

Abstract
A case of sublingual epidermoid cyst presenting distinctive magnetic resonance imaging (MRI) findings is described. A 39-year-old man presented to our hospital with a three months progressive left submandibular swelling, difficulty moving his tongue, and snoring. Preoperative evaluation with MRI and fine needle aspiration cytology (FNAC) revealed that the heterogeneous cystic lesion contained the squamous cells, which is compatible with ectodermal tissue. The mass was located above the mylohyoid muscle and spread to the pharyngeal space. By considering the size, infection history, patient age, and location, the cyst was completely resected under general anesthesia via cervical approach without any complication. Histopathologically, the cyst wall was lined by stratified squamous epithelium with no skin appendage, suggesting an epidermoid cyst. Ultrasound (US), MRI and FNAC were very useful of the preoperative diagnosis for oral and sublingual lesion. The postoperative course was uneventful and without recurrence after 24 months. This case showed that epidermoid cysts formed the rarely heterogeneous cystic tumor and it underlined usefulness of preoperative diagnosis, such as US, MRI and FNAC for oral and sublingual tumor.
Key words: Epidermoid cyst, sublingual, oral floor, magnetic resonance imaging
Introduction
The most frequent cystic lesions occurring in the oral floor are benign, including ranulas associated with the sublingual glands, lymphangioma, hemangioma, and dermoid cysts of ectodermal origin. Dermoid cysts originating in the oral floor constitutes only 1-2% of all dermoid cysts.
Surgical excision has been the accepted first line therapy for cysts in the oral floor. Recently OK-432 has been used to treat cystic lesion with thin epithelia such as the head and neck, because it is less invasive treatment. Magnetic resonance imaging (MRI), computed tomography (CT), ultrasonography (US), and fine needle aspiration cytology (FNAC) are useful and increasingly important for making a preoperative diagnosis and determining therapeutic strategy. We present the case of a patient with a large sublingual epidermoid cyst presenting with distinctive MRI findings. This patient was successfully treated with a small cervical skin incision, without any complications.
Case Report
A 39-year-old man presented to our hospital with a 3-month history of progressive submandibular swelling, difficulty moving his tongue, and snoring. He had been aware of a swelling of the oral floor for 4 years. Over the previous year, he had been experiencing a bitter taste from the oral floor.
On presentation, the patient had marked swelling of the left oral floor and swelling of the left submandibular region. The oral floor mucosa was not eroded. An elastic mass suspicious for cystic tumor was palpated from the oral cavity. The cyst wall was slightly thickened and covered with mucosa. The vocal cord moved well, but the left tongue base was swollen and reduced the pharyngeal airway space. A 10.0×6.5 cm tumor was palpated in the left submandibular region. No facial palsy was observed.
MRI showed a 9.5×7.0×5.0 cm heterogeneous tumor with low intensity on T1-weighted image and high intensity on T2-weighted image (Figure 1A, B). The tumor was located above the mylohyoid muscle and spread to the pharyngeal space. FNAC of the tumor contents revealed enucleated squamous cells and inflammatory cells, with no malignant cells present. A diagnosis of dermoid or epidermoid tumor of heterogeneous viscosity was made.
Figure 1.
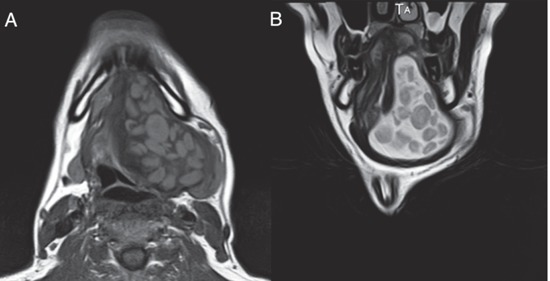
Preoperative magnetic resonance imaging. A) Axial section showing heterogeneous components in the cystic lesion (T1-weighted image). B) Coronal section showing spread of the cystic lesion from the oral floor to the pharyngeal space, with heterogeneous components (T2-weighted image).
Tumor excision was performed under general anesthesia with right nasotracheal intubation to allow intra-oral surgical manipulation and postoperative respiration control in the event of airway swelling. A 4.5 cm horizontal skin incision was made 2.5 cm below the edge of the mandible to preserve and prevent damage to the mandibular branch of the facial nerve. The skin and subcutaneous tissues were elevated toward the head just under the platysma muscle. Tumor resection was performed from anterior to posterior. The facial vein penetrated the tumor and was ligated. The tumor extended to the oral floor, the midline of the tongue base, and adhered to the submandibular gland posterolaterally. The submandibular lymph node was not swollen. The tumor was separated from the mandible and the oral floor mucosa. The tumor with attached submandibular gland was completely resected (Figure 2A). The nasotracheal tube was removed after confirming adequate airway space with little swelling of the tongue base by endoscopic fiberscope. No facial palsy, bleeding, or tongue discomfort were observed post-operatively.
Figure 2.
