Quinsy) was performed.
Figure 1.

Preoperative view of the sialolith in the posterolateral area of the soft palate.
The surgical site was prepared with antiseptic solution and transoral sialolithotomy was performed. The sialolith was oval and hard in consistency measuring approximately 0.5 cm in diameter and 1.7 cm in length (figure 2).
Figure 2.
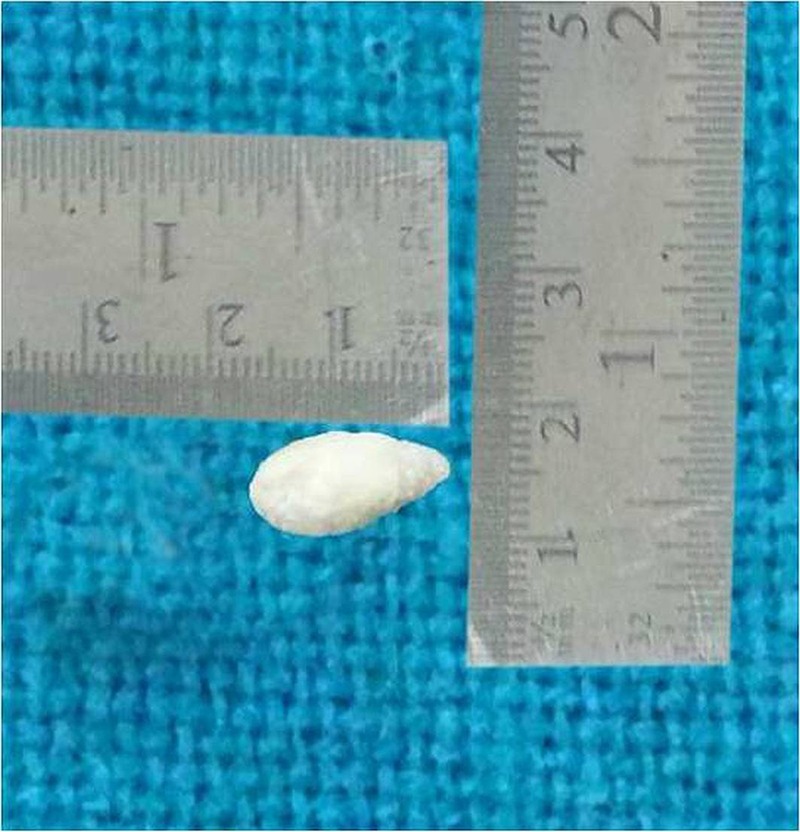
Excised calcified mass measuring approximately 1.7 cm×0.8 cm.
Histopathological examination of the specimen revealed a calcified mass exhibiting a lamellated appearance with alternating eosinophilic and basophilic bands, with a more homogeneous central part, indicative of a sialolith (figure 3). Regular follow-up was maintained and the surgical site healed properly without any postoperative recurrence or complications (figure 4).
Learning points.
Occurrence of sialoliths in major salivary glands/ducts is not unusual. They frequently involve submandibular and parotid followed by sublingual salivary glands. However, although the incidence of a sialolith in minor salivary glands is very rare, suspicion should be entertained, as in our case.
We present a rare case of a sialolith in the posterolateral area of the soft palate, which is unique in terms of its location. Routine radiographic examination in such cases is not possible because of the location, however, CT scan/MRI may aid in the diagnosis; however, they are expensive. In our case, we confirmed the diagnosis of sialolith based on histopathological examination.
Figure 3.
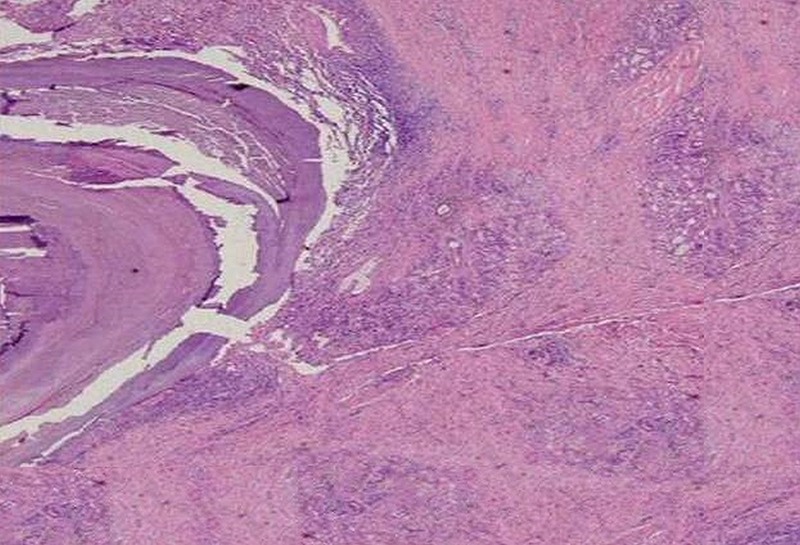
Histopathological view demonstrating the lamellar pattern of excised mass (40×).
Figure 4.

Postoperative view of the surgical site.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Lagha NB, Alantar A, Samson J, et al. Lithiasis of minor salivary glands: current data. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:345–8 [DOI] [PubMed] [Google Scholar]
- 2.Tanda N, Echigo S, Teshima T. Sialolithiasis of a Blandin's gland duct. Int J Oral Maxillofac Surg 1988;17:78–80 [DOI] [PubMed] [Google Scholar]
- 3.Anneroth G, Hansen LS. Minor salivary gland calculi: a clinical and histopathological study of 49 cases. Int J Oral Surg 1983;12:80–9 [DOI] [PubMed] [Google Scholar]