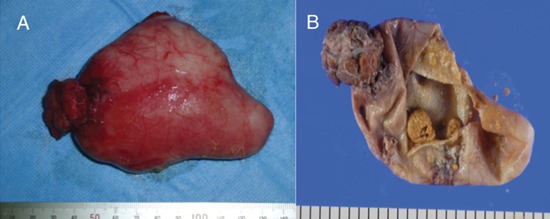
Surgical specimen. A) Lateral view of the cyst. B) Cross-section of the cyst. The cystic tumor comprised brown secretory material and a dark brown firm mass.
The tumor was sectioned and comprised brown secretory contents and a dark brown firm mass without any skin appendage (Figure 2B). The resected tumor was 9.5×8.0×4.0 cm. Histopathology confirmed an epidermoid cyst lined with squamous cells without any skin adnexa (Figure 3).
Figure 3.
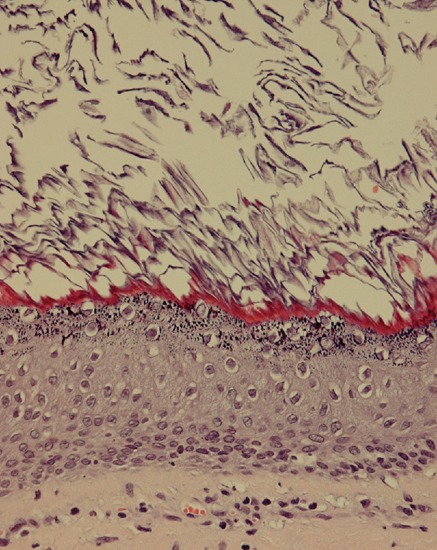
Histopathological findings. The wall of the cyst was lined with squamous cells without any skin appendage (hematoxylin and eosin ×400).
Discussion
Cystic tumors in the oral floor have been reported, including ranulas originating from the sublingual glands,1 lymphangioma, dermoid cysts, epidermoid cysts, and midline cervical cysts.2
Dermoid cysts originating in the oral floor constitutes only 1-2% of all dermoid cysts.3 Dermoid and epidermoid cysts in the oral cavity develop in the midline or sublingual region of the oral floor.4-9 Dermoid cysts are formed by the congenital enclosure of ectodermal tissue, and clinical symptoms generally begin when patients are 15 to 35 years of age. Tumors of ectodermal origin are classified by their contents. Dermoid cysts are broadly classified into three subtypes by histological findings: dermoid, epidermoid, and teratoid. The dermoid cysts contain skin adnexa in the epithelial wall, epidermoid cysts are lined only with epithelium, and teratoid cysts contain other tissues, such as muscle, cartilage, and bone, within the cavity.10
Surgical excision has been the accepted standard therapeutic strategy for cystic tumors in the oral floor. OK-432, which is a lyophilized streptococcal preparation made from the Su strain of A-group Streptococcus pyogenes, has recently been reported as an alternative therapy to surgical excision, and is now the first line treatment for lymphangioma.11 Because OK-432 therapy causes inflammation in the thin epithelium, leading to adhesion of the cyst wall, it is indicated for the treatment of cysts with thin epithelia such as ranulas, lymphangiomas, and salivary mucoceles. A high success rate (over 96%) has been reported in the treatment of ranulas with OK-432.12 OK-432 has been less effective in treating cysts with thicker walls and squamous epithelium such as dermoid cysts, epidermoid cysts, and branchial cleft cysts. Therefore, a preoperative diagnosis is important when deciding whether excision or OK-432 is the best therapy. In this case, the complete resection was more suitable than OK-432 therapy because of preoperative diagnosis presenting the epidermoid cyst.
CT, MRI, US, and FNAC are useful tools for the preoperative diagnosis of cystic masses in the oral floor. MRI yields more tumor information than CT, and US has also been reported to provide information about tumor contents.13,14 With MRI, the contents of cystic tumors usually appear homogeneous, presenting low T1 and high T2 intensity, depending on the concentration of protein and mucin in the cyst. FNAC gives important preoperative diagnostic information. Ranulas and lymphangiomas do not contain epithelial cells. The presence of squamous cells on FNAC rules out the possibility of a ranula, which may effectively be treated by OK-432 therapy.
Dermoid cysts are usually located on the midline, while this cyst originated on the left side of the oral floor and spread to the pharyngeal space.4,15 Heterogeneous contents have been reported in dermoid cysts, which contain skin adnexa in the cyst wall,16 while epidermoid cysts have not been reported to show such heterogeneity on MRI. The two different viscosity components in the cyst in this case both had acellular histological findings.
The treatment for dermoid and epidermoid cysts is total resection. The topographic relationship between the mylohyoid muscle and the cyst determines the approach of the resection: orally or through a cervical skin incision.
The mylohyoid muscle separates the sublingual space from the submental and submandibular spaces. Tumors above the mylohyoid muscle can be resected by the intraoral approach, whereas those below the mylohyoid muscle and large tumors with spread to the pharyngeal space can be approached via a cervical skin incision.17,18 In this case a 4.5 cm cervical skin incision was selected, because the tumor measured over 10 cm and extended to the upper and lower aspects of the mylohyoid muscle. The epidermoid cyst was completely removed with no oral mucosa defect and no complications. Gentle surgical handling enabled complete removal with a small incision. Repeated infections cause severe adhesions of tumor to surrounding tissues. Therefore, the surgical approach should be selected by considering tumor size, infection history, patient age, and tumor location.
Conclusions
Only 1 to 2% of all dermoid cysts arise in the sublingual region. FNAC and MRI findings were useful in the present case for showing that the tumor characteristics and extension to the pharyngeal space with a smooth margin presenting the ectodermal origin tumor. OK-432 has been less effective in treating cysts for thicker walls with squamous epithelium such as dermoid or epidermoid cysts. Surgical complete resection with small incision is useful for treatment in epidermoid cyst extended to the upper and lower aspects of the mylohyoid muscle in the oral floor.
References
- 1.Harrison JD, Garrett JR. Mucocele formation in cats by glandular duct ligation. Arch Oral Biol 1972;17:1403-14 [DOI] [PubMed] [Google Scholar]
- 2.Batsakis JG, McClatchey KD. Cervical ranulas. Ann Otol Rhinol Laryngol 1988;97: 561-2 [DOI] [PubMed] [Google Scholar]
- 3.Meyer I. Dermoid cysts of the floor of the mouth. Oral Surg 1955;8:1149-64 [DOI] [PubMed] [Google Scholar]
- 4.King RC, Smith BR, Burk JL. Dermoid cyst in the floor of the mouth. Review of the literature and case reports. Oral Surg Oral Med Oral Pathol 1994;78:567-76 [DOI] [PubMed] [Google Scholar]
- 5.Rosen D, Wirtschafter A, Rao VM, Wilcox TO., Jr.Dermoid cyst of the lateral neck: a case report and literature review. Ear Nose Throat J 1998;77:125-32 [PubMed] [Google Scholar]
- 6.Görür K, Talas DU, Ozcan C. An unusual presentation of neck dermoid cyst. Eur Arch Otorhinolaryngol 2005;262:353-5 [DOI] [PubMed] [Google Scholar]
- 7.Mandel L, Surattanont F. Lateral dermoid cyst. J Oral Maxillofac Surg 2005;63:137-40 [DOI] [PubMed] [Google Scholar]
- 8.Mathews J, Lancaster J, O’Sullivan G. True lateral dermoid cyst of the floor of the mouth. J Laryngol Otol 2001;115:333-5 [DOI] [PubMed] [Google Scholar]
- 9.Masliah MK, Blain S, Sanders B. Dermoid cysts of the oral region in children. J Pedod 1979;3:221-34 [PubMed] [Google Scholar]
- 10.New GB, Erich JB. Dermoid cysts of the head and neck. Surg Gynecol Obstet 1937;65:48-55 [Google Scholar]
- 11.Ogita S, Tsuto T, Tokiwa K, Takahashi T. lntracystic injection of OK-432: a new sclerosing therapy for hygroma in children. Br J Surg 1987;74: 690-1 [DOI] [PubMed] [Google Scholar]
- 12.Ohta N, Fukase S, Suzuki Y, et al. Treatments of various otolaryngological cystic diseases by OK-432: its indications and limitations. Laryngoscope 2010;120: 2193-6 [DOI] [PubMed] [Google Scholar]
- 13.Vogl TJ, Steger W, Ihrler S, et al. Cystic masses in the floor of the mouth: value of MR imaging in planning surgery. AJR Am J Roentgenol 1993;161:183-6 [DOI] [PubMed] [Google Scholar]
- 14.Kutuya N. A case of dermoid cyst of the floor of the mouth: ultrasonography was more useful than computed tomography and magnetic resonance imaging in the preoperative diagnosis. J Med Ultrasonics 2009;36:27-31 [DOI] [PubMed] [Google Scholar]
- 15.Walstad WR, Solomon JM, Schow SR, Ochs MW. Midline cystic lesion of the floor of the mouth. J Oral Maxillofac Surg 1998; 56:70-4 [DOI] [PubMed] [Google Scholar]
- 16.Ikeda K, Koseki T, Maehara M, et al. Hourglass-shaped sublingual dermoid cyst: MRI features. Radiat Med 2007;25: 306-8 [DOI] [PubMed] [Google Scholar]
- 17.Seward GR. Dermoid cysts of the floor of the mouth. Br J Oral Surg 1965;3:36-47 [DOI] [PubMed] [Google Scholar]
- 18.Leveque H, Saraceno CA, Tang CK, Blanchard CL. Dermoid cysts of the floor of the mouth and lateral neck. Laryngoscope 1979;89:296-305 [DOI] [PubMed] [Google Scholar]